
Abstract
Background
One of several operations to correct abduction deformity of the little finger, (Wartenberg's sign) in ulnar nerve palsy, is a combined procedure that radializes the extensor digiti minimi (EDM) at the level of the fifth metacarpophalangeal (MCP) joint and reroutes it from the fifth to fourth extensor compartment. This cadaveric study was designed to investigate the impact of both elements on adduction.
Materials and Methods
Anatomy of the little finger extensor apparatus was studied in 16 freshly frozen cadaver hands sectioned at mid forearm. We observed little finger motion after different modifications of the EDM. We tested the effect of a rerouting maneuver by pulling on the EDM, as well as radialization of the EDM alone and in combination with rerouting.
Results
The EDM was present in all cases. Little finger extensor digitorum communis (EDCV) was missing in two cadavers. In no case was adduction created by rerouting the EDM to the fourth compartment. Radialization of the EDM corrected the abduction deformity beyond the axis of abduction/adduction of the fifth MCP joint in 13 cases and only up to it in three cases. In one of the three with limited correction, a rerouting maneuver allowed for further adduction.
Conclusion
The key to correct abduction deformity of the little finger is radialization of the EDM, which can be done through a solitary incision at the level of the MCP joint. Rerouting alone does not correct the abduction deformity, and in combination with radialization it does not predictably enhance the correction.
Introduction
Permanent abduction of the little finger can be bothersome, impeding insertion of one's hand into a glove or pocket. It was described by Wartenberg [11] in 1930 in the context of ulnar nerve palsy in two patients; one suffered from a neuritis of the ulnar nerve and the other from the sequelae of a traumatic ulnar nerve lesion in the arm. As the extensor digiti minimi (EDM) has the potential to abduct the little finger through its indirect attachment onto the abductor tubercle of the proximal phalanx [2], the Wartenberg's sign can result from high and low ulnar nerve palsies. Other causes for an abduction deformity of the little finger have been described and include traumatic avulsion of the third palmar interosseous muscle [5], necrosis, and contracture of the hypothenar muscles such as occurring after tight plaster application [8], closed ligament injury of the radial collateral ligament, and the connexus intertendineus IV/V [8] in association with a lax palmar plate [9]. Rheumatoid arthritis is also known to cause abduction deformity of the little finger.
A number of different operations have been proposed to address the deformity of the extensor apparatus of the little finger in ulnar nerve palsy. In 1976, Blacker [2] described a technique named the Fowler-Brooks transfer, in which the ulnar-most slip of the EDM is transferred to the volar radial side and inserted into the flexor tendon sheath. This operation was preferred if, in addition, there was clawing of the little finger. Blacker [2] described a second technique which he applied when clawing was absent, transferring the ulnar-most half of the EDM into the radial collateral ligament of the metacarpophalangeal (MCP) joint of the little finger. In 1991, Dellon [3] described transposition of the ulnar slip of the EDM to the radial side of the extensor hood, and in 1998 Bellan [1] proposed a rerouting transfer of the EDM from the fifth into the fourth compartment in association with radial transposition of the EDM, in the belief that rerouting modified the leverage on the little finger [1]. A limited amount of research has been performed on the effect of this combined operation in the cadaver hand [1].
The objective of our study was to investigate the impact on adduction of the two components of the rerouting and radialization operations [1], separately and in combination. Additionally, we studied the anatomy of the extensor tendons and compared it to previously published anatomical observations.
Material and Methods
Sixteen fresh cadaver hands (ten right hands and six left hands) were utilized for the study, and no routine X-ray analysis of the specimens was performed. We dissected the extensor apparatus of the little finger and studied its anatomy, looking particularly at the number of EDM slips and existence of the fifth extensor digitorum communis (EDCV). We recorded the position of the slips of the EDM tendon regarding the center of axis of abduction/adduction of the fifth MCP joint.
The forearm was stabilized on the dissection table with the dorsum of the hand upwards in a neutral position with regard to the radiocarpal axis of abduction/adduction. Subsequently, we made a series of modifications within the extensor apparatus of the little finger (Fig. 1). We first rerouted the EDM from the fifth extensor tendon compartment to the fourth by sectioning the wall between the fourth and fifth compartments, which was closed afterwards with forceps to ensure the transfer. We measured the deviation of the angle created by rerouting the EDM to the fourth extensor compartment. Secondly, we removed the forceps and transferred the EDM back into the fifth extensor compartment and secured its position by closing the intercompartmental wall once again with forceps. Then both strips of the EDM were tenotomized and transposed to the radial side of the extensor apparatus of the little finger, where they were attached to the extensor digitorum communis (EDC) by a side-to-side suture. In cases where the EDCV was absent, we tenotomized the EDM, advanced it, and sutured it side by side to the radial side of itself. Lastly, we added a rerouting transfer to the radialized EDM, once again ensuring its position by closing the intercompartmental wall with forceps. At the beginning and following each modification, we positioned the little finger in abduction and pulled with maximal strength on the EDM tendon. We observed little finger motion and the ability to correct abduction up to, or beyond, the center of the axis of abduction/adduction of the fifth MCP joint.
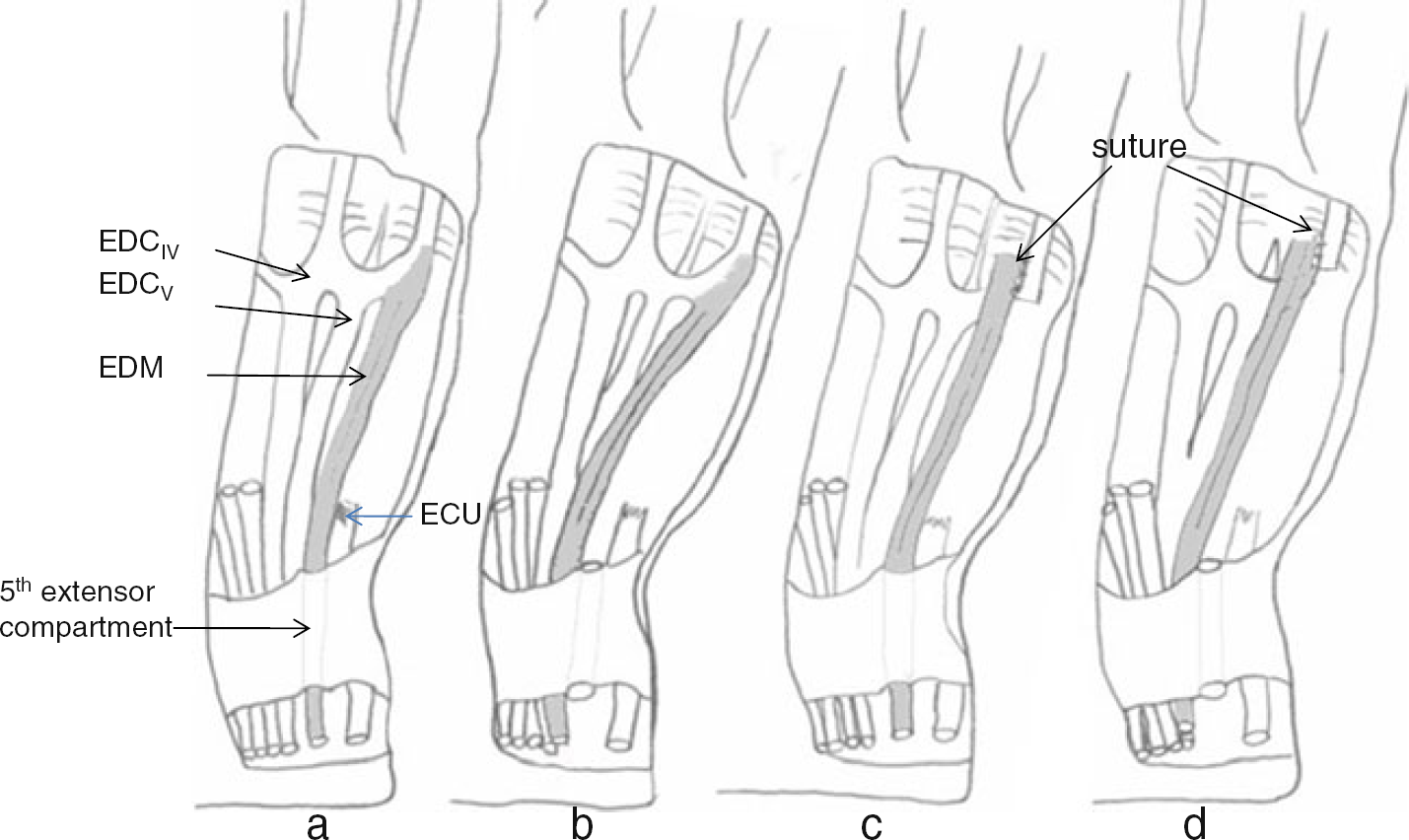
The different modifications within the extensor apparatus of the little finger.
Results
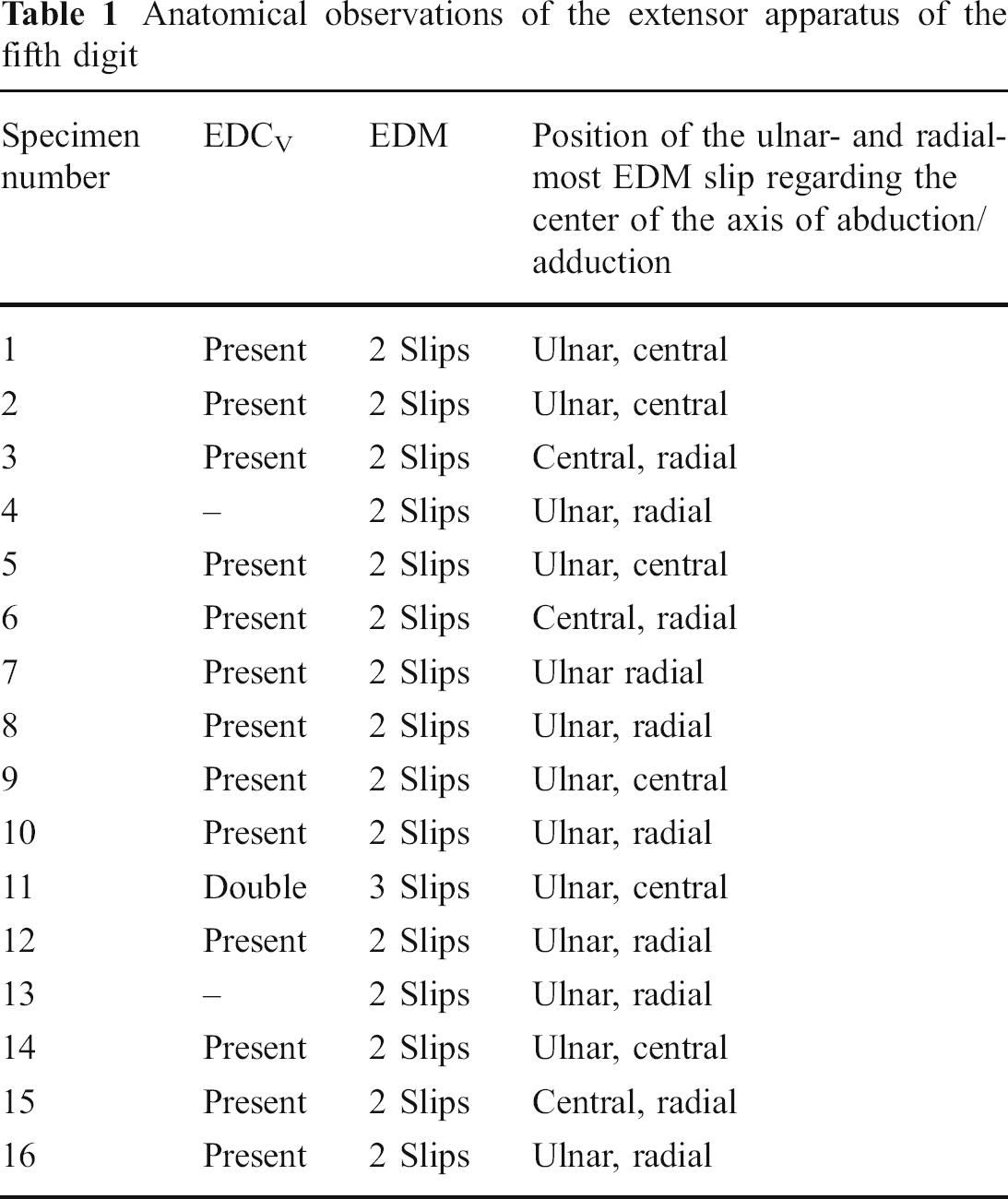
The anatomical observations of the extensor apparatus of the little finger in 16 cadavers are shown in Table 1. In two (12%) specimens, the EDCV was missing, but a connexus intertendineus was present. In one specimen, the EDCV was doubled. The EDM was present in all cases, with two tendon strips found in 15 cases and a triple strip in one specimen. The ulnar-most strip of the EDM was ulnar to the center of the axis of abduction/adduction of the fifth MCP joint in 13 cases and passed directly over the center in the remaining three cases. The radial-most strip of the EDM was radial to the center of the axis of abduction/adduction in ten cases, and in the remaining six specimens it passed directly over the center (Fig. 2). The functional observations that were noted following modification within the extensor apparatus of the little finger are shown in Table 2. Prior to modifying its position, a pull on the EDM resulted in abduction of the fifth digit in all cases. A solitary rerouting maneuver did not correct abduction in any of the specimens. The modification of the course of the EDM after rerouting was between 8° and 10°. Radialization of only the EDM itself (Fig. 3) corrected abduction beyond the center of the axis of abduction/adduction of the fifth MCP joint in 13 cases. In these 13 cases, the combination of radialization and rerouting of the EDM did not further enhance adduction. In three specimens, adduction was possible only up to the center of the axis of abduction/ adduction by radialization of the EDM. In one of these three cases, the combination of radialization and rerouting created further adduction beyond the axis of abduction/adduction.
Anatomical observations of the extensor apparatus of the fifth digit
Functional observations after modification of the extensor apparatus of the small finger
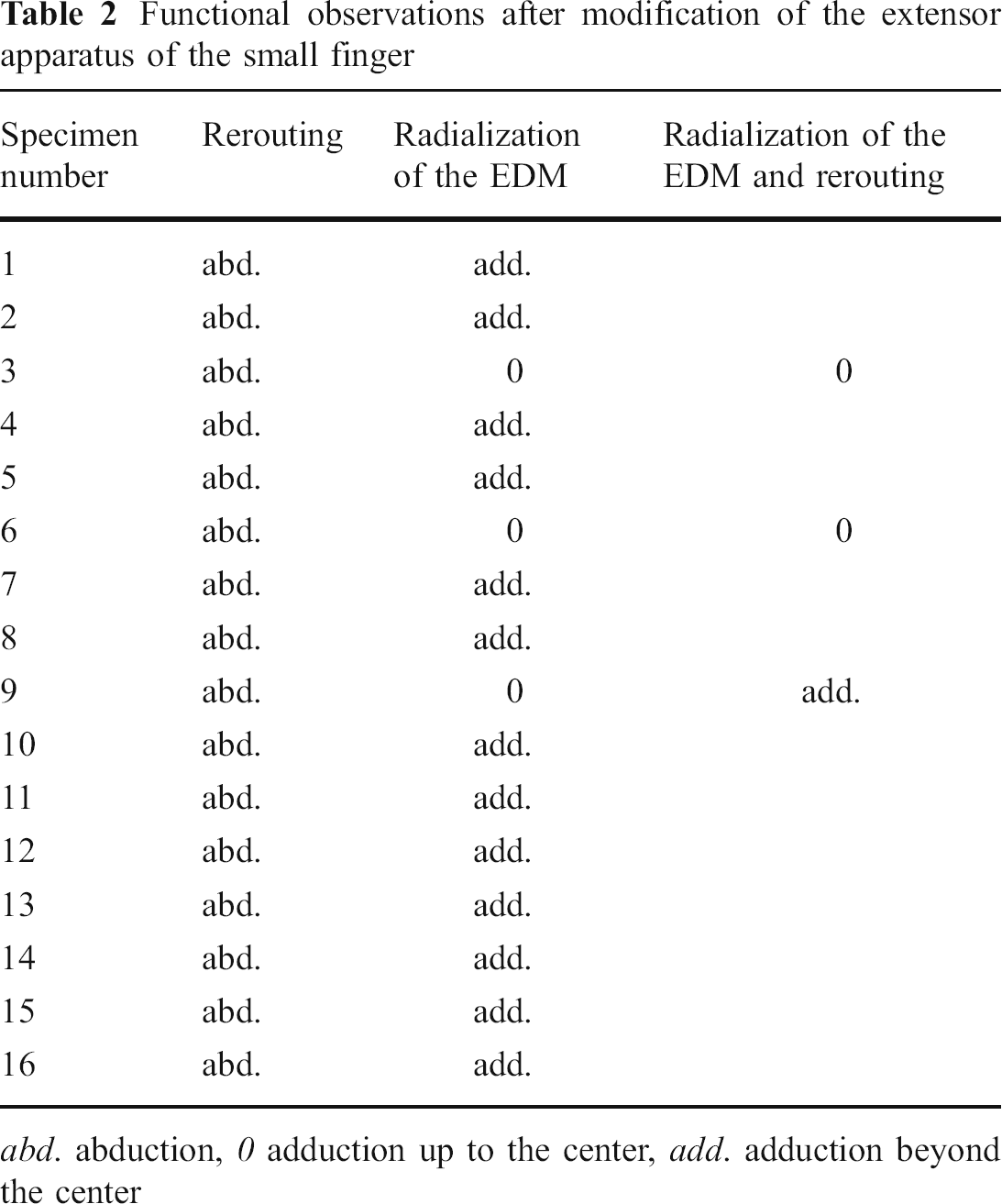
abd. abduction, 0 adduction up to the center, add. adduction beyond the center

The figure shows the anatomical findings.
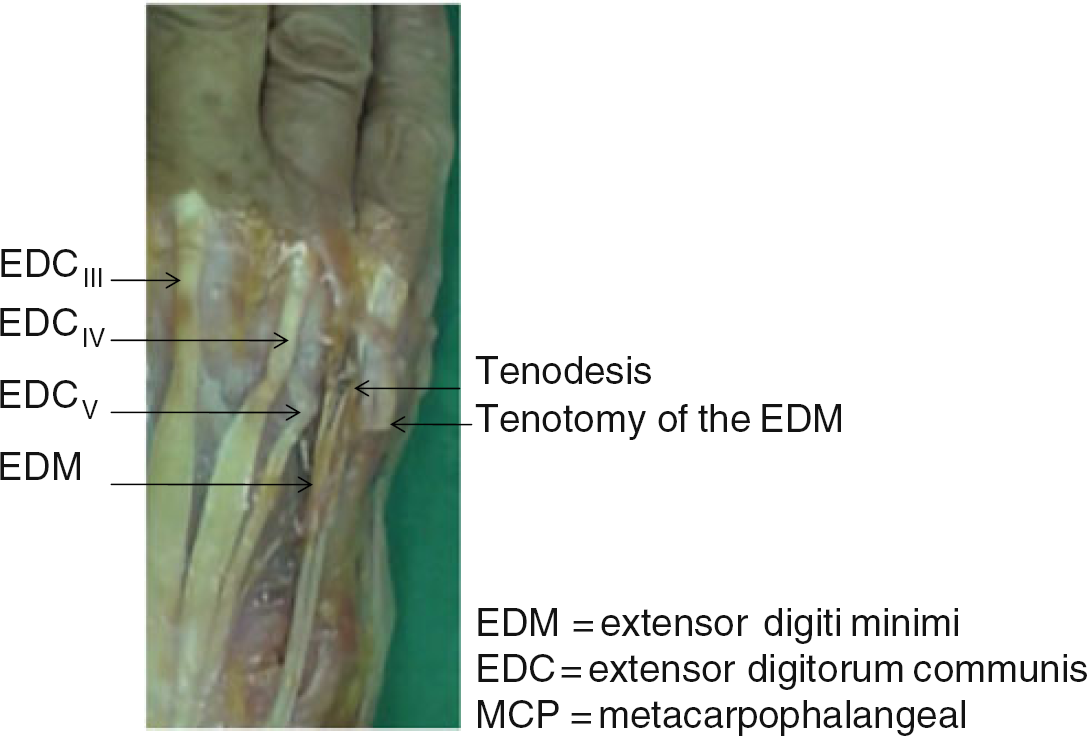
Radialization of the EDM at the level of the fifth MCP joint
Discussion
The occasional absence of the EDCV and presence of two tendon strips for the EDM in the majority of the cases corresponds to what has been previously reported [6]. In the majority of cases, the ulnar-most slip of the EDM passed ulnar to the axis of abduction/adduction as mentioned above [2]. However, it remains unclear if this corresponds to the relationship in vivo once the tendons are under muscle tone. Before modification of its position, a pull on the EDM resulted in abduction of the fifth digit in all cases, even in the three cases where the ulnar-most strip of the EDM was directly over the center of the axis of abduction/adduction of the fifth MCP. This observation is explained by the fact that the ulnar-most tendon strip passes around the ulnar border of the metacarpal head to gain attachment to the tendon of the abductor digiti minimi [2]. This also explains why, in all specimens, a solitary rerouting maneuver failed to correct the deformity. Correction of abduction at least up to the axis of abduction/adduction of the fifth MCP joint could be achieved in all cases by radialization of the EDM itself. Thus, the key point in correcting the abduction deformity is radialization of the EDM at the level of the fifth MCP joint. Once the EDM is radialized, a rerouting maneuver can add further adduction. In one of three cases where radialization of the EDM only corrected the abduction deformity up to the center of the axis of abduction/adduction of the fifth MCP joint, rerouting resulted in further adduction. However, we could not identify any specific reason to account for the unpredictability of the rerouting. The satisfying results reported by the combined radialization/rerouting operation [1] in five cases might be due largely to changing the lever by radialization and not to rerouting. Changing the lever of the EDM has been successfully performed by different techniques. Blacker [2] reported the results for two techniques in eight patients. He noted satisfying results in four patients where the ulnar-most slip of the EDM was transferred to the volar radial side with insertion into the flexor tendon sheath. He also found good results in four patients where he transferred the ulnar-most slip of the EDM to the dorsal radial side with insertion into the phalangeal attachment of the radial collateral ligament of the MCP joint of the little finger. Dellon [3] reported successful results in ten of ten patients transferring the ulnar-most slip of the EDM into the radial extensor hood of the little finger.
Since we did not measure the force of adduction, we cannot exclude that it might be enhanced when rerouting is added to radialization. However, since we already mentioned that in two of three cases, the angular deformity could not be corrected; it seems unlikely that the adduction force would be predictably enhanced in the remaining cases. In addition, the concern is to correct the angular deformity and not the force of adduction.
Finger movements are dependent upon balancing flexor and extensor forces, which is difficult to reproduce in cadaver studies. However, we conclude that in our clinical practice, correction of the Wartenberg's sign should be performed only by radializing the EDM at the level of the MCP joint according to one of the previously described techniques [2,3] and not to add a rerouting maneuver.
One should keep in mind that the abductor digiti minimi may be paralyzed in ulnar nerve palsy, and transposing the EDM might remove the last muscle with an abduction moment and lead to loss of abduction. In such cases, the deformity can be corrected by using an extensor indicis [7] transfer, a tenodesis [4], or a transfer of the EDCIV [10].
Footnotes
Acknowledgement
We thank Dr. Richard Stern from the University Hospital of Geneva for assistance in preparation of the manuscript.