
Abstract

Introduction
Minimally displaced scaphoid fractures may be treated effectively with non-operative treatment strategies [1,6]. However, delayed diagnosis of a scaphoid fracture may frequently lead to non-union, especially if the fracture is in the proximal portion of the scaphoid [4,11]. Proximal pole scaphoid fractures commonly result in non-unions secondary to disruption of the retrograde blood flow. Although proximal pole scaphoid fractures may heal spontaneously, the fracture location leads to non-union in the majority of the cases without surgical intervention.
Based on our literature review, there has not been a report of spontaneous healing of an established proximal pole scaphoid non-union. Here, we present an unusual case of healing of a proximal pole scaphoid fracture without surgical intervention or immobilization.
Case
A 23-year-old right-hand-dominant male sustained an injury to his non-dominant left wrist during an ultimate Frisbee match in May 2005. The patient self-diagnosed his injury as a simple wrist sprain and did not seek treatment. In August 2005 (3 months after initial injury), the patient sought consultation as he continued to have wrist discomfort with activity. During his initial evaluation, his primary orthopaedist obtained radiographs which revealed a proximal pole scaphoid nascent fracture (Fig. 1). The patient declined treatment at that time due to personal reasons and was later referred for consultation to a hand surgeon.

Four views of the proximal pole scaphoid non-union 3 months from injury
The patient was evaluated at our institution 6 months after his initial injury (November 2005). He had mild tenderness in the anatomic snuffbox but no evidence of instability based on provocative testing of the scapholunate interval (Watson's shift test, scapholunate ballottment test). The patient's range of motion was only slightly decreased in extension (60° versus 70° for the contralateral wrist) and radial deviation (20/25). On physical exam, no gross carpal instability was present. Wrist flexion and ulnar deviation were symmetrical. Radiographs confirmed the scaphoid non-union. An MRI was obtained, which confirmed nonunion of the proximal pole scaphoid with heterogeneous T1 signal throughout the scaphoid, including the proximal pole. The non-union site was clearly delineated (Fig. 2).
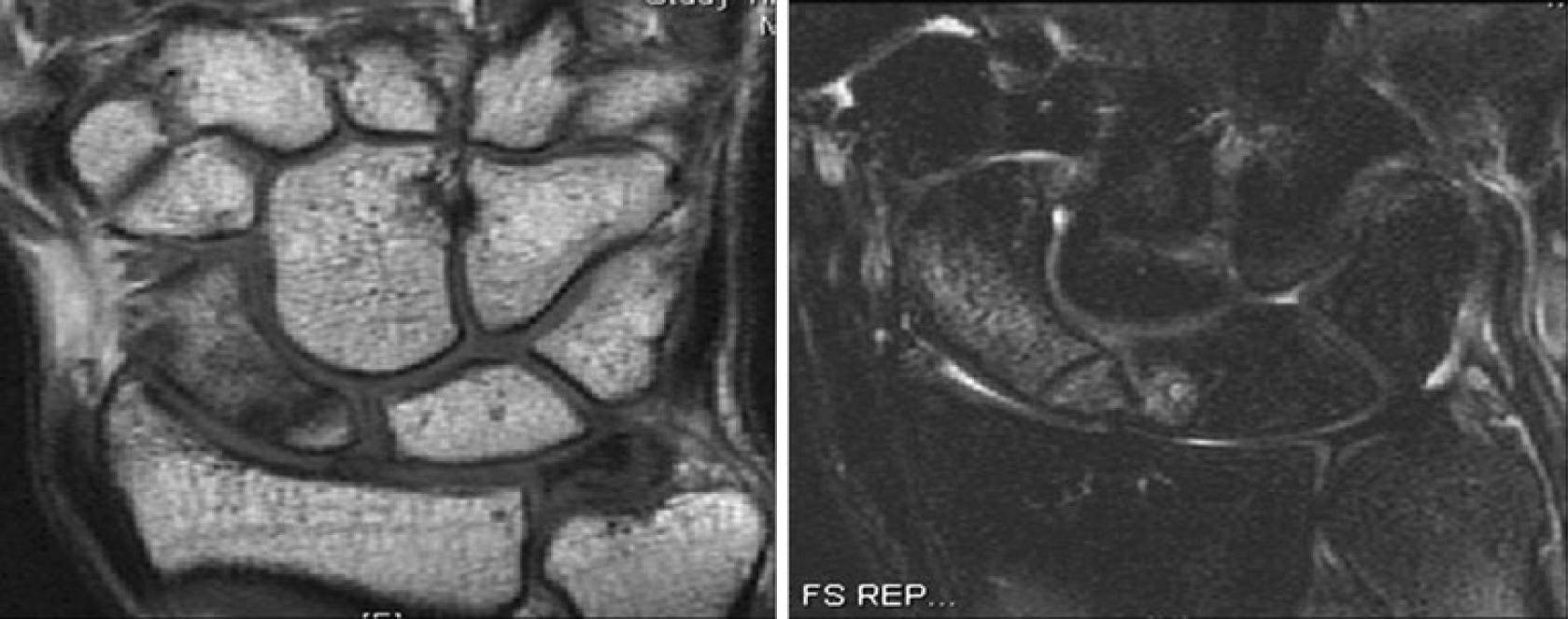
MRI of the proximal pole scaphoid non-union revealing heterogeneous T1 (left) and T2 (right) signal 6 months from injury
With clear evidence on MRI of a proximal pole scaphoid non-union, surgical options were discussed, including fixation with autogenous bone graft versus vascularized bone graft. The patient considered his options and due to personal issues decided against surgery at that time. He also declined any form of wrist immobilization.
The patient was lost to follow-up but returned 18 months later (May 2007). He had fallen onto his left (previously injured) wrist during a skiing accident. He was asymptomatic, but wished to have his wrist re-examined for safe measure. Radiographs were taken in the clinic, which revealed interval healing of the proximal pole scaphoid fracture (Fig. 3). No treatment was recommended. The patient followed up 6 months later (November 2007), and repeat radiographs and a CT scan were obtained that confirmed complete healing of the proximal pole scaphoid fracture with no evidence of avascular necrosis (Fig. 4). The patient was completely asymptomatic with full range of motion of the wrist.

Four views of spontaneously healed proximal pole scaphoid fracture 30 months out from injury

CT scan of scaphoid confirming union of proximal pole scaphoid fracture 30 months from injury
Discussion
The scaphoid is considered the cornerstone of the wrist representing the vital link between the proximal and distal carpal rows [12]. Of the carpus, the scaphoid is the most commonly fractured, with an incidence of greater than 345,000 per year [8]. Approximately 10% of scaphoid fractures fail to heal and become non-unions [3]. Due to the vascularity of the scaphoid, proximal pole fractures have a particular predisposition towards this complication [2,3].
The wide body of literature on proximal pole scaphoid non-unions advises aggressive operative treatment for these types of fractures [5,11,12]. The above described case report is the first documented report of spontaneous healing of a proximal pole scaphoid non-union with no form of treatment. Based on a thorough English literature search, there is only one other case of spontaneous healing of a fractured scaphoid which describes a symptomatic distal pole scaphoid fracture uniting after 3 years in a 19-year-old farmhand [9]. That patient showed no evidence of osteoarthritis or avascular necrosis at his 3-year follow-up nor did our patient at his 30-month follow-up.
Our case is interesting in terms of the imaging modalities that were utilized in this patient's assessment and the possible predictive value based on retrospective analysis. Close inspection of the initial consultation radiographs revealed clear evidence of an old scaphoid proximal pole fracture and sclerosis surrounding the fracture site (Fig. 1).
However, the radiodensity of the proximal pole appears very similar to the waist and distal pole. In addition, the MRI demonstrated normal fat signal proximal to the fracture site (Fig. 2).
Morgan et al. evaluated the significance and role of magnetic resonance imaging in assessing factors affecting healing in scaphoid non-unions [7]. There were three groups that were delineated in the study with respect to scaphoid non-unions. Group 1 had normal trabecular bone radiographically and vascular bone marrow on magnetic resonance imaging and was expected to heal after surgery. Group 2 had normal trabecular bone radiographically but avascular marrow on MRI and was expected to have delayed healing after surgery. Group 3 had abnormal radiographs and avascular bone on MRI and was expected to fail to show healing. The patient in our case study would likely have been classified in group 1 at 6 months from the injury. Our initial assessment with MRI was based on the fact that the patient presented to our clinic 6 months after the injury and showed clear x-ray evidence of non-union. An MRI was obtained to evaluate the vascularity of the proximal pole. A CT scan at that point would have provided less information compared to an MRI.
Smith et al. also evaluated scaphoid non-unions utilizing computed tomography [10]. This study revealed increased radiodensity of the proximal pole and absence of any converging trabeculae between the fracture fragments as the most significant determinants of avascular necrosis. On the initial evaluation of this patient, T1-weighted MRI revealed minimal bridging trabeculae, and there was evidence of increased radiodensity on the plain radiographs.
After close inspection of the radiographs and MRI, the patient had several factors that positively weighed in on a more favorable outcome. In addition, the patient was young, a non-smoker, had type 2 lunate with a minimally displaced scaphoid fracture, did not show any evidence of carpal instability, and was pain-free. Treatment was refused by this patient, and more than 1 year was necessary to achieve radiographic proof of union. The intent of this report is not to advocate non-treatment of proximal pole scaphoid fractures and non-unions but to note that in isolated cases, spontaneous healing may occur.