
Abstract
Background
A multitude of operative approaches have been described for treatment of Dupuytren's contracture. A less-invasive technique of segmental fasciectomies performed through multiple small transverse incisions is presented.
Methods
Seventy-three digits in 37 patients were treated with segmental fasciectomies. The results of 34 digits in 14 patients are described with subsequent follow-up longer than 2 years.
Results
Metacarpophalangeal joint extension improved from a mean of 32.5° to 2.2°, while proximal interphalangeal joint extension improved from 22.9° to 4.1°. Patients subjectively rated their surgical outcomes as excellent or good in 91.2% of cases. No recurrence of the disease was noted, though extension of the disease to adjacent digits was observed in three patients.
Conclusions
Though this approach is technically demanding and requires the help of a skilled assistant, this preliminary study supports our contention that this less-extensive procedure allows excellent correction of contractures; results in mild postoperative pain; and permits a rapid return of finger flexion with satisfactory long-term results so far at 2-years follow-up.
Introduction
In 1834, Baron Guillaume Dupuytren advocated several essential principles in the operative treatment of the disease which bears his name, including: using transverse incisions in the skin creases, dividing the fascial bands, leaving the wounds open to heal by granulation, and splinting the digits in extension [6]. Over 170 years later, the operative treatment of Dupuytren's contracture continues to challenge hand surgeons, as the results of surgical intervention are sometimes suboptimal. Recurrences and extension of the disease are frequent, and the incidence of complications leading to morbidity can be high [2,7].
Several operative approaches which have been described in the hand surgery literature primarily vary in the design of the incisions and the management of the palmar fascia. The various approaches described include straight line incisions broken up by Z-plasties, Bruner's zig-zag incisions [3], Moermans' small curved incisions [9], multiple V–Y advancement flaps, and multiple transverse incisions.
The purpose of this study was to evaluate patients who had undergone a minimally invasive technique for contracture release using multiple transverse incisions, to report clinical outcomes following surgery, and to determine the overall complication rate of this technique. To our knowledge, the efficacy of using multiple transverse incisions has never been analyzed critically, although its use has clearly been described in the literature [8]. We report our preliminary findings with this technique.
Methods
From 2002 to 2005, 37 patients (73 digits) with Dupuytren's contracture underwent segmental fasciectomies through multiple transverse incisions. Of these 37 patients, 14 (34 digits) had subsequent follow-up longer than 2 years. The average duration of symptoms before surgery for these 14 patients was 13.1 years (range, 3–26 years). Seven of these patients demonstrated findings consistent with Dupuytren's diathesis with plantar fibromatosis, penile fibromatosis, knuckle pads, and a positive family history. The involved digits included 1 thumb, 2 index fingers, 7 middle fingers, 14 ring fingers, and 10 small fingers. Four of the 14 patients had undergone previous surgery and underwent revision surgery for recurrent disease using transverse incisions.
Preoperative and postoperative ranges of motion were carefully recorded with the use of a goniometer. The patients completed a questionnaire during their follow-up visits to evaluate their needs for postoperative pain medication, their occupational therapy requirements, the time to regain full finger flexion, and the patients' subjective assessments of their result. Patients were asked to rate their surgical outcomes as excellent, good, fair, or poor. Comparative analysis of the data was performed with the Student's t test. Statistical significance was achieved at a 95% level of confidence.
Surgical Technique
Surgery was performed as an outpatient under axillary block or Bier block anesthesia with an arm tourniquet. Transverse incisions (1–1.5 cm) were typically started over the distal palmar crease before proceeding distally as necessary to the metacarpophalangeal joint crease, the proximal phalanx, and the proximal interphalangeal joint crease to release the digit into full extension. The pretendinous cord was isolated from the overlying skin and from the underlying flexor tendon for a distance of approximately 1 cm proximal and distal to each incision. Special care was taken to identify and protect the common digital nerves in the distal palmar incision and the radial and ulnar digital nerves in the digital incisions. Segmental fasciectomies were then performed, occasionally leaving intermediate sections of diseased fascia undisturbed (Fig. 1). Once the affected digits could be released into full extension, the tourniquet was deflated and hemostasis achieved using bipolar electrocautery. The margins of the incisions were then loosely approximated using 4-0 nylon horizontal mattress sutures. The central portion of the incisions was often left open and was only closed primarily if there was no significant skin tension. Rarely, full-thickness skin grafts were used for larger skin defects over the proximal interphalangeal flexion crease.
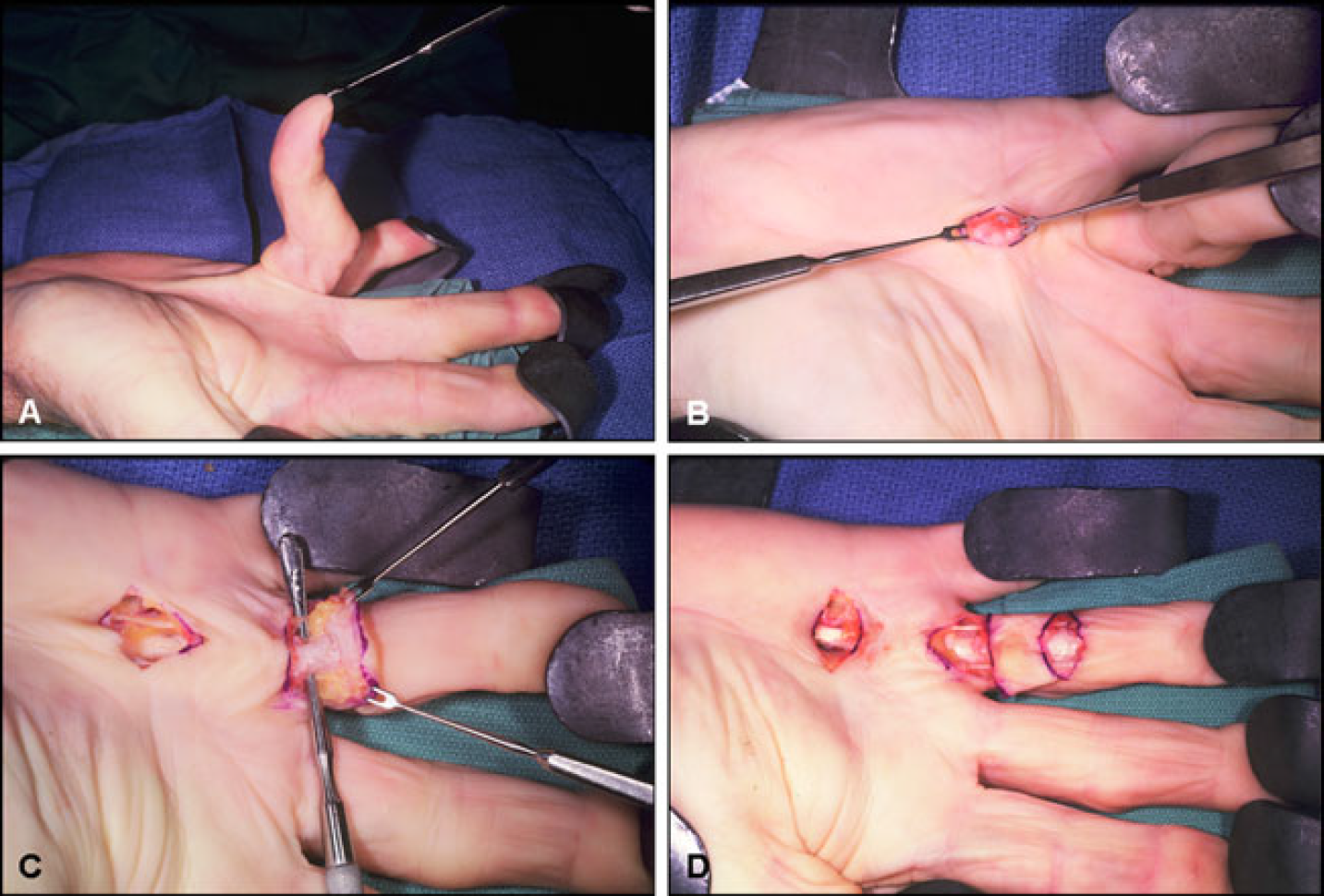
Dupuytren's contracture affecting the ring finger with a degree contracture of the metacarpophalangeal joint and a degree contracture of the proximal interphalangeal joint.
The affected digits were splinted in full extension at the metacarpophalangeal and interphalangeal joints before active mobilization was started 3 days postoperatively with a hand therapist. When skin grafts were utilized, mobilization was delayed until 10 days postoperatively.
Results
Preoperative contractures ranged from 0° to 85° at the metacarpophalangeal joint and from 0° to 90° at the proximal interphalangeal joint. The average contracture was 32.5° at the metacarpophalangeal joint and 22.9° at the proximal interphalangeal joint. Digital flexion was not found to be problematic, except in one patient whose proximal interphalangeal flexion was 10° shy of maximum in two affected digits. Segmental fasciectomies through multiple transverse incisions significantly improved metacarpophalangeal joint extension from a mean of 32.5° to 2.2° (p<0.01) and proximal interphalangeal joint extension from 22.9° to 4.1° (p<0.01) postoperatively.
Nine of 14 patients required narcotic pain medications following surgery. Seven patients (50%) required pain medications for 1 day only and had mild pain, according to a Dupuytren's contracture postoperative pain scale proposed by Gelberman et al. [7]. Two patients required pain medications for 7–10 days following surgery and had severe pain.
On average, patients only required 8.4 sessions of therapy to attain their maximal range of motion. Full flexion, defined as the ability to touch the distal fingertips to the distal palmar crease, was attained in under 4 weeks on average.
Patients rated their subjective outcomes of surgery for each involved digit. Twenty-five digits were rated as excellent, six as good, two as fair, and one as poor. The one patient who noted a poor outcome from surgery had undergone three previous procedures for recurrent disease. Using multiple transverse incisions in this patient's small finger improved metacarpophalangeal joint extension from 50° to 0° and proximal interphalangeal joint extension from 90° to 40°.
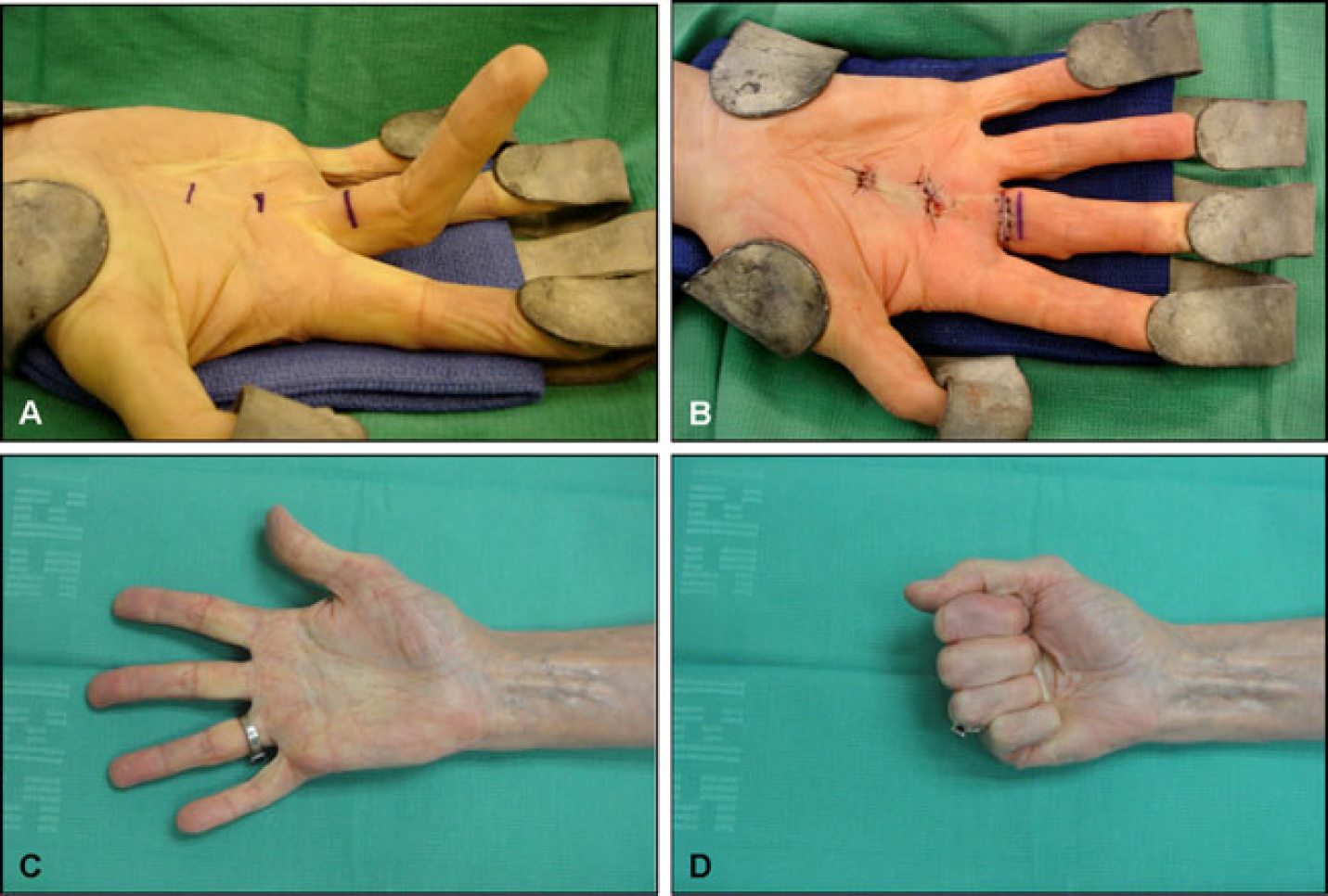
Two patients noted paresthesias in the operative digits for approximately 2 weeks, but ultimately regained full sensation of their digits. No recurrences have occurred in these patients so far with a minimum 2-year follow-up (Fig. 2), although three patients demonstrated extension of the disease to adjacent digits. We adopted the definition of recurrence and extension used by Tubiana and Leclercq [10]: Recurrence is the reappearance of Dupuytren's tissue in an area already cleared by surgery, in contrast to an extension which describes the appearance of diseased tissue in non-operated areas of the hand.
Intraoperative photographs demonstrating three transverse incisions for correction of Dupuytren's contracture.
Discussion
Based on our preliminary findings, a minimally invasive approach to correcting Dupuytren's contracture results in mild postoperative pain and allows patients to regain finger flexion rapidly. Although a higher recurrence rate would be expected using small transverse incisions and occasionally incomplete segmental fasciectomies, no recurrences have developed so far. Initial use of transverse incisions does not preclude conversion to Bruner incisions at the initial operation or if subsequent surgery becomes necessary.
However, segmental fasciectomies performed through multiple small transverse incisions is technically far more demanding for the surgeon and requires the help of a skilled assistant. The use of transverse incisions has been described as “dissecting under a bridge” [5] but is more like “dissecting through a tunnel”.
When compared to segmental fasciectomies performed through small curved incisions, our results appear to be comparable with respect to restoration of extension at the metacarpophalangeal joint and perhaps superior at the proximal interphalangeal joint (Fig. 3). Through small curved incisions, Moermans [9] reported metacarpophalangeal joint extension improved from 37.1° to 1.1° and proximal interphalangeal joint extension improved from 45.1° to 13.7°. However, these patients were only followed for less than 6 weeks on average (range, 2-30 weeks).
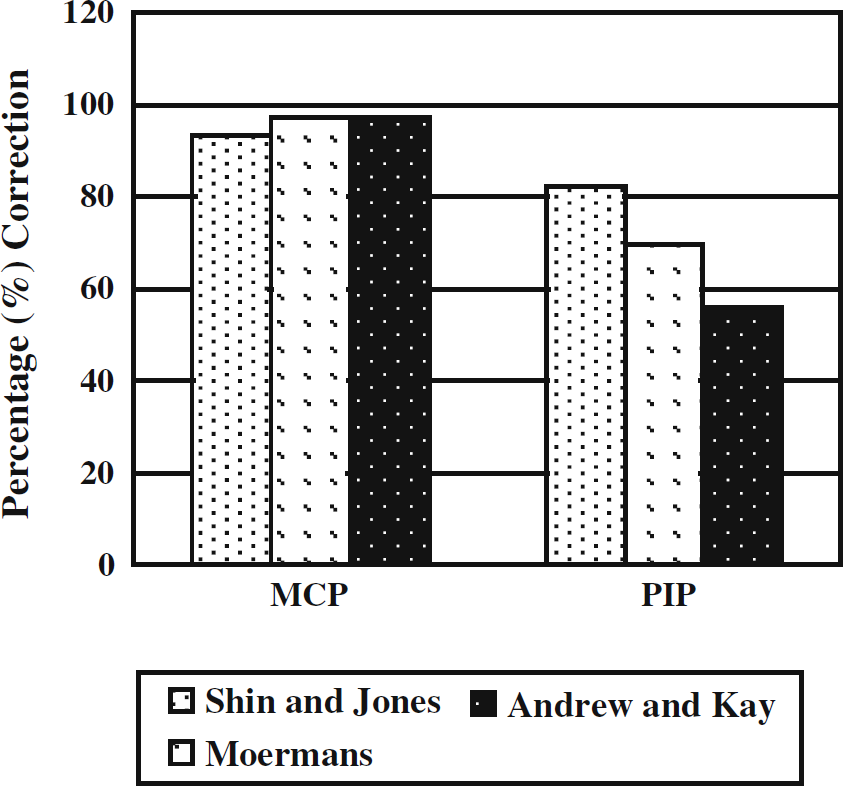
Using multiple transverse incisions, our preliminary results are comparable to those published by Moermans and Andrew and Kay for correction of metacarpophalangeal joint contractures. Our results are superior in treating proximal interphalangeal joint contractures with 82.1% correction of the contracture
Andrew and Kay [1] reported 46 patients who underwent segmental fasciectomies through small curved incisions. At 1-year follow-up, metacarpophalangeal joint extension improved from 41° to 1.1°, while proximal interphalangeal joint extension improved from 50° to 22°. Their results are similar to those expected from subtotal fasciectomy, with almost complete correction of the metacarpophalangeal joint contracture and correction of about half the flexion contracture at the proximal interphalangeal joints.
Clibbon and Logan [4] examined 67 patients who underwent segmental fasciectomies through small curved incisions for well-localized palmar cords only. At a mean follow-up of 2.5 years, four patients (6%) had developed recurrent metacarpophalangeal joint flexion contractures and seven patients (10%) had developed significant recurrence of proximal interphalangeal joint flexion contractures. In contrast, no patients have developed recurrent contractures in our study to date at the 2-year follow-up.
Because this is a retrospective study, obvious limitations may influence interpretation of the data. Patients may be subject to recall bias in completing questionnaires 2 years after their index procedures. We also acknowledge the small numbers being presented so far. Nevertheless, this study reports the preliminary findings of a single surgeon's experience in an academic center with 2-year follow-up results. The data support our contention that this less-extensive procedure provides good correction of Dupuytren's contracture and satisfactory results 2 years postoperatively.