
Abstract
Zone III flexor tendon injuries are relatively rare in comparison to other flexor tendon injuries in zones I, II, IV, and V. Often, these are open injuries resulting from an electrical device like a saw; however, closed injures are even rarer, and those mid-substance ruptures resulting from bowling with no evidence of underlying tendinopathy from diseases like gout are highly unusual. The principles underlying tendon repair remain the same regardless of the etiology. In this case, we delineate some of the options and stress the guiding principles of the various methods available in this interesting and unusual case.
Introduction
Laceration of one or more flexor tendons is one of the most common traumatic injuries encountered by hand surgeons [6]. By contrast, closed rupture of a flexor tendon is less common, with the injury occurring most frequently by avulsion of the profundus tendon from its insertion on the distal phalanx. Rupture is rare at the musculotendinous junction and is often associated with a forearm crush injury. Mid-substance ruptures are typically attributable to underlying pathology such as a fracture, rheumatoid arthritis, or gout [5]. Traumatic mid-substance flexor tendon rupture without underlying pathology is very rare. The most common mechanism of injury for a spontaneous flexor tendon rupture occurs when the actively flexed distal interphalangeal joint is forced into extension.
This case report describes a patient who experienced closed simultaneous mid-substance rupture of the flexor digitorum profundus (FDP) tendons of the right index, long, and ring fingers of the point of lumbrical origin in the palm while bowling. There was no evidence of underlying tendon pathology.
Case Presentation
A 49-year-old man presented to a hand clinic with an inability to completely flex the index, long, and ring fingers on his right dominant hand. His problem began 3 days earlier when he felt what he described as a painful “pop” in his forearm while bowling. After the “pop,” he was immediately unable to completely flex the index, long, and ring fingers. He had no significant medical history, and the resting attitude of his fingers, on physical examination, was suggestive of FDP tendon injury. It was noted that he was unable to actively flex his right index, long, and ring fingers at the distal interphalangeal (DIP) joint. He also had a mass on his volar forearm measuring approximately 5× 5 cm that was tender to palpation. He was not tender to palpation anywhere along the flexor tendon sheath in the hand. Neurovascular examination was normal, and the sublimis tendons appeared intact with independent flexion of the proximal interphalangeal joints. Preoperative assessment included an evaluation for gout, and this was negative. He reported no clinical symptoms suggestive of a history of collagen vascular disease. He had never taken oral steroids nor had he received a steroid injection. He only occasionally took NSAIDs. Radiographic examination showed no evidence of fracture, bone fragments, and intercarpal arthritis within or adjacent to the flexor tendon sheath. The initial diagnosis was rupture of the flexor digitorum profundus tendons to the index long and ring fingers in the forearm. Operative exploration was planned to repair this injury.
Operative Procedure
The patient was taken to surgery 9 days following the injury. A volar curvilinear incision was made beginning at the wrist and carried proximally up the forearm to facilitate exposure. Care was taken not to injure the cutaneous nerves of the forearm, including the palmar cutaneous nerve. A mass of synovium, which had retracted out of the palm and wrist, was noted when the forearm fascia was opened. The ulnar neurovascular bundle was identified and retracted ulnarly to protect it during excision of the synovium. It was clear that the distal ends of the tendons were in the palm. The incision was than extended distally into the carpel tunnel to expose the distal ends of the right index, long, and ring fingers FDP tendons. The superficial palmar arch was identified and carefully retracted distally. The tendon rupture appeared to have occurred just proximal to the origin of the lumbrical muscles. The tendon ends could not be approximated and acute tendon grafting was necessary to restore the integrity of the flexor tendons. The palmaris longus and a half strip of the flexor carpi ulnaris tendons were used as tendon grafts. The palmaris longus was fashioned into a U-shaped graft to motor the long and ring fingers, while the strip of flexor carpi ulnaris was used to graft the tendon defect in the FDP of the index finger. A pulvertaft weave tenorrhaphy was performed, and the resting tension of the tendon grafts was set by flexing and extending the wrist. The incisions were closed and the hand was placed in a dorsal blocking splint. The patient did well following surgery and 3 months of hand therapy. He regained near-normal finger flexor but lacked full DIP joint flexion in a closed fist (Fig. 1). His grip strength 18 months following surgery was 50% of the opposite hand. He had returned to work as a stock room clerk but had not returned to bowling (Fig. 2).
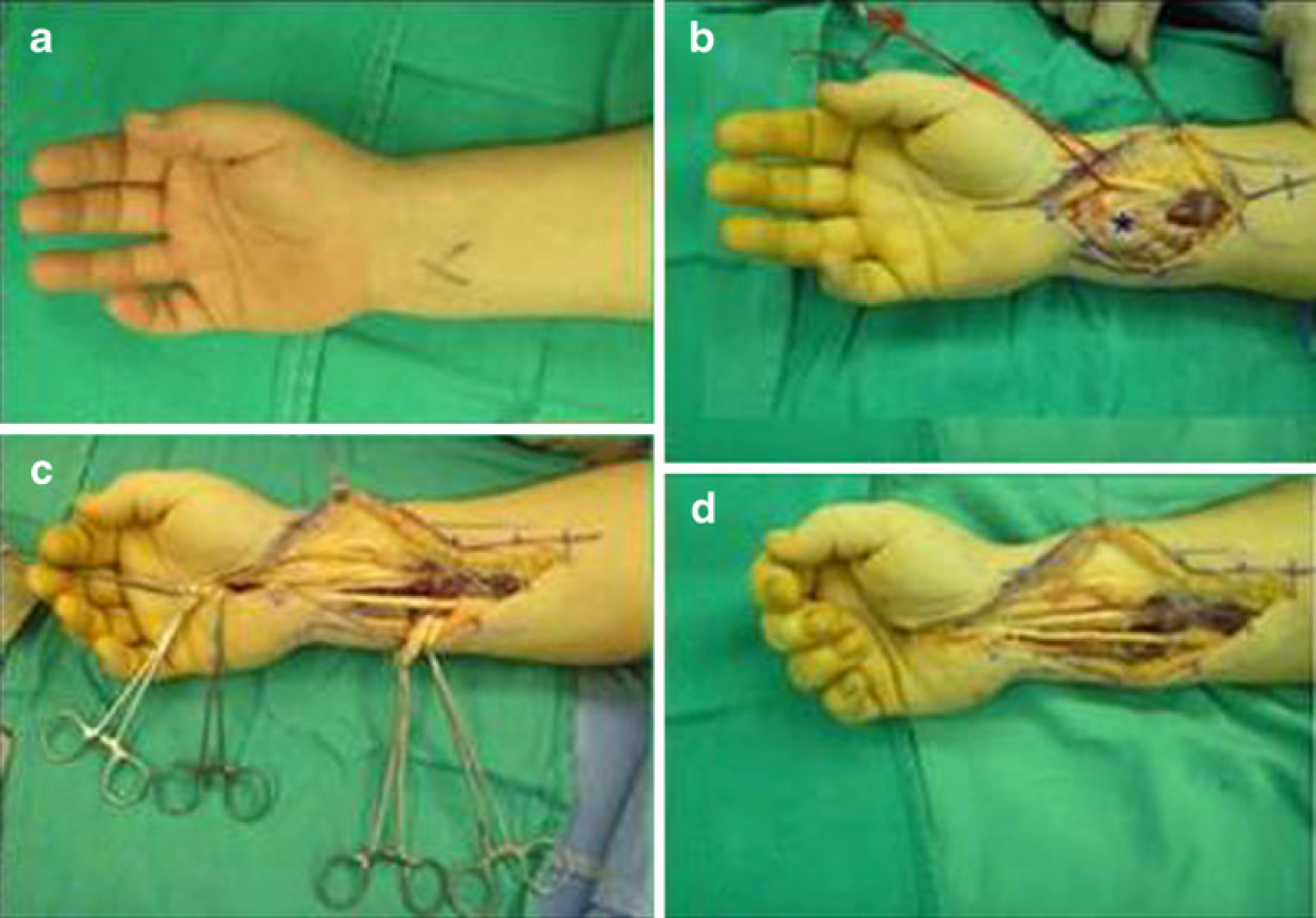
Operative procedure.

Near-normal finger flexor but lacked full DIP joint flexion in a closed fist.
Discussion
Flexor tendon rupture is most commonly described in the long and ring fingers in zone I when the FDP attachment to the distal phalanx is avulsed. This so-called Jersey finger is caused by forced extension of an actively flexed distal interphalangeal joint [8]. This is a common injury that is treated with advancement of the avulsed tendon back into its insertion at the base of the distal phalanx and reattachment with a bone anchor, pull out suture, or a similar technique. Reinsertion of the profundus tendon is best performed within 2 weeks of injury. The patient's history was compatible with this type of injury, but physical examination and X-rays failed to confirm distal avulsion, suggesting a more proximal disruption.
Flexor tendon ruptures due to bowling are exceedingly rare. They have been described in the flexor pollicis longus tendon but never in multiple FDP tendons, which makes this case so unique. We initially considered underlying causes that would result in attrition such as intercarpal arthritis, similar to a Mannerfeldt or a Vaughn–Jackson type of lesion, or gout, but we could not elicit that history. Furthermore, previous use of steroids and other medications such as NSAIDS and levaquin were considered. But as noted, use of NSAIDS was infrequent in this patient, and he has no recollection of any recent use of other medications, prescription, OTC, and herbal medication. We do believe, though, that although the cause is not clear, there is most likely an underlying cause, perhaps a medicine, that along with frequent bowling acted synergistically to cause tendon rupture. The patient did report taking NSAIDS occasionally after bowling, for instance. But this is still a highly speculative assumption.
Factors that influence the treatment and outcome of this injury include the length of time between injury and treatment, the extent of tendon retraction, the condition and blood supply to the avulsed tendons, the method of repair, and the type of duration of hand therapy [1]. When we confirmed that three FDP tendons had ruptured secondary to bowling, a search was initiated for systemic conditions that could have caused attrition of the tendons and/or a predisposition for spontaneous rupture, but none were found. The tendons did not appear diseased at surgery but could not be re-approximated primarily, necessitating the tendon grafts.
Rheumatoid arthritis is a disease with a recognized predisposition for tendon rupture. Tendon integrity is weakened by direct invasion of the tendons and interference with normal tendon blood supply from rheumatoid tenosynovitis. Attrition rupture may occur after tendons subluxate or dislocate due to loss of normal supporting structures by repeatedly passing over osteophytic surfaces or through erosion from chronic synovitis [2].
Tophaceous gout, a form of chronic gout, can result in nodular masses and depositions of uric acid crystals (tophi) in various soft tissues of the body, including tendons, predisposing them to rupture. Surgical pathology will demonstrate uric acid crystals within the excised tendon. Medical therapy to prevent further acute attacks of gout and reduce tophaceous gout infiltration is highly recommended [3]. Pseudogout may also lead to tophaceous deposition of calcium pyrophosphate dehydrate crystals in tendons, once again predisposing to tendon rupture [4]. In both disease processes, crystal-induced inflammation and chronic attrition have been emphasized in the pathogenesis of tendon rapture. A full medical workup performed to elucidate possible sources of autoimmune disease and systemic metabolic disorders was negative. This suggests that trauma alone during bowling caused rupture of the flexor tendons in this case.
No matter the cause of the injury, the principles of flexor tendon repair must be observed, anatomy must be understood, and proper technique must be employed. In this case, local tendon grafts were utilized to bridge the defects in zone III. Tension was set using the pulvertaft technique, which, in addition to strength, affords the surgeon more precision in restoring the normal resting cascade of the fingers. Because of the common origin of the FDP, a U-shaped graft was used for the long and ring fingers to minimize the possibility of quadriga. However, the index finger was grafted separately in an attempt to restore and maintain the relative independence it has in relation to other fingers in the hand.
Free tendon grafting should be considered only under a strict set of guidelines. If there is a wound, it must have healed enough to return suppleness to the soft tissues of the hand, permitting full passive flexion and extension of the involved digit(s). If there is an injury to both digital nerves, repair and regeneration should precede tendon grafting. At least one digital nerve should be functioning. The most important factor affecting the prognosis of flexor tendon grafting is the patient's age, with the best results seen in patients between 10 and 30 years old [7]. This patient could fully flex the DIP joints with the MP joints extended, but could not fully flex them in a closed fist position. This suggests that the grafts were slightly too long and should have been repaired under more tension.
Contraindications to flexor tendon grafting include inadequate soft tissue, an insensate digit, poor vascular supply, and the need for a pulley reconstruction. In addition, the mechanism of injury affects outcome, with flexor grafting not advised after extensive soft tissue loss, severe phalangeal fractures, and crush injuries [7].
The complications of flexor tendon injury and repair include the quadrigia effect, adhesions, flexion contractures, graft rupture, swan neck deformity, bowstringing, and a lumbrical plus deformity which occurs when a profundus tendon is cut distal to the origin of the lumbrical muscle in zones one or two. The FDP tendon retracts proximally and is then attached to the finger only through the lumbrical muscle. This increases tension on the lumbrical muscle and causes an extrinsic/intrinsic imbalance, manifested when the patient initiates flexion, which then paradoxically extends the interphalangeal joint through the pull of the proximal FDP muscle on the lumbrical tendon [7]. The FDP tendons in this case ruptured proximal to the origin of the lubrical muscles, decreasing the resting tension on the lumbricals.
Bowstringing occurs in severe zone II injuries with disruption of one or more pulleys of the fibrosseus canal. Pulley reconstruction is often done primarily over a Hunter Rod with tendon reconstruction performed as a secondary procedure. Tendon adhesions are most problematic in zone II injuries but can occur to grafted musculotendinous units in the hand and forearm. Early hard therapy to initiate passive tendon gliding is important to regain full motion. This patient began passive motion exercises 5 days following surgery. The most critical problem in grafting FDP tendons is adjusting the muscle tension to avoid the quadrigia effect, which was a problem in this case. The excursion of the uninjured small finger FDP tendon after surgery allows full flexion of the DIP joint, while the added length of the grafted profundus tendons to the ring and long fingers prevents full composite flexion into a fist. The index finger DIP flexor lag is less severe. Slightly more graft tension would have produced better function, but the patient is happy with the results.