
Abstract
The use of end-to-side neurrorhaphy remains a controversial topic in peripheral nerve surgery. The authors report the long-term functional outcome following a modified end-to-side motor reinnervation using the spinal accessory to innervate the suprascapular nerve following a C5 to C6 avulsion injury. Additionally, functional outcomes of an end-to-end neurotization of the triceps branch to the axillary nerve and double fascicular transfer of the ulnar and medial nerve to the biceps and brachialis are presented. Excellent functional recoveries are found in respect to shoulder abduction and flexion and elbow flexion.
Introduction
The use of end-to-side neurorrhaphy remains a controversial topic in peripheral nerve surgery. The premise of end-to-side neurorrhaphy is reinnervation of an injured recipient nerve by collateral sprouting from an intact donor nerve. Recent work has primarily focused upon mechanisms to induce collateral sprouting from the donor nerve and the interactions of sprouting axons with basal laminar layers [5,10,12,13,15,28,29,35]. Most authors would agree that end-to-side coaptation is not an ideal strategy for optimal reinnervation when other options exist; yet, in the appropriate setting (e.g., reinnervation of noncritical sensory deficits), good results can be obtained. An increased utilization and understanding of the potential of nerve transfers has facilitated improved patient outcomes [7,16,18,21,22,30]. Despite these results, nerve transfers are not always feasible and do carry some risk for loss of function to the donor nerve and muscle. End-to-side neurorrhaphy is useful in large nerve gaps or in injuries where the proximal stump of the injured nerve is unavailable. Autografting may be necessary when dissection cannot expose sufficient nerve length to permit a tension-free coaptation. We have recently investigated a definitive end-to-side repair mouse model, in which axons fluoresce and can be accurately traced to the motor neuron pool [12]. We have shown that collateral motor sprouting will not occur without injury, while collateral sensory sprouting will occur without injury. A crush injury will produce some motor regeneration, but a neurectomy is required for robust motor regeneration. We report a modified case of an end-to-side motor reinnervation of the suprascapular nerve using the spinal accessory nerve following a C5 to C6 avulsion injury. In this case, a partial neurectomy was made in the spinal accessory nerve at the location of the end-to-side repair prior to an induced crush injury proximal to the repair site.
Case Report
Preoperative Course
A 29-year-old right-hand dominant man was involved in a motorcycle accident in August 2003. The patient sustained a C5 to C6 nerve root avulsion leaving him with 0/5 shoulder and elbow motor strength and diminished sensation in the right thumb, index finger, and lateral humeral region. Notably, the patient had good trapezius motor function. The patient was referred to our institution for surgical evaluation approximately 12 weeks following his injury and on exam demonstrated no clinical or electrodiagnostic improvement in symptoms.
Operative Procedure
Reconstruction of the axillary and suprascapular nerves was performed, as is frequently done since these nerves are both compromised in upper trunk injuries. In addition, a double fascicular nerve transfer to restore elbow flexion was performed. A triceps to axillary nerve transfer was used for axillary reconstruction, employing the triceps branch (to medial head) of the radial nerve as the donor. The branch to the medial head is the longest triceps branch, allowing for a tension-free transfer while minimizing the need for intramuscular dissection to free the donor.
Given that the brachialis is the most powerful flexor of the arm, a double fascicular transfer procedure was performed using redundant fascicles from both the ulnar and median nerves to reinnervate both the biceps and the brachialis branches of the musculocutaneous nerve.
Both the triceps to axillary and double fascicular transfers have been well described previously, as illustrated in the thorough reviews by Mackinnon et al. and others [7,14,16,17].
To first describe the end-to-side spinal accessory to suprascapular nerve transfer procedure, a supraclavicular incision in the neck was utilized while the patient was in the supine position. The distal accessory nerve was identified along the free border of the trapezius muscle. The plexus was followed distally to the suprascapular nerve. A second incision was made in the medial arm and dissection proceeded down through the soft tissue to identify the median, ulnar, musculocutaneous, and lateral antebrachial cutaneous (LABC) nerves. A 3-cm portion of the LABC was harvested for grafting and sutured end-to-end to the distal stump of the identified suprascapular nerve and end-to-side to the accessory nerve. A partial neurectomy over approximately half of the accessory nerve was performed (Fig. 1). After securing the graft in place, a 30-s crush injury with jewelers forceps was applied to the accessory nerve proximal to the end-to-side anastomosis.
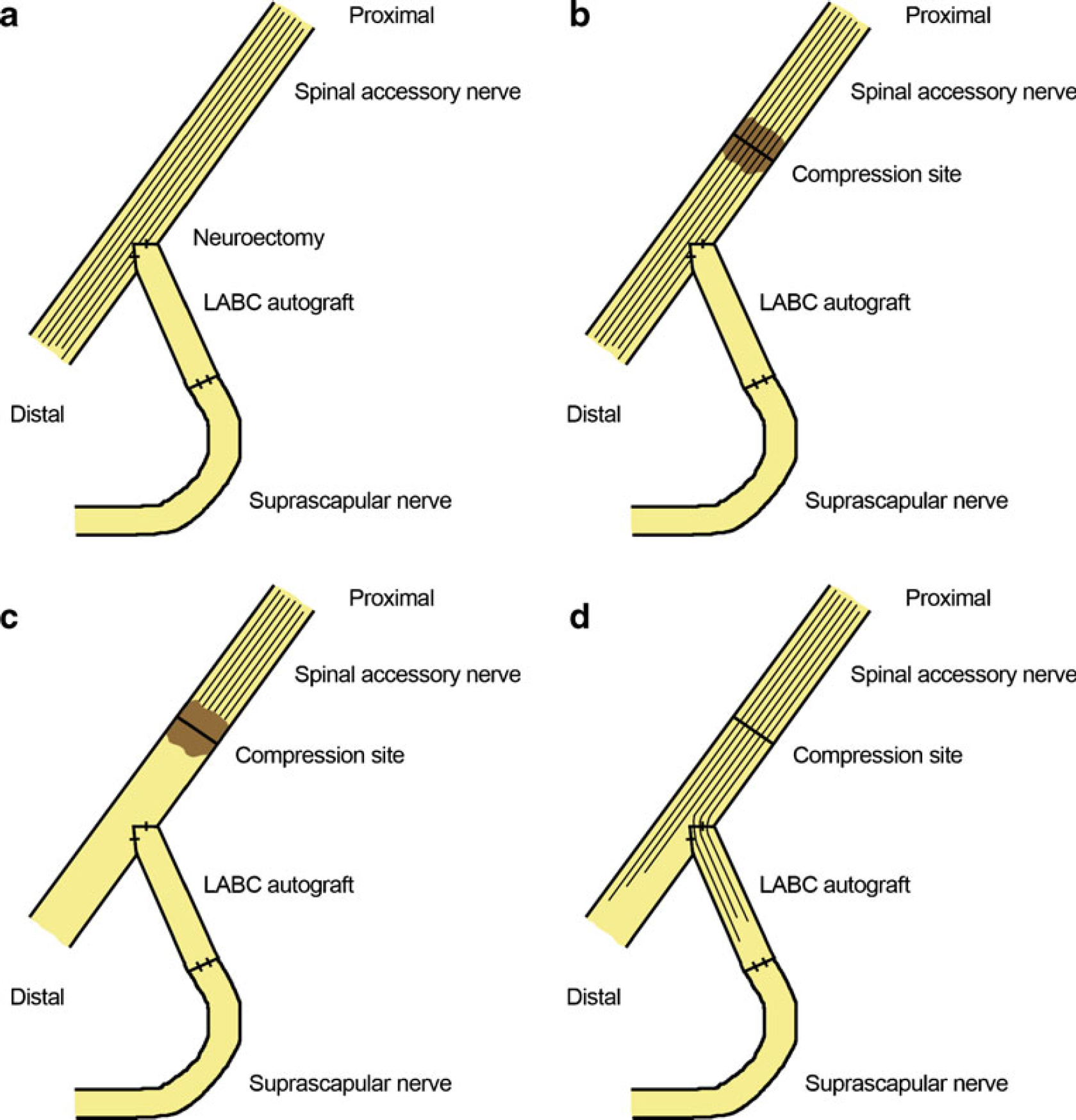
Reinnervation mechanism of an end-to-side neurotization of the suprascapular nerve to the spinal accessory nerve to restore supra/infraspinatus function and preserve trapezius function.
Postoperative Course
Postoperatively, the patient participated in active physical therapy and motor re-education. He was seen back in the immediate postoperative period at 3, 9, 16 months, and 5.5 years. At 16 months, the patient had regained full strength in both elbow flexion and shoulder abduction with some atrophy of the deltoid. At 5.5 years, the patient demonstrated the same full strength in both elbow flexion (Fig. 2; Video
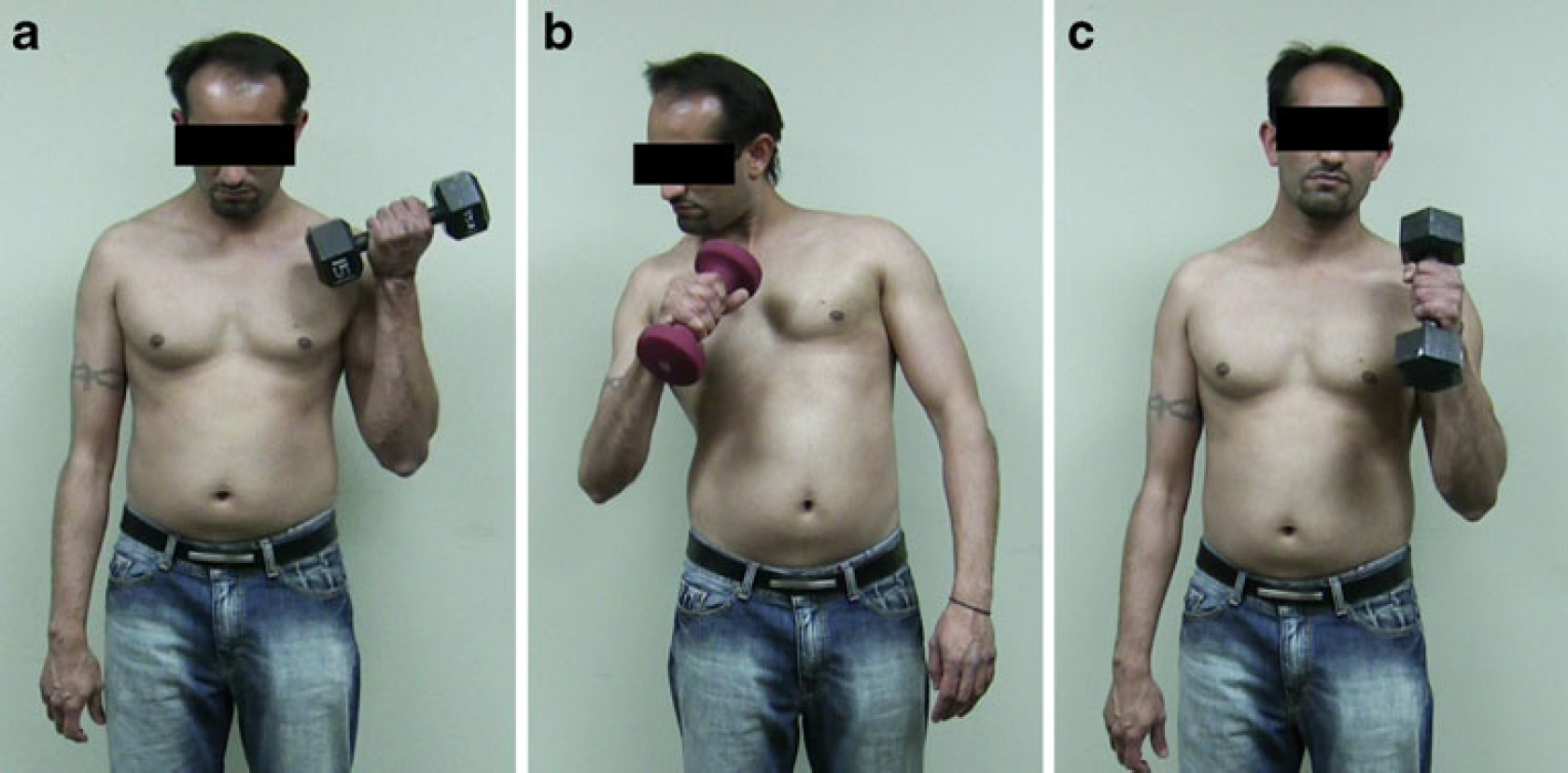
Restoration of elbow flexion 5.5 years following end-to-end neurotization of the ulnar nerve (flexor carpi ulnaris fascicle) to the brachialis nerve and median nerve (flexor carpi radialis fascicle) to the biceps branch of the musculocutaneous nerve.
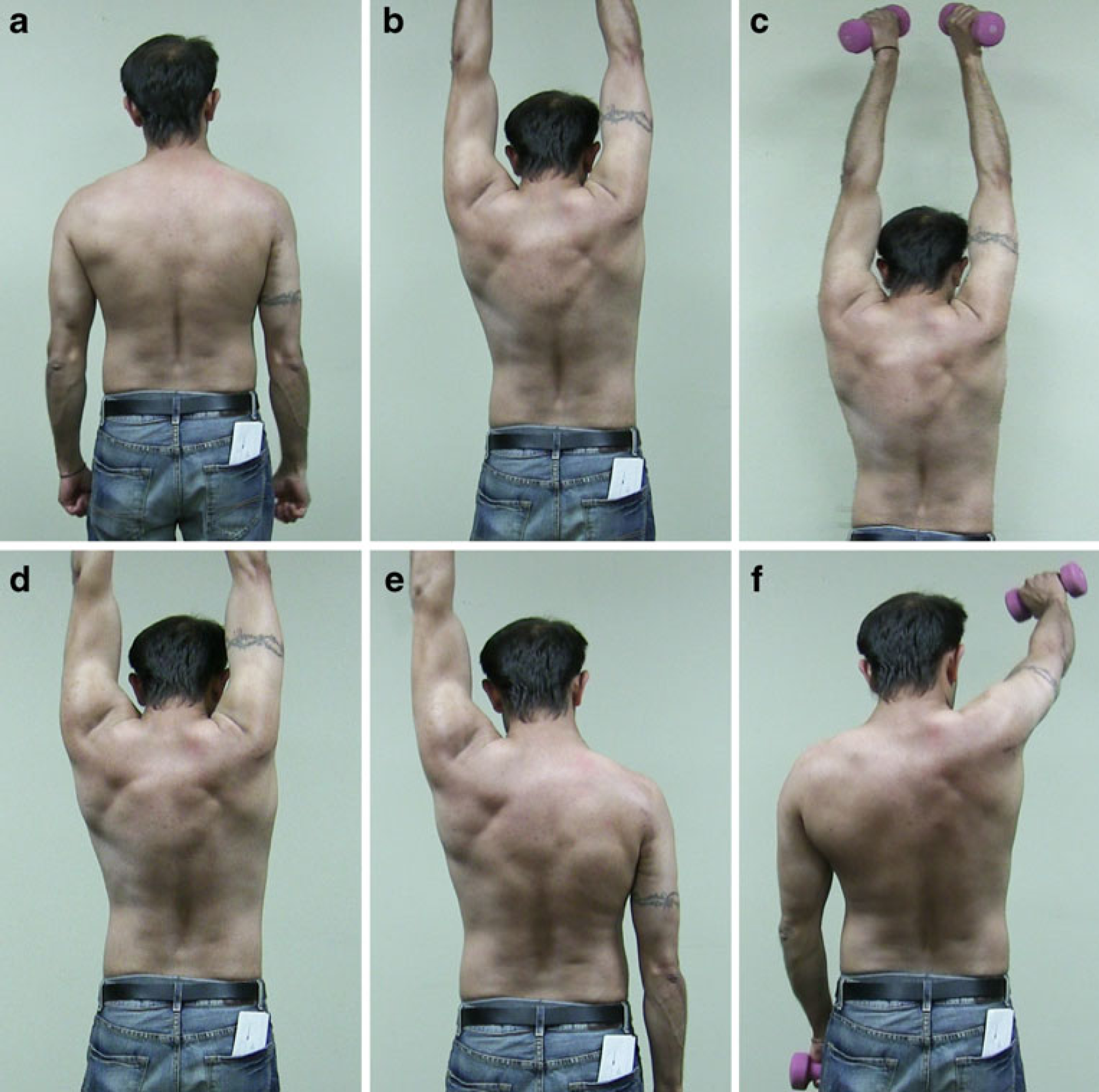
Five years and 6 months following an end-to-side neurotization of the suprascapular nerve to the spinal accessory nerve and end-to-end neurotization of the triceps branch to the axillary nerve on the right side.
Discussion
The precise mechanism of axonal regeneration following end-to-side neurrorhaphy remains controversial with both experimental and clinical studies reporting mixed results [4,6,8,11,12,19,20,23–25,33–37]. Several authors have concluded that axonal damage to the donor nerve is required to induce motor collateral sprouting but may not be required to induce sensory sprouting in end-to-side neurorrhaphy [1,12,28,29]. In a recent review by Dvali et al., the authors concluded that the degree of motor axonal sprouting following end-to-side repairs depends upon the degree of axonal damage, while sensory sprouting was less dependent on the presence of injury [8]. After reviewing both the basic science and clinical literature, they concluded that end-to-side repair without deliberate nerve injury should be limited to repair of noncritical sensory deficits. In a similar review by Rovak et al., the authors also concluded that collateral sprouting depended not only upon axonal damage but also was highly dependent on the extent of injury, with more collateral sprouting associated with increased damage [26]. While several authors have reported excellent functional results with facial nerve reinnervation using an end-to-side repair using the hypoglossal nerve as a donor [2,3,9,27,31,32], the most definitive experimental study on end-to-side repair was recently reported by Hayashi et al. using Thy1-GFP mice that express green fluorescent protein in their motor axons [12]. This study utilized the femoral nerve as a donor and a transected sciatic nerve as the recipient. A nerve graft taken from the median nerve was sutured end-to-side into the femoral nerve and into the distal stump of the sciatic nerve. Both atraumatic model and epineurotomy group were used, with and without a proximal compression injury to the donor (femoral) nerve. Confocal imaging, histomorphometry, and retrograde labeling demonstrated the most rapid and robust regeneration in the epineurotomy group that had also received a proximal compression injury.
Our report corroborates the laboratory findings of Hayashi et al. by illustrating several important technical points regarding end-to-side repairs. As described in the operative procedure, it is critical to introduce a neurectomy into the donor nerve, creating a small degree of axonal disruption while removing basal laminar layers (Fig. 1a). After securing either the recipient stump or in this case an intervening autograft, an axonotmetic crush injury was induced proximal to the end-to-side repair site on the donor nerve (Fig. 1b). Wallerian degeneration proceeds distal to the axonotmetic injury (Fig. 1c). Following recovery from axonotmetic injury, axonal regeneration proceeds down both the native donor nerve and into the recipient pathway through the end-to-side repair (Fig. 3d). While neurectomy alone has been shown to cause some injury to the donor nerve, an additional crush would result in a greater net degree of injury, which animal studies have shown to result in greater motor recovery (as described above). Therefore, in our patient, the crush injury and the neurectomy to the donor nerve both likely play an important role in enhancing regeneration.
The results from this end-to-side suprascapular nerve to axillary nerve were outstanding, especially in the fact that we did not downgrade trapezius muscle function evident with proper scapular stabilization (Video
Although the precise mechanisms underlying end-to-side regeneration remain unresolved, this case provides a clinical example in which end-to-side repair was used with a good clinical outcome. As discussed above, this case utilized both an axonotmetic injury and direct neurectomy to the donor nerve, both of which are likely critical to allow adequate motor nerve regeneration for an end-to-side nerve transfer.