
Abstract
Cutaneous fungal infections are a rare but significant complication associated with immunocompromised states. Lesions allowed to progress to disseminated fungemia are associated with a near 80% mortality rate. Treatment guidelines aimed at local control are vague, centering on wide local excision with systemic antifungal medications. We present the case of a 3-year-old female who, while receiving induction chemotherapy, developed a progressive Aspergillus flavus infection. Involvement included the distal palm and common and proper neurovascular bundles to two fingers. Initial treatments with serial debridement and topical Dakin's solution were unsuccessful in eliminating this fungal infection. A novel treatment using topical voriconazole mixed with Aquaphor® (Beiersdorf AG; Hamburg, Germany) was compounded in the hospital pharmacy to maintain a moist wound healing environment followed by the use of the Vacuum Assisted Closure (VAC®, Kinetic Concepts, San Antonio, TX). Significant improvement was noted within 4 days with this new dressing regimen. Topical voriconazole therapy followed by VAC allowed progressive healing and eventual closure with a split thickness skin graft. The wound was then durably closed, allowing critical chemotherapy to resume. No evidence of systemic fungemia developed, and her clinical recovery preceded laboratory evidence of immune system recovery. Fungal skin infections can be a threat to both life and limb in immunocompromised patients. The armamentarium available to combat this rare but difficult problem is imperfect. In certain infections not responsive to other therapies, the therapeutic regimen described herein should be considered if wide local excision carries significant functional morbidity.
Introduction
Childhood cancers are treated more effectively now than ever before. With more advanced and aggressive treatments have come significant comorbidities. In the case of chemotherapy for hematopoietic malignancy, pancytopenia and temporary devastation of the immune system put the host at risk for otherwise uncommon sequelae. As immune surveillance and cell-mediated immunity decrease, the body becomes ever more susceptible to skin and soft tissue infections. Small breakdowns in the defense mechanisms of the skin can turn otherwise trivial microbe exposures into life-threatening illness.
Elevated risk is especially important in the case of fungal soft tissue infection. Treatment efforts for this difficult problem must prevent systemic spread as the evolution of disseminated Aspergillosis is associated with mortality rates as high as 80% [2–4,8]. Wide local excision of all involved soft tissue has been discussed as the preferred surgical intervention. Such drastic measures in the hand, however, would result in a lifetime of disability and disfigurement.
We present the case of a 3-year-old female child who developed a locally aggressive and resistant Aspergillus flavus infection at the distal palm. Multiple and progressive debridements were able to control the disease only when coupled with a combination of intravenous and compounded topical voriconazole cream. Subsequent use of a Vacuum Assisted Closure (VAC) device and a split thickness skin graft provided rapid and stable closure to allow the continuation of chemotherapy.
Case Report
K.T. was initially evaluated following 3 months of vague lower extremity myalgias and an episode of syncope. She was found to have precursor B cell acute lymphoblastic leukemia with severe anemia, neutropenia, and thrombocytopenia. An aggressive regimen of induction chemotherapy including doxorubicin and vincristine was begun. As is common with small children, the hand with her intravenous line was placed in an arm board to limit trauma and to secure vascular access. When this board was removed several days later, a small black spot was noticed at the distal palm, just proximal to the third web space on her left hand. The clinical hallmark of Aspergillus skin infection is a black discoloration. A 4-mm punch biopsy removed the entire area of concern. Pathologic evaluation of the specimen was significant for nearly complete dermal and subdermal invasion of a fungus identified as A. flavus. The patient was taken urgently to the operating room where the wound was debrided of all necrotic-appearing tissue to a healthy margin of approximately 5 mm in all directions except the base of the wound. This base consisted of the common and proper neurovascular bundles to the ulnar aspect of her long finger and the radial aspect of her ring finger (Fig. 1). These vessels appeared disease-free and were patent with excellent Doppler signals. A second debridement was scheduled for 3 days later; only a small amount of black tissue was identified and removed during that procedure. Wound care was performed with twice daily application of 0.025% Dakin's solution. Soaks in warm soapy water facilitated dressing changes. Dakin's solution and gauze dressings are bactericidal and fungicidal and may help to debride small remaining foci of necrotic tissue while providing minimal and acceptable harm to native tissue [11]. Twice daily dressing changes and wetting of the gauze every 4 h was only moderately effective at maintaining a moist environment. The gauze inevitably became stuck to the wound, and removal during dressing changes caused the patient great pain and distress.

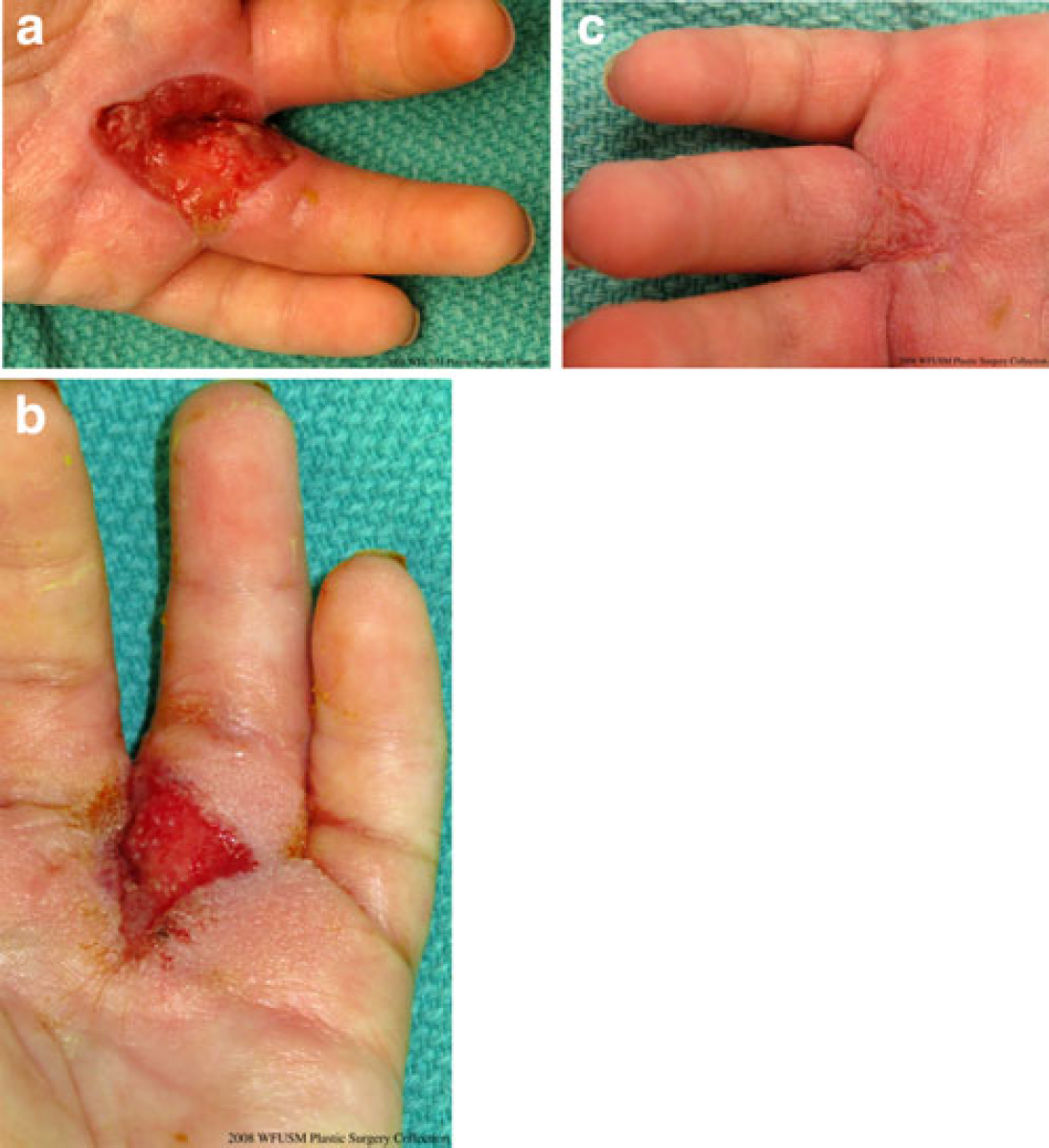
Progression of wound in spite of multiple debridements, topical 0.025% Dakin's solution and intravenous voriconazole. Wound began as a 3-mm eschar. Taken with permission from “A Collection of Images and Illustrations,” published by the Wake Forest University School of Medicine, Department of Plastic and Reconstructive Surgery.
Third and fourth debridements were unsuccessful in eradicating the fungal invasion of tissue. The wound displayed recurring, persistent black discoloration in the periphery and base. During the fourth debridement, neurovascular bundles were removed along with 5 mm circumferential margins of palmar skin. The base of the wound was debrided to clean, healthy appearing tissue which required removal of the necrotic-appearing flexor tendon sheath to the ring finger. A fifth debridement 2 days later was required to remove clearly dead tissue with fungal elements found on microscopy.
Multiple surgical attempts failed to rid her wound of fungus. The wound consistently had a light gray/black appearance within one dressing change of a debridement. Dakin's solution dressings and intravenous voriconazole were inadequate. Progressive fevers and cultures from the wound consistently were positive for Aspergillus. Chemotherapy for this child could not be continued with ongoing cutaneous fungal infection. Radical amputation of subtotal or total hand was contemplated.
At this point a new treatment approach was tried as a last effort to save this child's hand. Based on guidelines published in a previous article [7], a topical solution of voriconazole was developed and compounded in our pharmacy. Two hundred milligrams of the intravenous formulation of voriconazole was mixed in 4 ml of sterile normal saline to create a 5% solution. This was then mixed with 15 g of Aquaphor. The aqueous voriconazole was mixed with the Aquaphor each morning, and a 24-h expiration date was assigned to the preparation. Dressings were changed twice daily; the wound was cleansed with a soapy warm water soak with each dressing change. Systemic antifungal voriconazole treatment was continued in addition to the topical voriconazole dressings. Because a bone marrow biopsy showed the cancer was in remission, chemotherapy was able to be temporarily held to improve wound healing. Of note, the application of the topical antifungal and resultant healing preceded recovery of this patient's immune response as her white cell count remained low at 0–1,600 lymphocytes along with an absolute neutrophil count between 100 and 600.
The patient was taken to the operating room for evaluation and cultures 7 days after the institution of this new treatment plan. All areas appeared clean and healthy, and no distinct evidence of fungal disease was found. A clean wound was confirmed with multiple samples sent for culture and to pathology for evaluation of fungal invasion. Significant granulation tissue had now begun within days of initiating topical voriconazole. A Vacuum Assisted Closure device was placed 2 days after cultures were negative and changed every third day for a total of 12 days. Cultures and pathologic slides sent at each VAC change were negative. In addition to promoting granulation, VAC application allowed progressive healing and contraction of the size of the wound (Fig. 2). A split thickness skin graft of 0.0010-in. thickness of glabrous skin from the sole of the left foot was placed on the hand, and a VAC was applied over the graft. Removal of the VAC after 4 days showed 100% skin graft take.
Discussion
There is a paucity of information in the literature to guide treatment of complex fungal wounds, especially in the hand. A small number of reported series suggests that the highest survival is likely only with rapid and wide surgical excision and intraoperative microscopic control [5,6]. Though wide local excision theoretically presents the highest likelihood of cure, such drastic measures in the hand may result in considerable life-long disability. As a result, margins may continue to be positive. Nonetheless, most sources reviewed agree that both fungal cultures on soft tissue specimens and microscopic exam by pathologists are necessary to determine residual fungal invasion and to support complete eradication of disease.
It is likely that both aggressively timed surgical excision and close monitoring via pathology and cultures as well as advancements in wound care contributed to the successful eradication of disease in this child. The continued presence of fungus after progressively more dramatic debridements, coupled with this patient's poor tolerance of very painful wet to dry gauze dressing changes, prompted the creation of a newly compounded form of voriconazole that allowed the wound to stay moist, painless, and in constant contact with the antifungal agent, thereby preventing further desiccation.
Various authors have described innovative approaches to cutaneous Aspergillus infections. Several have described topical application of antifungal agents, and a favorable outcome has been reported in one patient with cutaneous A. flavus using wet to dry 1% voriconazole dressings in combination with debridement and intravenous amphotericin B and caspofungin [7]. Other reports have described favorable outcomes using Mohs excision and systemic amphotericin B or continuous topical infusion of amphotericin B alone [1,10]. Our regimen was built from these ideas but with the added knowledge that a moist wound heals more effectively than a desiccated wound [9].
This patient's recovery was likely multifactorial, and it is impossible to suggest that this wound care regimen saved either her hand or her life. The degree to which this 3-year old will regain sensation in the affected fingers remains to be seen, though she began using both hands equally and readily 4 weeks after stable coverage was obtained. This result does suggest, however, that when faced with a progressive fungal infection in an immunocompromised patient, one might consider the implementation of this topical medication regimen. Further basic science studies are required to know the eventual role that this therapy should play in the treatment of cutaneous Aspergillus infections.