
Abstract
Introduction
Soft tissue metastases to the hand are rare with studies suggesting an incidence of 0.2% among patients treated for cancers [9]. This paper describes the case of a 67-year-old male presenting with hand pain several years after treatment for a primary basal cell adenocarcinoma of parotid gland origin. Investigations confirmed what is believed to be the first documented case of parotid basal cell adenocarcinoma metastasizing to the hand. A description of the challenges faced in the treatment of this aggressive malignancy presents the opportunity to discuss key factors that must be considered when formulating management plans for similar presentations.
Case Report
A 67-year-old right-handed male presented to hand clinic complaining of a 4-month history of gradually worsening pain and swelling over the dorsum of his left hand. Relevant past medical history included a diagnosis of parotid basal cell adenocarcinoma treated with complete resection and local radiotherapy 2 years previously. There was no other history of malignancy, and the patient was asymptomatic following his initial treatment.
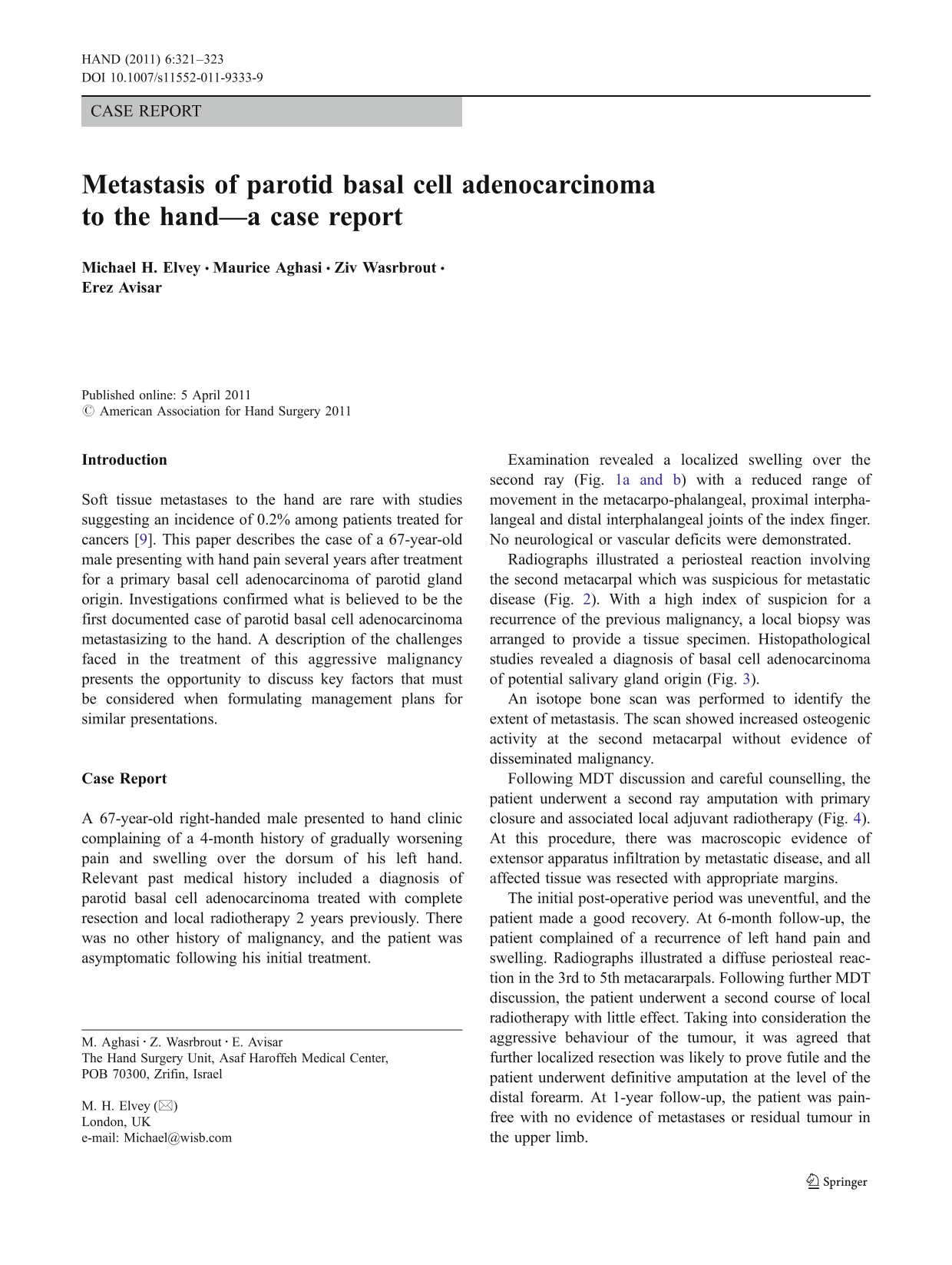
Examination revealed a localized swelling over the second ray (Fig. 1a and b) with a reduced range of movement in the metacarpo-phalangeal, proximal interphalangeal and distal interphalangeal joints of the index finger. No neurological or vascular deficits were demonstrated.
Pronounced dorsal swelling over the 2nd metacarpal
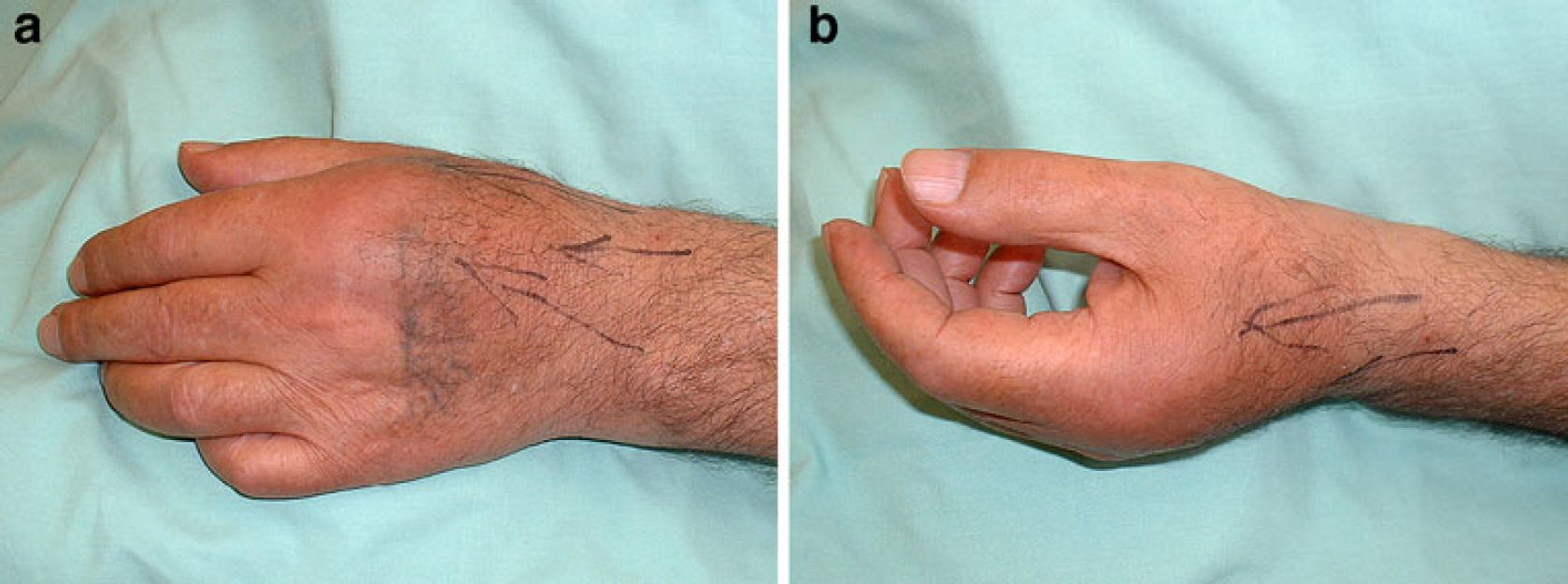
Radiographs illustrated a periosteal reaction involving the second metacarpal which was suspicious for metastatic disease (Fig. 2). With a high index of suspicion for a recurrence of the previous malignancy, a local biopsy was arranged to provide a tissue specimen. Histopathological studies revealed a diagnosis of basal cell adenocarcinoma of potential salivary gland origin (Fig. 3).

Pre-operative plain radiographs (AP and Oblique) illustrating radiolucency and irregularity of the second metacarpal with associated soft tissue swelling
H&E section from left 2nd metacarpal demonstrating solid cell nests with associated vesicular nuclei and nuclear pleomorphism. Moderate cytological atypia is seen in conjunction with significant mitotic activity—
An isotope bone scan was performed to identify the extent of metastasis. The scan showed increased osteogenic activity at the second metacarpal without evidence of disseminated malignancy.
Following MDT discussion and careful counselling, the patient underwent a second ray amputation with primary closure and associated local adjuvant radiotherapy (Fig. 4). At this procedure, there was macroscopic evidence of extensor apparatus infiltration by metastatic disease, and all affected tissue was resected with appropriate margins.

Post-operative plain radiographs (AP and Oblique) demonstrating extent of 2nd ray amputation
The initial post-operative period was uneventful, and the patient made a good recovery. At 6-month follow-up, the patient complained of a recurrence of left hand pain and swelling. Radiographs illustrated a diffuse periosteal reaction in the 3rd to 5th metacararpals. Following further MDT discussion, the patient underwent a second course of local radiotherapy with little effect. Taking into consideration the aggressive behaviour of the tumour, it was agreed that further localized resection was likely to prove futile and the patient underwent definitive amputation at the level of the distal forearm. At 1-year follow-up, the patient was pain-free with no evidence of metastases or residual tumour in the upper limb.
Discussion
This study provides the first documented evidence of parotid basal cell adenocarcinoma metastasising to the hand and illustrates the danger of attempting limited clearance in the first instance.
Metastases to the hand from any primary malignancy are rare findings and typically present after the fifth decade with a male to female ratio of 2:1 [12]. The phalanges are most commonly affected followed by the metacarpals and carpals. There is no predominance among individual phalanges. Radiographic findings classically illustrate lytic lesions without a margin of sclerosis or joint involvement. Soft tissue swellings are very common and tend to present on the dorsum of the hand [7]. The differential diagnosis includes tuberculosis, osteomyelitis and primary musculoskeletal tumours including enchondromas and osteosarcomas.
The most common primary malignancies with a tendency to metastasise to the hand include pulmonary, breast and renal malignancies. The literature describes sporadic reports of rare primary malignancies metastasising to the hand including choriocarcinoma [1] and benign pleomorphic adenomas [3]; however, there are no reports of basal cell adenocarcinoma of the parotid gland behaving in such a manner.
Traditionally, the discovery of hand metastases has been associated with a poor prognosis representing aggressive and disseminated disease. Available treatment modalities include amputation and disarticulation with localized radiotherapy becoming more widespread in recent years. The key consideration when planning treatment is patient prognosis. In the palliative patient, surgeons must consider both the physical and psychological impact of an amputation and decide whether such an approach is in the best interests of the patient.
Basal cell adenocarcinomas were first described in 1978 and account for approximately 2% of salivary gland neoplasms [8]. They are classified as low-grade tumours with approximately 90% occurring in the parotid gland. The majority are thought to develop de novo; however, up to 25% may arise from pre-existing basal cell adenomas [6]. Four major histological growth patterns are described: solid, tubulotrabecular, cribriform and membranous. The solid pattern is the most common and the most likely to present with perineural invasion. Whilst local recurrence rates are high (37%), long-term outcome following resection is favourable due to the rarity of both regional lymph node involvement and distant metastases (8% and 4%, respectively) [2,4,11]. Management of these tumours is controversial and in general follows the principles of treatment of other parotid malignancies. There is good evidence to support both total and superficial parotidectomy depending on individual tumour characteristics. Typically small low-grade tumours which fail to demonstrate local tissue invasion or evidence of regional lymph node involvement are suitable for superficial parotidectomy, and in all cases, post-operative radiation is recommended to reduce the high rates of local recurrence typically seen with these tumours [5,10].
In the subject case described above, the unusual finding of an isolated metastasis in a patient with a high quality of living and good life expectancy directed the surgeons towards an interventional strategy which failed in the first instance. Retrospectively, it may be argued that the recurrence following ray amputation and adjunctive radiotherapy might have been predictable and in keeping with the high local recurrence rates of primary basal cell adenocarcinoma of the parotid gland. This raises the question of whether the surgeon faced with a similar presentation should proceed with an extensive resection in the first instance when operative intervention is thought to be in the best interests of the patient.
This study is limited in its nature as a retrospective case report. A larger cohort and longer follow-up period is required before one may draw conclusions with regard to the natural history of metastatic parotid basal cell adenocarcinoma to the hand and its response to surgical resection. Nevertheless, as the first case of its type reported in the literature, and as evidence of the detrimental outcome of attempted conservative resection, these authors believe that this study can be of educational benefit to those involved in the management of complex hand surgery and bone tumours.
Footnotes
None.