
Abstract
Background
Traditional management of lateral humeral epicondylitis (“tennis elbow”) relies upon antiinflammatory medication, rehabilitation, steroid injection, counterforce splinting, and, finally, surgery to the common extensor origin. The diversity of surgical approaches for lateral humeral epicondylitis (LHE) suggests perhaps that the ideal technique has not been determined. Denervation of the lateral humeral epicondyle is the concept of interrupting the neural pathway that transmits the pain message. Epicondylectomy may accomplish its relief of LHE by denervating the epicondyle.
Methods
Since it is known that the posterior branch of the posterior cutaneous nerve of the forearm innervates the lateral humeral epicondyle, 30 patients who were treated surgically for refractory LHE were retrospectively evaluated. Group 1 consisted of 17 patients who were treated with epicondylectomy alone, group II consisted of seven patients who were treated with lateral epicondylectomy plus neurectomy, and group III consisted of seven patients treated with lateral denervation alone.
Results
Denervation alone gave statistically significantly greater improvement in pain relief (p<0.001) and statistically significantly faster return to work than did epicondylectomy alone (p<0.001). Denervation plus epicondylectomy gave results that were the same as denervation alone.
Conclusion
It is concluded that denervation gives significant relief from LHE once traditional non-surgical treatment has failed.
Introduction
The treatment of “tennis elbow” or lateral humeral epicondylitis (LHE) begins with anti-inflammatory medications, alterations in activities of daily living, steroid injections, physical therapy, and counterforce splinting. When these approaches fail, surgical intervention may be appropriate. There is no currently accepted surgical approach to treat LHE, with available options including lengthening of the musculofascial origins of the wrist and finger extensors described by Nirschl in 1979 [13] and epicondylectomy described by Almquest in 1998 [1]. Sterling Bunnell, MD, the Father of Hand Surgery noted in 1944 that “operative methods are to stop the pull by severing the muscle at its origin. But the results hardly warrant their use routinely” [2]. Gardner, in 1947, was the first to describe the innervation of the elbow joint [7]. The anatomist and hand surgeon, Emanuel Kaplan, in 1959, was the first to describe elbow denervation [11]. He said that “although the actual pathology of epicondylitis is not known, it is suspected that the pain and weakness are associated with the complex nerve distribution of the region, and might be due to an irritating factor affecting these nerves”. Kaplan dissected 30 cadavers and had performed three clinical cases in which he resected branches from the radial nerve to humeral-radial joint. In Nirschl's approach [13], a chisel removes the origin of the extensor mass and raises the question as to whether his approach denervates the lateral humeral epicondyle. The same can be said about the resection of the epicondyle and muscle flap required in the Almquist approach [1], in which the anconeus muscle is rotated into the space previously occupied by the epicondyle.
Wilhelm, in 1958 [16] and in 1966 [17], described, in German, the innervations of the joints of the hand, which led to the treatment of wrist pain by “total wrist denervation”. In 1996, Wilhelm applied this concept to the treatment of LHE [18]. He obtained, “on average 90% success in cases of resistant tennis elbow…..denervation is accomplished blindly by disinsertion of certain muscles. The result of this procedure also depends on simultaneous indirect decompression of the posterior interosseous nerve.”
The Wilhelm approach also requires division of one or more branches from the radial nerve that went through the brachioradialis to the lateral humeral epicondyle.
The purpose of the current study was to compare the results of denervation of the lateral humeral epicondyle with and without an associated epicondylectomy to determine if the epicondylectomy was a necessary component of the surgical approach to the treatment of recalcitrant LHE.
Methods and Materials
A retrospective evaluation was done on 45 patients who had been treated surgically for refractory LHE.
Inclusion criteria were patients who had more than 9 months of non-medical treatment for their LHE, including at least one cortisone injection into the extensor origin from the lateral humeral epicondyle. All patients had been given a trial of splinting with a counterforce brace. Presence of co-existing compression of the posterior interosseous nerve in the elbow region or of the radial sensory nerve in the forearm was not an exclusion criterion.
Exclusion criteria were presence of an underlying medical contraindication for surgery, previous elbow fracture, presence of a tumor or ganglion in the region of the elbow, and a history of a bleeding disorder.
Stratification of the 30 patients who were treated surgically for refractory LHE is as follows: group 1 consisted of 17 patients who were treated with epicondylectomy, group II consisted of seven patients who were treated with lateral epicondylectomy and neurectomy, and group III consisted of seven patients who were treated with neurectomy (denervation) alone. Demographics are given in Table 1.
Demographics

For the denervation group, there had to be a decrease of at least five points on the visual analog scale (VAS) after a local anesthetic blockade of the posterior branch of the posterior cutaneous nerve of the forearm at a site 2–3 cm proximal to the lateral humeral epicondyle.
Co-existing compression of the radial nerve existed in two patients in group I, one patient in group II, and one patient in group III.
One group of surgeons (RR and MN), who have used lateral humeral epicondylectomy to treat LHE, incorporated the concept of denervation in 2006 into their treatment approach and included a group of patients with recalcitrant LHE who had epicondylectomy alone (17 patients), a group of patients who had denervation alone (1 patient), and a group of patients who had both an epicondylectomy and a denervation done simultaneously (7 patients). The remaining surgeon (ALD) contributed six patients who did not have an epicondylectomy, but who had just a resection of the posterior branch of the posterior cutaneous nerve of the forearm, beginning in 2004. None of these patients had prior surgery to treat their LHE.
Outcome analysis was based upon change in the pain level as determined by a VAS and on time to return to work, as this relates to time required for rehabilitation and recovery of function. Statistics included a Chi-square analysis and Student's t test.
Surgical Technique
For all patients, general anesthesia, a pneumatic tourniquet, loupe magnification, and bipolar coagulation were employed.
The lateral humeral epicondylectomy was performed by placing a 4-cm incision just anterior to the lateral epicondyle. The tissues are bluntly dissected to expose the bony prominence. Cauterization of the periosteum and soft tissues exposed the cortical bone. A straight osteotome was used to decorticate the epicondyle at the origin of extensor musculature. Careful attention was taken not to damage the collateral ligament or enter the joint space. Hemostasis was completed, and the wound was irrigated and closed in layers (Fig. 1).
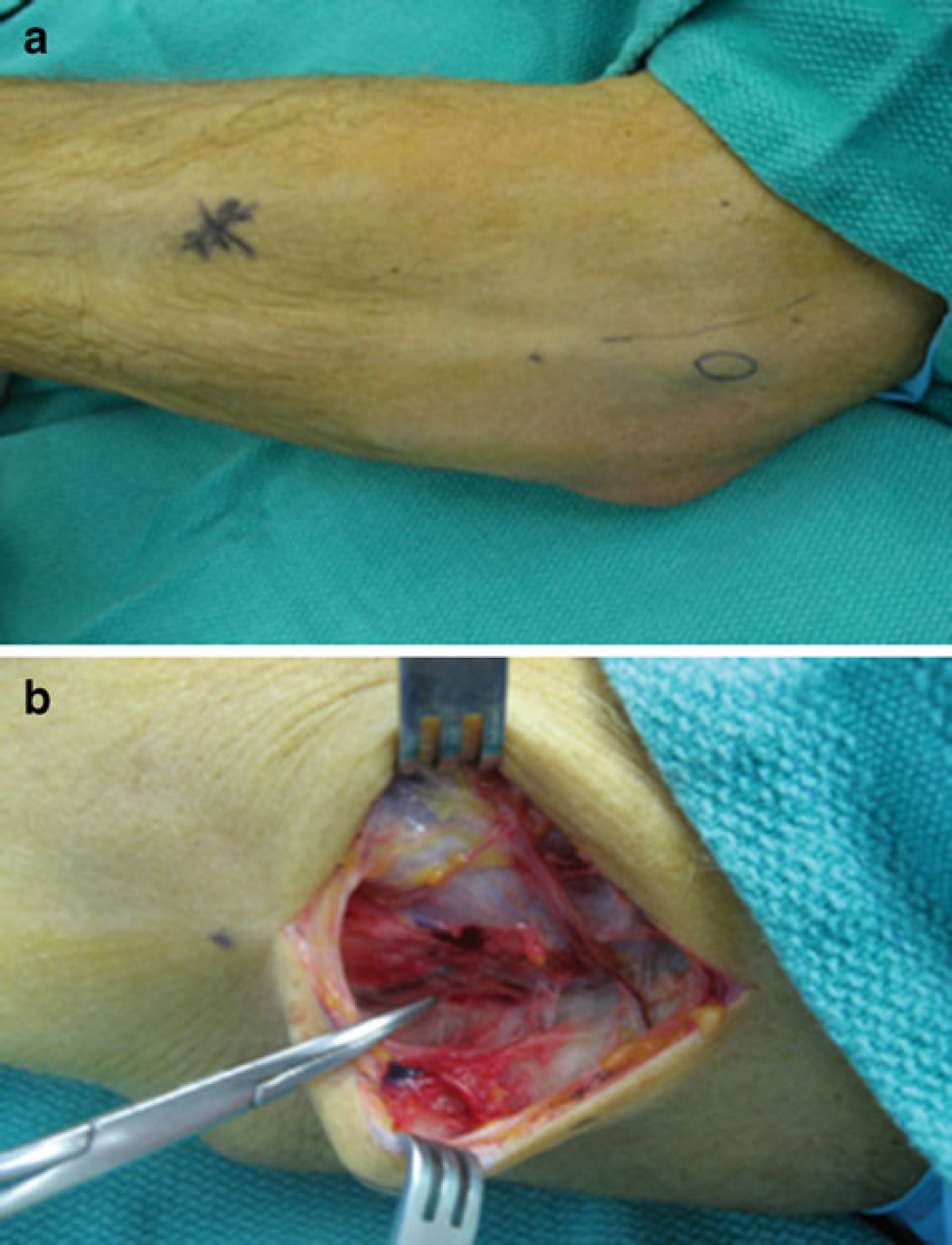
Surgical technique for epicondylectomy.
The denervation of the lateral humeral epicondyle was done through an incision that was 4–7 cm in length, depending upon the girth of the arm. This incision was begun just proximal to the lateral humeral epicondyle and extended proximally along the midlateral line of the arm [5]. The posterior cutaneous nerve of the forearm was identified and preserved [3] (Fig. 2). One or more posterior branches were identified traveling towards the lateral humeral epicondyle and were resected, then dissected proximally and implanted into either the brachioradialis muscle proximal to the elbow or into the lateral head of the triceps muscle, depending upon the regional anatomy and how far proximally these posterior branches could be dissected while preserving the branch to the forearm. (If the branch to the forearm was found to have been injured by previous surgery, creating a painful neuroma, then, the entire posterior cutaneous nerve of the forearm should be resected [3]. Fig. 3).
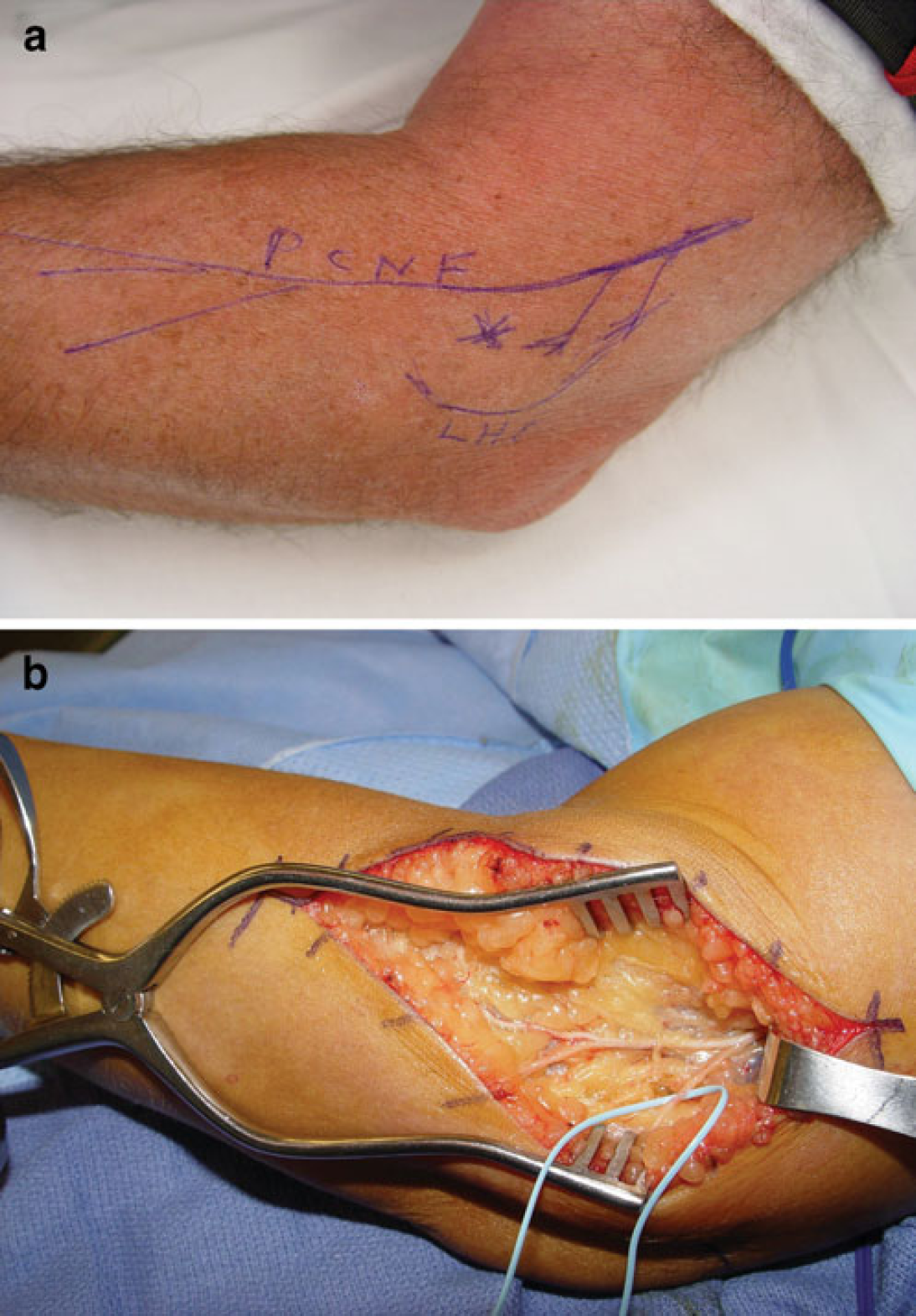
Anatomy of the posterior cutaneous nerve of the forearm in the left arm.
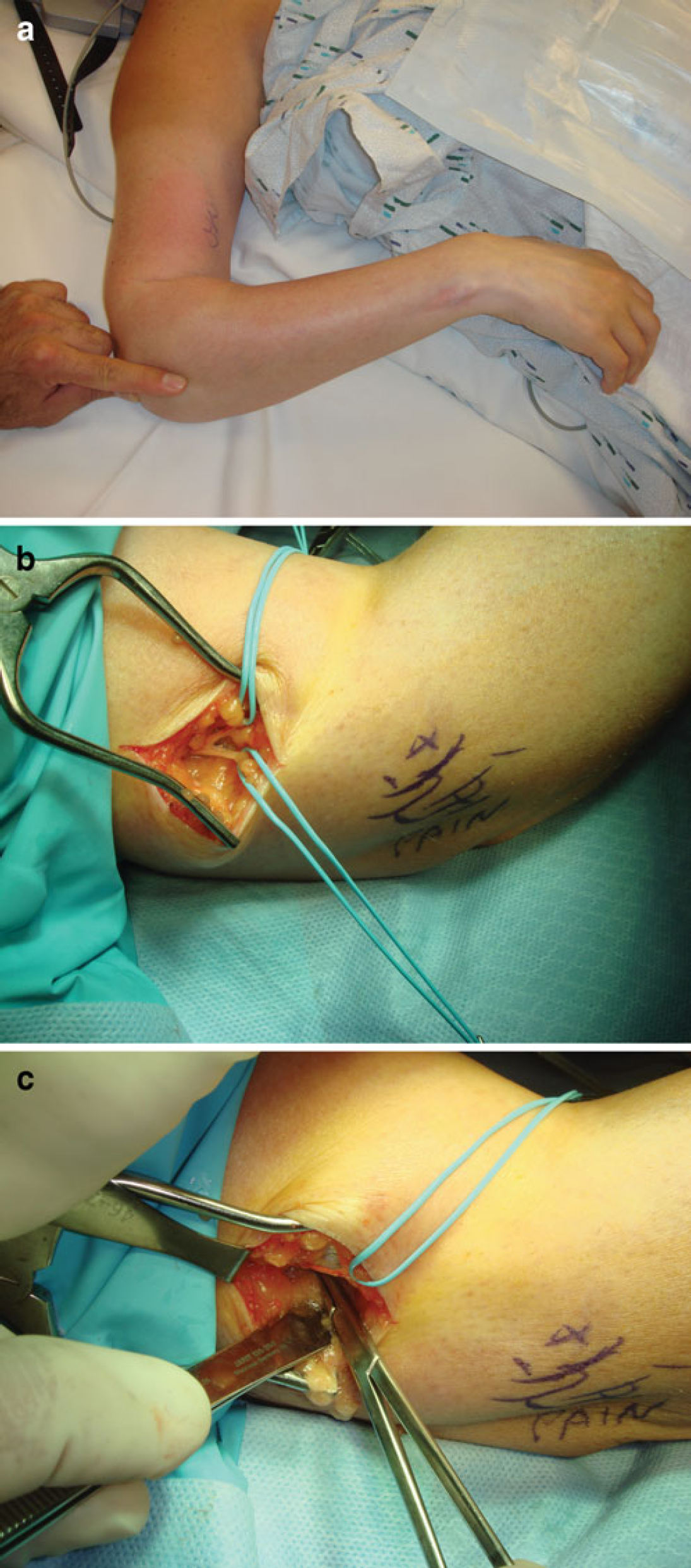
Surgical technique for denervation of the lateral humeral epicondyle.
Neurolysis of the posterior interosseous nerve, when existing in these patients, was done as previously described [6,9,12,14].
Results
Post-operative follow-up was a mean of 7.5 months in the group with epicondylectomy alone, 16.0 months in the group with both epicondylectomy and denervation, and 16.3 months in the group with denervation alone.
While there was an improvement in patients whose LHE was treated by epicondylectomy alone, those patients who were treated with denervation alone improved significantly more than those who had epicondylectomy alone (mean VAS of 5.1 versus mean VAS of 0.5, p<0.001). Patients who had epicondylectomy plus denervation did not demonstrate an improvement significantly more than those who had just epicondylectomy (mean VAS of 1.3 versus mean VAS of 5.1, p=0.067), and this was probably due to the study being underpowered.
Patients who had denervation alone had a significantly faster return to work than did those who had an epicondylectomy (mean return to work 41 days versus mean of 125 days, p<0.001). Those who had an epicondylectomy plus denervation returned to work significantly faster than those who epicondylectomy alone (mean return to work of 42 days versus mean of 125 days, p<0.001).
Analysis of the three groups demonstrates that there was no significant difference in the proportion of patients who had a neurolysis of the posterior interosseous nerve in each group (p>0.05).
Discussion
The results of this retrospective analysis demonstrate that while symptoms of refractory LHE can be successfully treated by lateral humeral epicondylectomy, this success may be achieved through the denervation component of the epicondylectomy rather than the release of the common extensor muscle origins. The results of this study showed that the overall improvement in pain level is significantly better (p<0.001) in patients who had a denervation to treat refractory LHE compared to those who had just an epicondylectomy. Postoperative recovery from a denervation procedure is significantly quicker than from an epicondylectomy alone (p<0.001).
One of the limitations of this study is that it is retrospective, and therefore, subject to bias in terms of which patients were chosen for epicondylectomy alone or epicondylectomy with denervation, or those with and without associated radial nerve entrapments. The observations of the present study support a prospective study in which the design includes an approach to the confounding variables associated with radial nerve entrapment. Another limitation is the small number of patients in the different groups for denervation.
The inclusion of patients who had a simultaneous neurolysis of the posterior interosseous nerve does not affect the conclusions of the study because these patients were included in all three patient groups to a degree that was not significantly different in each group (p>0.05). While some authors have indicated that symptoms of LHE can be due to compression of the posterior interosseous nerve in the region of the elbow [4,8,9,15], other authors have not found this to be true [10,15]. It is our belief that these nerve compressions are secondary to the use of the counterforce brace during the initial months of treatment of the LHE. Symptoms of radial nerve compression at the region of the elbow include those of aching or pain proximally along the humerus, wrist aching (due to the terminal branch innervating the dorsal wrist capsule), but do not include complaints related to the lateral humeral epicondyle.
The denervation procedure described in our approach is different in concept from the one proposed by Wilhelm. The approach described here just resects the posterior branch of the posterior cutaneous nerve of the elbow to the lateral humeral epicondyle.
In contrast, in an attempt to treat all branches of the radial nerve at the elbow, Wilhelm decompresses the radial nerve, resects branches of the radial nerve that course through the brachioradialis to the epicondyle and radial–humeral joint, disinserts the origin of the supinator from the epicondyle as well as releasing the extensor tendon origins, and also resects the posterior branch of the posterior cutaneous nerve of the forearm [17].