
Abstract
Background
Arthrodesis of the distal interphalangeal (DIP) joint is indicated for the treatment of arthritis. While several techniques have been recommended, the use of headless compression screws has grown in popularity. Rates of union reported vary widely, ranging from 80% to 100%, with most studies based on small series. The purpose of this study was to review the outcomes and complications associated with DIP joint arthrodesis using the Herbert headless compression screw in a large case series.
Methods
The medical charts, surgical reports, and X-rays for patients undergoing DIP joint arthrodesis with a Herbert screw between January 1996 and May 2006 were retrospectively reviewed to determine the frequency and types of complications. All operations were performed by the senior author at a single institution.
Results
Of 64 joints in 51 patients that were treated with the Herbert screw, a total of 95% (n=61) went on to union. Union within 3 months occurred in 89% (n=57) while delayed union (between 3 and 6 months) occurred in 6% (n=4). Nonunion requiring subsequent revision arthrodesis occurred in 5% (n=3). Screw removal for symptomatic hardware was required in 8% (n=5).
Conclusions
Fusion of the DIP joint with the Herbert screw can be achieved at rates that are comparable to other techniques and other headless compressive screws. However, while complications do occur, the Herbert screw provides an acceptable rate of union and ease of operative technique, making it a suitable procedure for DIP joint arthrodesis.
Keywords
Introduction
Arthrodesis of the distal interphalangeal (DIP) joint is widely acknowledged as the indicated treatment for several forms of arthritis, including primary osteoarthritis, inflammatory arthritis, and traumatic arthritis [8]. While methods of fixation vary among surgeons, the most common techniques employ the use of either Kirshner wires (K-wires) with interosseous wiring, or headless compression screws, either cannulated or uncannulated [8]. Previous studies of the Herbert compression screw have suggested that compression screw fixation is a reliable option for small joint arthrodesis [1–3,5,6].
For DIP arthrodesis using a headless compression screw, there is a wide range of union rates reported in the literature, ranging from 80% to 100% [1–3,5,6]. The purpose of this study was to determine the rate of union and review the complications associated with distal interphalangeal joint arthrodesis using the Herbert headless compression screw in a large, consecutively treated case series.
Materials and Methods
This study was based on a retrospective analysis of 51 consecutive patients, resulting in 64 distal interphalangeal joint fixations using Herbert screws performed by the senior author (R.J.K.) at a single institution from January 1996 to May 2006. The surgical technique was relatively unvaried between patients and began by exposing the DIP joint through a curvilinear incision over the dorsal aspect of the finger with division of the extensor mechanism. A cup-and-cone arthrodesis was accomplished using a rongeur, and a 0.035-in. K-wire, used as a pilot guide, was drilled proximal to distal through the distal phalanx. After fluoroscopic confirmation of the K-wire's position, it was removed and used to select a Herbert screw of the corresponding length (Fig. 1a). Next, the handheld Herbert screw drill was used to create pilot holes in the distal phalanx and the distal aspect of the middle phalanx. The Herbert screw was used to stabilize and compress the DIP joint in full extension or the thumb IP joint at 10° of flexion (Fig. 1b). Fluoroscopic confirmation of the alignment of the joint and position of the screw were obtained. The wound was closed with a 4-0 nylon suture, and a sterile dressing was placed in conjunction with a plaster splint. Splints were removed on postoperative day 1 or 2.
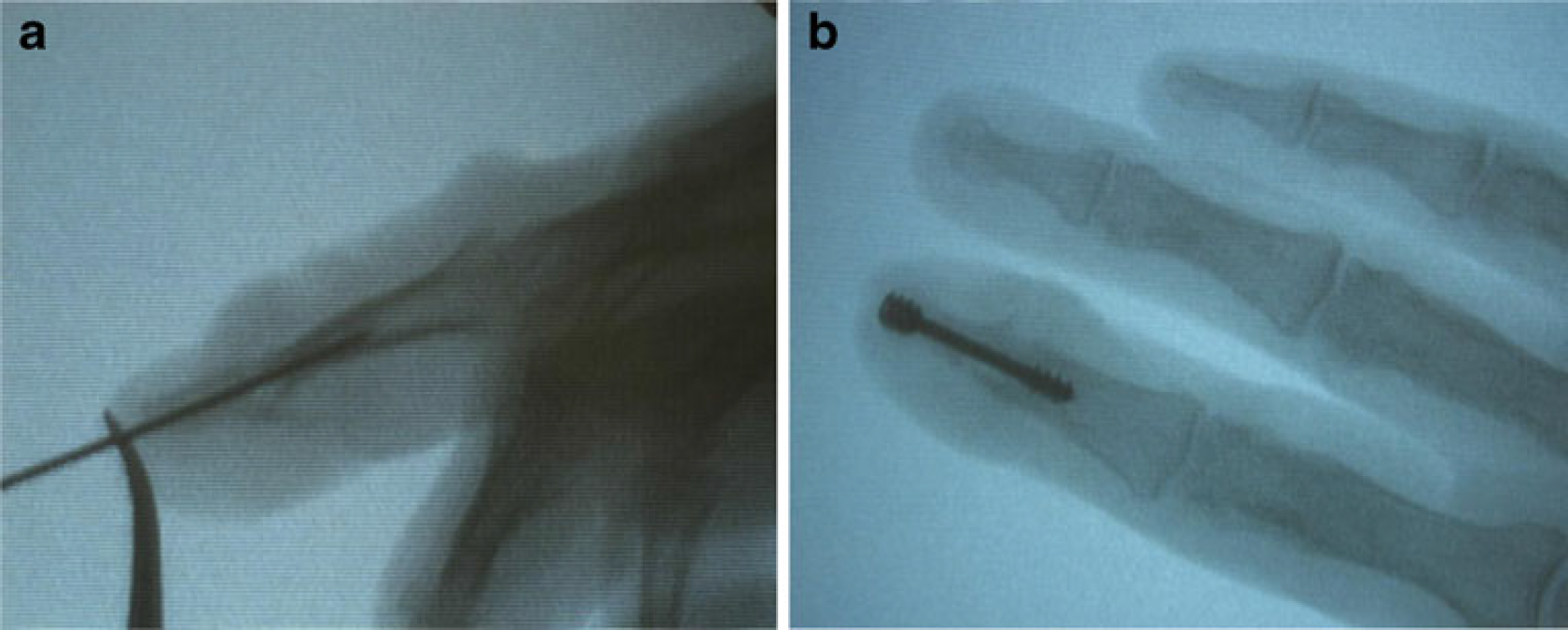
Intraoperative fluoroscopic images.
The medical charts, surgical reports, and X-rays were reviewed to determine the frequency and types of complications as well as the post-operative time required to achieve union. Bony unions were verified both radiographically, by trabeculae crossing the arthrodesis site, and clinically, by evidence of a painless, stable joint on stress (Fig. 2). All joints were categorized into three types of union. The first category was union within 3 months, the second was a delayed union (3 to 6 months), and the final was a nonunion (greater than 6 months and requiring further revisional surgery to obtain union).

Post-operative X-ray demonstrating union with trabeculae crossing the arthrodesis site
Results
Of the 51 patients that were treated with the Herbert screw, 67% (n=34) were female and 33% (n=17) were male, with a median age of 57 years, ranging from 19 to 89. Of the 64 resulting joints, 46% received the procedure due to post-traumatic arthritis, 44% due to primary arthritis, 5% due to gouty arthritis, and the remaining 5% due to rheumatoid arthritis. Seven of the joints fused were thumb IP joints, and the remaining 57 were DIP joints, with 19 index finger fixations, 23 middle finger fixations, six ring finger fixations, and nine small finger fixations. Average follow-up time was 15.5 months, ranging from 3 months to 8.8 years.
A total of 95% (n=61) ultimately went on to union and the average overall time to union in these cases was 2.8 months, with delayed unions taking up to 5.7 months. Union within 3 months occurred in 89% (n=57) while delayed union occurred in 6% (n=4). Failure to fuse using the Herbert screw occurred in 5% (n=3). In two of these cases, nonunion was corrected by screw removal and revision arthrodesis with interosseous wires and K-wires. In one case, an attempt to correct persistent pseudoarthrosis was made by bone grafting and revision screw fixation. A subsequent infection led to the screw removal a second time, but union and fusion eventually occurred with immobilization.
Screw removal for symptomatic hardware was required in 8% (n=5). Of these patients, the primary reason for symptomatic hardware was screw prominence, with the distal end of the screw incompletely buried in the distal phalanx. In all of these cases, the screw was removed after clinical and radiographic union was confirmed. Symptomatic hardware occurred in two index fingers, two ring fingers, and one small finger.
Discussion
Reported union rates associated with DIP arthrodesis using headless compression screw fixation vary widely in the literature [1–3,5,6]. To our knowledge, our study represents the largest consecutive series of cases and confirms that union rates are consistent with the relatively high percentages that were previously reported.
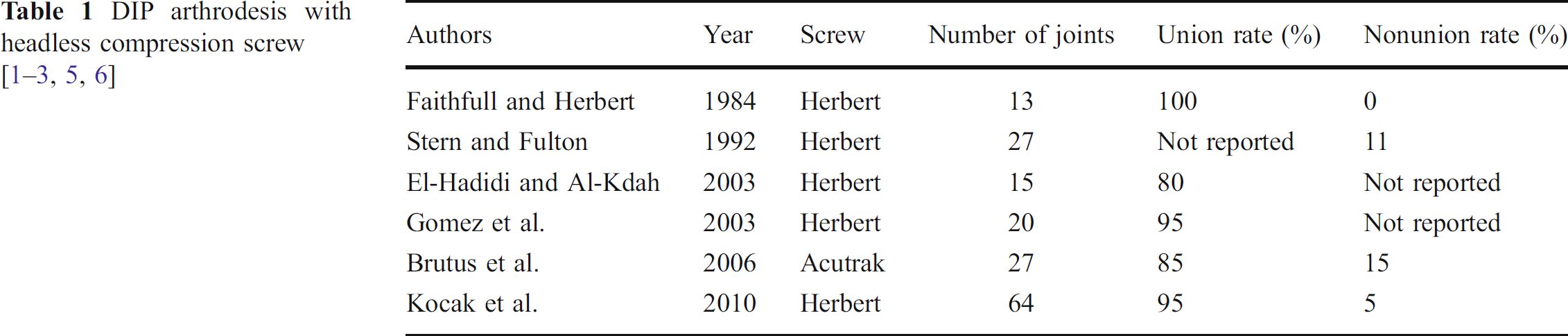
Relatively few studies that describe union rates and types of complications resulting from this type of fixation have been reported (Table 1). Based on our literature search, we were able to identify five previous papers reporting outcomes for DIP or thumb IP joint arthrodesis using headless compression screw fixation [1–3,5,6]. The earliest report by Faithfull and Herbert describes the use of this screw in 11 DIP and two thumb IP joints with 100% success [2]. Unfortunately, time to fusion and follow-up times are not reported. These dramatic results were challenged in a paper from 1992, which reported a nonunion in three out of 27 joints (11%) treated with Herbert screw fixation [6]. In 2003, one study reported union in 12 out of 15 joints (80%) [8], and in another, a series of 16 DIP and four thumb IP joint arthrodesis operations with the Herbert screw, an osseous union was reported in 95% of cases [7]. New literature in 2006 reported using the Acutrak headless compression screw in a series of 27 joints. The authors reported union in 23 (85%) and nonunion in four (15%), giving them the highest nonunion rate reported in the literature [4]. These previous studies demonstrate nonunion rates ranging from 0% to 15%. In all of these studies, the number of thumb IP or DIP joints included ranged from 13 to 27 joints in a given study. The two studies with 27 joints found the highest nonunion rates. In our study, which had the advantage of analyzing the largest series of cases to date, we found a much lower nonunion rate.
In addition to nonunion, previous studies have reported other complications associated with this procedure such as dorsal skin necrosis, parasthesias, cold intolerance, and prominent hardware. The present study corroborates some of these findings, especially as symptomatic hardware was the primary indication for hardware removal. While it would be expected that symptoms related to hardware would be caused by prominence of the screw in specifically smaller digits, this was not entirely the case. While incomplete burying of the screw was the primary reason for symptomatic hardware, the index finger was the most common digit requiring hardware removal. This may be due the role of the index finger in pinching and the resulting pressure exerted over the head of the screw at the distal tip. We postulate that this complication can be avoided by completely burying the trailing end of the screw in the distal phalanx.
Alternate methods of small joint arthrodesis have also been reported, with interosseous wire fixation being the most common [7,9]. The reported union rates for interosseous wire fixation in these studies ranged from 80 to 100%. While these rates are comparable to the ones reported in the present study using Herbert screws, the authors feel that that the technical simplicity and rigid stability of fixation associated with compression screw placement make them the ideal choice in most situations.
Despite the utility of analyzing such a large patient base, the limitations of our study must still be noted. As mentioned above, the variation between what each author considers “union” could cause data to be distorted between studies. We chose to report union status separate from complications. Also, because a single surgeon preformed all the procedures that we analyzed, it brings into question whether our union rates will be reflective of a larger population of surgeons performing the same operation, as there is a technical learning curve that develops as a greater number of procedures are done.
Conclusions
A wide range of union rates following arthrodesis of the DIP or thumb IP joint using a headless compression screw have been reported. The present study, which is based on a large series of patients, supports a high union rate for this procedure. In addition, due to its technical simplicity, limited post-operative immobilization time, and low complication rate, arthrodesis using the headless compression screw presents a favorable method for DIP or thumb IP joint fusion.
Footnotes
The authors declare that they have no conflict of interest.