
Abstract
The purpose of this study is to evaluate the value of distal spinal accessory nerve (SAN) transfer to the suprascapular nerve (SSN) in children with brachial plexus birth injuries in order to better define the application and outcome of this transfer in these infants. Over a 3-year period, 34 infants with brachial plexus injuries underwent transfer of the SAN to the SSN as part of the primary surgical reconstruction. Twenty-five patients (direct repair, n=20; interposition graft, n=5) achieved a minimum follow-up of 24 months. Fourteen children underwent plexus reconstruction with SAN-to-SSN transfer at less than 9 months of age, and 11 underwent surgical reconstruction at the age of 9 months or older. Mean age at the time of nerve transfer was 11.6 months (range, 5–30 months). At latest follow-up, active shoulder external rotation was measured in the arm abducted position and confirmed by review of videos. The Gilbert and Miami shoulder classification scores were utilized to report shoulder-specific functional outcomes. The effects of patient age at the time of nerve transfer and the use of interpositional nerve graft were analyzed. Overall mean active external rotation measured 69.6°; mean Gilbert score was 4.1 and the mean Miami score was 7.1, corresponding to overall good shoulder functional outcomes. Similar clinical and shoulder-specific functional outcomes were obtained in patients undergoing early (<9 months of age, n=14) and late (>9 months of age, n=11) SAN-to-SSN transfer and primary plexus reconstruction. Nine patients (27%) were lost to follow-up and are not included in the analysis. Optimum results were achieved following direct transfer (n=20). Results following the use of an interpositional graft (n=5) were rated satisfactory. No patient required a secondary shoulder procedure during the study period. There were no postoperative complications. Distal SAN-to-SSN (spinoscapular) nerve transfer is a reliable option for shoulder reinnervation in infants with brachial plexus birth injuries. Direct transfer seems to be the optimum method. The age of the patient does not seem to significantly impact on outcome.
Introduction
Interest in the use of selective nerve transfers in the surgical reconstruction of brachial plexus birth injuries continues to emerge. Specifically, the spinal accessory nerve (SAN) transfer to the suprascapular nerve (SSN; spinoscapular nerve transfer) in infants with brachial plexus birth injuries is an attractive reconstructive option for restoration of shoulder stability and active external rotation given the accessory nerve's extraplexal origin and proximity to the upper trunk and SSN. The purpose of this study is to evaluate the value of distal SAN transfer to the SSN in children with brachial plexus birth injuries in order to better define the application and outcome of this spinoscapular nerve transfer in this patient population.
Methods
Over a 3-year period (2003–2006), 34 infants (15 male, 19 female) underwent reconstruction of a brachial plexus birth injury that included transfer of the distal spinal accessory nerve into the suprascapular nerve as part of the primary surgical reconstruction performed by a single surgeon (JAIG). The majority of patients also underwent reconstruction of the upper trunk (anterior and posterior divisions) using sural nerve grafts from C5 and/or C6. No other nerve transfer was performed in any child. No surgery was performed on the long thoracic nerve in any patient. In 26 patients, a direct repair was performed, and in eight patients, a short interpositional nerve graft was utilized to bridge a gap between the two nerve ends (mean graft length, 2.5 cm). At the time of surgical intervention, the brachial plexus injury pattern subcohorts included C5-C6 (n=16), C5-C6-C7 (n=5), and global (n=13). The right upper limb was involved in 21 patients and the left in 13 patients. The outcome analysis was based on the 25 patients followed for at least 24 months.
Operative Technique
The SAN to SSN (spinoscapular nerve) transfer has evolved into our procedure of choice for suprascapular nerve reconstruction because of the success of direct nerve transfers. This frees up additional spinal nerve donors for grafting. The entire procedure is performed using the operating microscope. The SAN is identified in the posterior cervical triangle behind the greater auricular nerve and beneath the sternocleidomastoid muscle. The SAN is then confirmed by direct stimulation to distinguish it from cervical plexus branches. Under direct vision, the SAN is traced distally beyond its branches to the middle and lower trapezius (Fig. 1a). Near the final bifurcation or trifurcation, large branches from the transverse cervical vessels are encountered which must be carefully divided. The nerve is then reconfirmed by stimulation and divided as distal as possible and elevated superiorward to join the suprascapular nerve. The level of division of the suprascapular nerve is selected based upon serial intraoperative frozen section histopathological analyses of the resected nerve segment. A tension-free direct end-to-end repair technique is performed outside the zone of injury using fibrin glue (Fig. 1b).
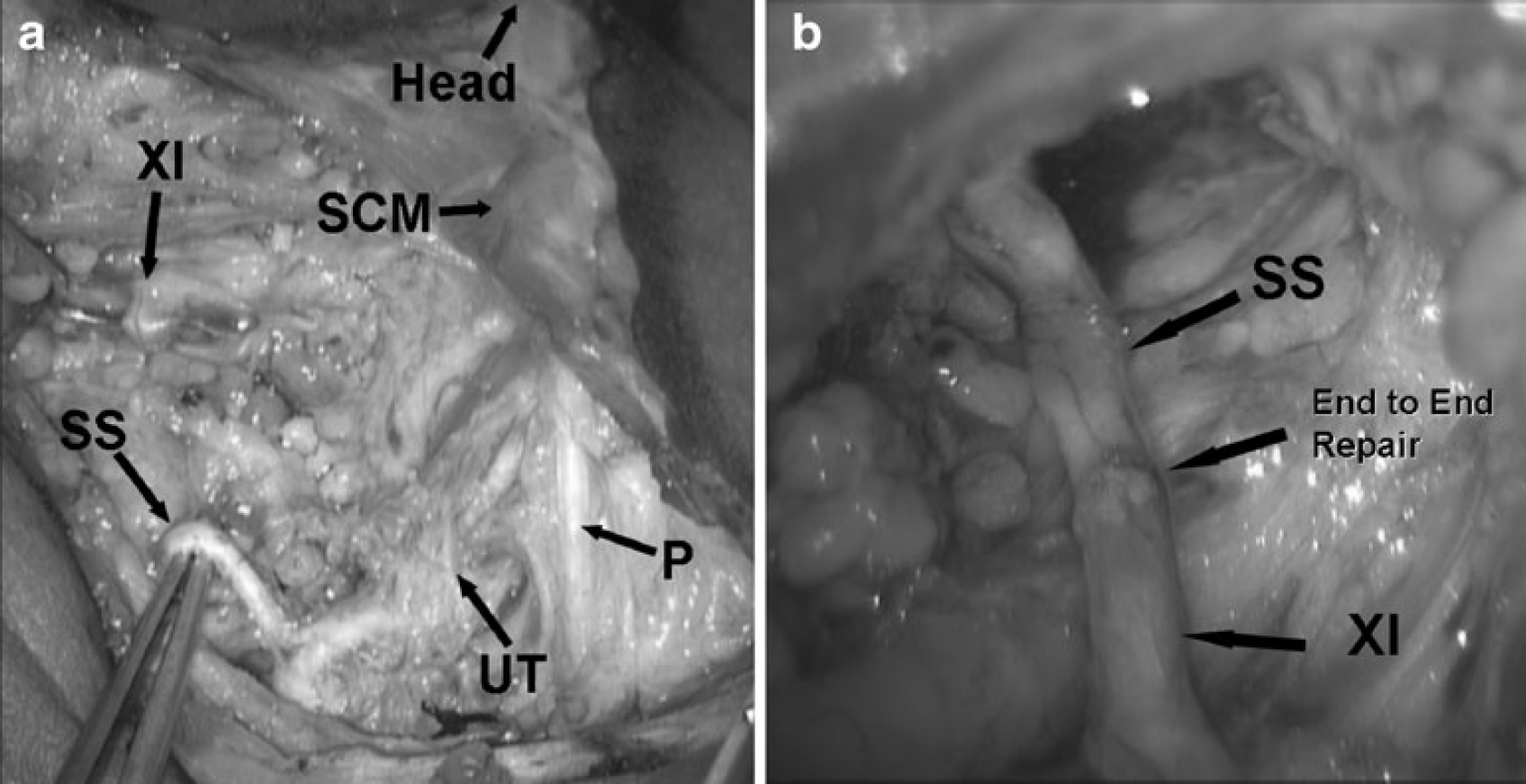
Intraoperative views.
At the time of the SAN to SSN transfer, all patients received botulinum toxin type-A injections into the pectoralis major (50 units) and the latissimus dorsi/teres major (50 units). Postoperatively, all children were immobilized in a modified shoulder spica cast for 2 weeks if plexus reconstruction was performed in isolation or 6 weeks if an associated shoulder contracture release was performed concomitantly (n=14). At the time of cast removal, occupational therapy and functional electrical muscle stimulation were initiated.
Twenty-five of 34 (74%) patients were available for follow-up at a minimum of 24 months postoperatively. Nine patients (27%) were lost to follow-up. A direct repair was performed in 20 infants, and an interpositional graft was required in five cases. Mean age at the time of nerve transfer was 11.6 months (range, 5–30 months). The need for a graft resulted from the necessity to do more extensive neuroma resection or because the suprascapular nerve lacked the usual redundancy.
From [7]
Fourteen of 34 (41%) of infants underwent simultaneous reconstruction of a shoulder internal rotation contracture. Our indications to perform a concomitant release of a shoulder contracture at the time of brachial plexus reconstruction include inability to obtain full passive external rotation of the shoulder when the upper limb is adducted at the patient's side and the elbow flexed or if there is joint instability. In the cohort of children who underwent plexus reconstruction and SAN-to-SSN transfer at less than 9 months of age (n=14), two underwent concomitant subscapularis slide and one underwent tenotomy of the pectoralis major. In the group who underwent surgery at the age of 9 months or older (n=11), three subscapularis slides were performed in isolation, and two slides were performed in conjunction with glenohumeral capsuloplasty. In the nine children with less than 2-year follow-up, three underwent subscapularis slide and three underwent subscapularis slide with capsuloplasty.
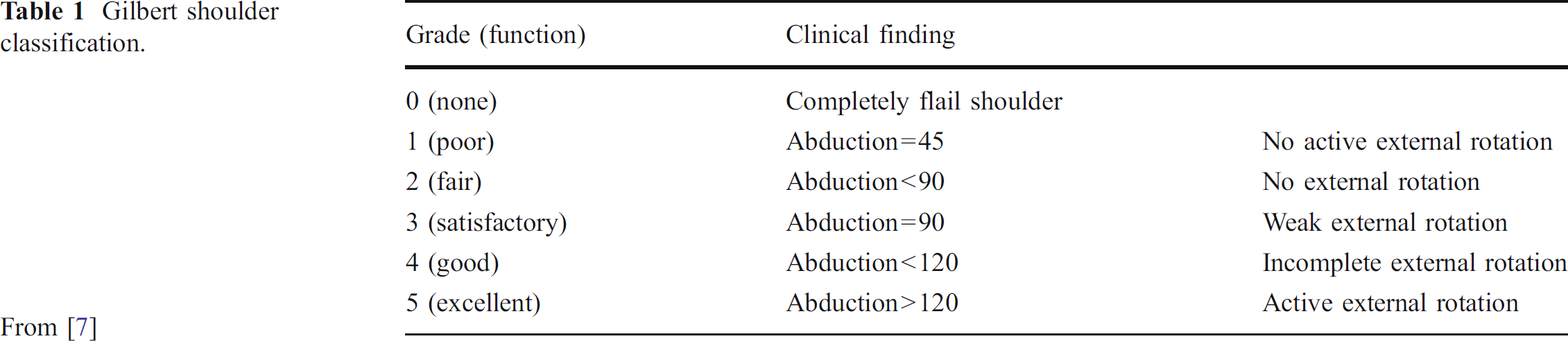
At the latest follow-up, clinical and functional outcomes were evaluated. Active shoulder external rotation was measured and confirmed by a review of videos obtained at each evaluation. Shoulder-specific functional outcome was evaluated with the Gilbert (Table 1) [5] and the Miami shoulder classification scores (Table 2) [7]. The effects of age at the time of nerve transfer and the use of interpositional nerve graft on outcome were analyzed.
Gilbert shoulder classification.
Miami shoulder classification.
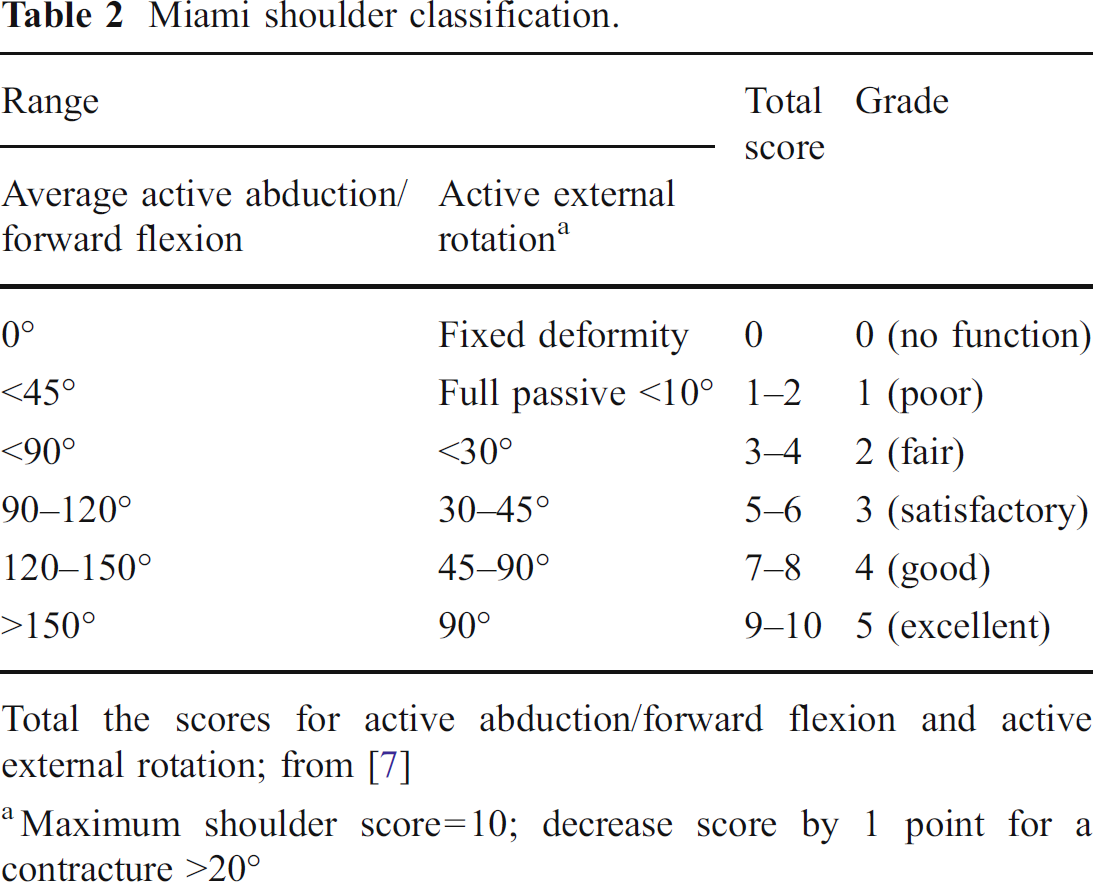
Total the scores for active abduction/forward flexion and active external rotation; from [7]
Maximum shoulder score=10; decrease score by 1 point for a contracture >20°
Results
At a minimum of 24 months follow-up, overall mean active external rotation measured 69.6°; the mean Gilbert score was 4.1 and the mean Miami score was 7.1, which corresponds to a good overall shoulder functional outcome on both scales. Subcohort analysis demonstrated that patients operated on at the age of 9 months or less (n=14) obtained a mean 70.3° of active external rotation, a mean Gilbert score of 4.2, and a mean Miami score of 7.4. Patients who underwent nerve transfer at greater than 9 months (n=11) of age achieved similar results with a mean 62.3° of active external rotation, a mean Gilbert score of 4.0, and a mean Miami score of 7.4 (Table 3).
Effect of patient age at time of transfer on clinical and functional outcome.
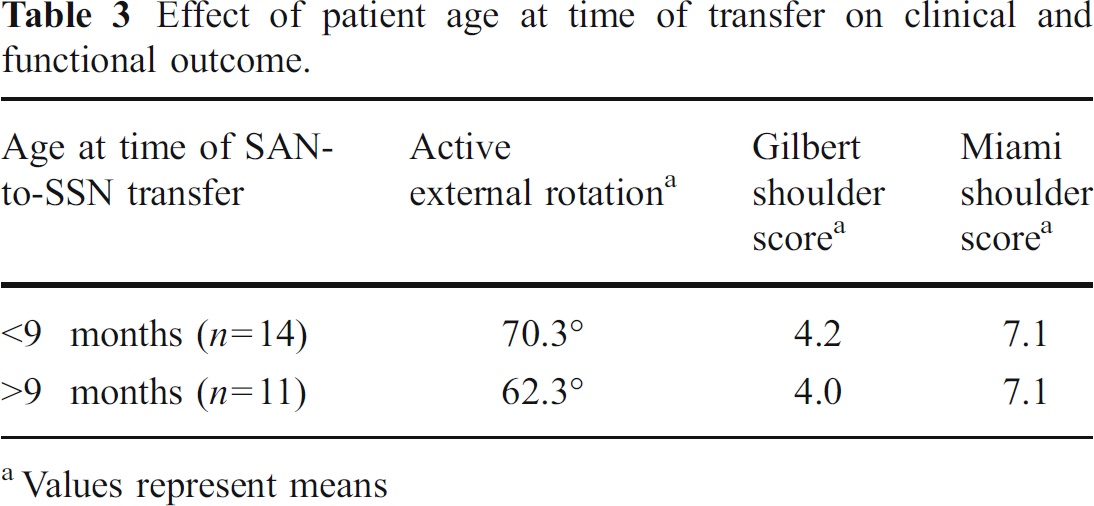
Values represent means
No patient underwent a secondary shoulder procedure during the study period. There were no postoperative complications and no evidence of trapezius atrophy/weakness on examination at latest follow-up. Although the majority of children underwent nerve conduction studies as part of the diagnostic protocol, no postoperative studies were performed in any child.
Discussion
Transfer of the distal spinal accessory nerve into a variety of recipients is commonly used in the surgical reconstruction of adult upper brachial plexus traction injuries [1–3,12,16,21]. Following the description of Kawabata and colleagues [9] of the use of the spinal accessory nerve as an ipsilateral nerve transfer to the suprascapular nerve in infants with upper brachial plexus birth injuries, its use has continued to expand.
Several groups [1,6,8,11,14,19,20] have published variable experiences with the use of the distal SAN-to-SSN transfer as part of a primary or secondary plexus reconstruction in infants who fail to demonstrate spontaneous recovery of active shoulder external rotation following a period of observation. In a retrospective review of 86 infants, Pondaag et al. [14] found similar clinical results and functional scores in infants undergoing C5-to-SSN bypass grafting (n=65) and those who received direct SAN-to-SSN (n=21) transfers performed at a mean of 5 months of age. Overall, functional outcomes as measured by the Mallet hand–mouth and hand–head scores for the cohort were superior to overall objective external glenohumeral rotation obtained at latest follow-up. Only 17 of 86 patients achieved more than 20° of external rotation. These data suggested that compensatory mechanisms play a significant role in allowing these children to obtain functional improvements in the involved upper limb independent of reconstructive strategy.
van Ouwerkerk and colleagues [20] reported promising results in 54 children following isolated SAN to SSN transfers performed as a primary (n=47) or secondary (n=7) procedure at a mean of 21 months of age (range, 6–84 months) in children without return of active shoulder external rotation. Thirty-nine of 54 patients achieved more than 20° of active external rotation by 4 months postoperatively, and the mean magnitudes were similar in children undergoing the transfer before and after 12 months of age. These data highlight the issue of the optimal timing of surgery for reinnervation of the shoulder. In this study, clinical and functional outcomes were similar when the transfer was performed prior to or following 9 months of age in this series.
A small subcohort of infants (n=8) in this series required an interpositional graft between the SAN and SSN nerve ends. Five of these children, at a minimum of 2-year follow-up, achieved a mean of 48° of active external rotation and a satisfactory shoulder-specific functional outcome. Given the small size of this subcohort, it is difficult to make a definitive statement comparing these results to those seen following direct transfer and end-to-end repair. While these results represent a 25% reduction in outcome compared to children with a direct repair, these children did obtain results comparable to the outcomes we have reported following partial SAN transfer into the suprascapular nerve using a proximal end-to-side technique with cervical plexus or reversed sural nerve grafts [6].
In the current series, all children received botulinum toxin type-A injections into the pectoralis major and the latissimus dorsi/teres major at the time of the primary plexus reconstruction. Use of botulinum toxin in this setting has been shown to reduce the incidence and severity of recurrent internal rotation contracture of the shoulder following a subscapularis slide [15]. Additionally, the performance of a simultaneous shoulder reconstruction for internal rotation contracture in 14 of the patients may have contributed to the magnitude of external rotation achieved.
The primary endpoint of the current study was active shoulder external rotation. This parameter was measured with the child standing. It continues to remain challenging to isolate the infraspinatus from potentially recovering axillary nerve innervated external rotators (posterior deltoid and teres minor) in this patient population.
The spinal accessory nerve constitutes an attractive ipsilateral donor to the suprascapular nerve in order to restore shoulder function in infants as it is an extraplexal pure motor nerve that lies in close proximity to the upper trunk and suprascapular nerve potentially allowing for direct coaption without the need for an interposition nerve graft. Variable motor innervation patterns of the trapezius and differential contributions from the spinal accessory nerve and cervical plexus (C2 and C3) motor branches to the transverse and ascending portions of the trapezius [4,8,10,13,17,18] limit mobilization of the spinal accessory nerve to its distal portion in order to ensure residual trapezial function following the transfer. Our group [6] has previously reported Grade 4 or better shoulder function in 26 infants undergoing partial transfer of the spinal accessory nerve into the suprascapular nerve using an interpositional reversed nerve graft (sural or cervical plexus sensory) and a modified end-to-side technique at the proximal end.
Spinoscapular nerve transfer appears to offer promising, reproducible clinical and functional results in select infants. Direct transfer seems to be the optimum method, and the age of the patient at the time of the transfer does not seem to significantly impact on outcome within the time frame of this study group. Shoulder function following use of an interpositional graft appears comparable to outcomes seen following partial SAN transfer performed with an end-to-side technique at the proximal end. Prospective series with larger cohorts, nonoperative and operative control groups, and long-term follow-up are necessary to continue to establish optimal treatments for children with brachial plexus birth palsy requiring primary surgical reconstruction.