
Abstract

Introduction
Since vaccination against Haemophilus influenzae serotype b (Hib) was introduced more than two decades ago, the epidemiology of H. influenzae (Hi) disease has changed, with an increase in the proportion of infections caused by other Hi serotypes. Hi disease leads to a number of invasive infections, most frequently meningitis, pneumonia, epiglottitis, and bacteremia without localized infection. Localized soft tissue infections, particularly of the hand, are exceedingly rare. We present the case of a young patient who presented with fever and a left hand abscess secondary to H. influenzae serotype a (Hia) infection.
Case Report
A 13-month-old Caucasian girl presented to a local emergency department with low-grade fever and decreased movement in her left upper extremity a day after falling down a short flight of stairs with no apparent injury. A full physical examination, including of the pharynx and tympanic membranes, revealed no obvious source for the fever. No specific areas of tenderness, swelling, or erythema were noted over the upper extremity. Active and passive ranges of motion were full. Given the history of a fall, radiographs were performed of the left upper extremity; no fracture, dislocation, or soft tissue abnormalities were noted. She was discharged home with supportive care in the form of ibuprofen and acetaminophen.
The patient returned to the local emergency department 4 days later with persistent fever, increased swelling of the left arm and hand, lethargy, anorexia, and decreased urine output. She had no vomiting, diarrhea, or upper respiratory infection symptoms. On examination, she was noted to be febrile (39.7°C), normotensive, and tachycardic (heart rate 182) and tachypneic (respiratory rate 50) despite adequate pain control with intravenous morphine. Tachycardia was responsive to normal saline boluses. Initial white blood cell count was 13.7 (x109/L), with a neutrophil count of 7.81 (x109/L). Radiographs of the left upper extremity revealed soft tissue swelling of the first webspace with no evidence of gas. Peripheral blood cultures were drawn and an initial Gram stain revealed Gram-negative bacilli. Intravenous antibiotic therapy (vancomycin and cefotaxime) was initiated and emergent transfer to a tertiary center undertaken with a putative diagnosis of a severe soft tissue infection and associated septicemia.
Her past medical history was otherwise unremarkable. She was born at term following an uncomplicated pregnancy with no neonatal complications. Her immunizations, including conjugated vaccine against Hib, were up to date. There was no history suggestive of immunodeficiency such as recurrent or severe infections. She was the third of three children. No known infectious human or zoonotic contacts were identified, nor was any recent travel undertaken.
Upon arrival to the tertiary center, the patient was admitted to the general pediatric medicine service, and the plastic surgery, orthopedic surgery, and the infectious diseases services were consulted. The patient's fever was controlled with acetaminophen and vital signs normalized with additional fluid boluses. Antibiotic therapy was broadened with the addition of clindamycin pending speciation of the blood culture drawn earlier. On examination, the patient favored her left arm and was upset with any manipulation of the extremity. Although active elbow movement was good, hand and wrist movement were limited by pain. An area of swelling, erythema, and tenderness was noted over the first webspace. The forearm was soft with no crepitus. Capillary refill to the digits was within normal limits, and the radial and ulnar pulses were palpable. Axillary lymphadenopathy was present. Sensation was preserved. Repeat bloodwork revealed an elevation of the white blood cell count to 20 (x109/L) with an increased band count.
MRI scan of the extremity revealed a collection in the first webspace suggestive of a phlegmon or early abscess (Fig. 1). Patchy signal was noted in the muscles of both the extensor and flexor compartments suggestive of edema. Associated circumferential proximal fluid tracking along the superficial fascia to a moderate reactive elbow effusion was noted.
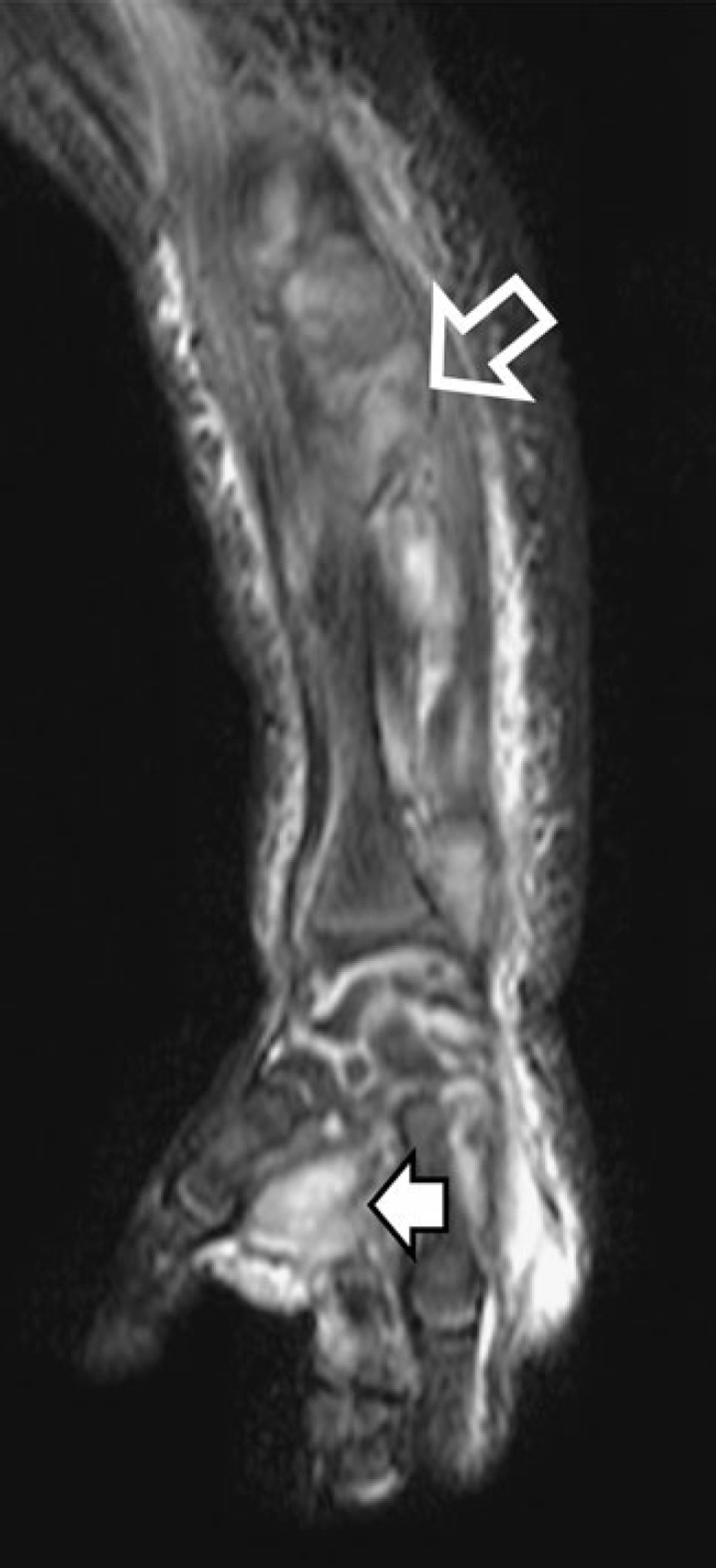
Representative coronal short T1 inversion recovery magnetic resonance image of the left upper extremity. Hyperintense signal suggestive of a phlegmon or abscess is noted in the first webspace (solid arrow). Patchy signal is noted in the extensor compartment of the forearm (hollow arrow) suggesting edema
Despite an initial improvement in the patient's clinical appearance in the first 48 h following transfer to our center, progression of the swelling and erythema in the hand was noted (Fig. 2) with extension into the forearm. Capillary refill was also noted to be brisker. A repeat white blood cell count was 31 (x109/L). The patient was brought to the operating room for an incision and drainage and exploration of the upper extremity 4 days following her initial presentation.

Immediative preoperative photographs of the volar (above) and dorsal (below) aspects of the left upper extremity demonstrating substantial swelling and erythema centered over the first webspace with proximal extension into the forearm
Intraoperative exploration was initiated through a volar incision along the first webspace crease. A deep pocket of pus was encountered and drained. Aerobic and anaerobic cultures were obtained. An intraoperative Gram stain was not performed. The carpal tunnel was released to reveal edema fluid only. The volar deep space was further explored and edema encountered without frank pus in the area adjacent to the abscess deep and radial to the flexor digitorum profundus tendon to index. No collections were noted more proximally in the volar forearm. The wound was extended dorsally to the level of the extensor retinaculum where pus was identified distal and superficial to the extensor retinaculum. The retinaculum was left intact with edema noted in the third and fourth compartments. A substantial amount of edema was palpable at the extensor origin with no overlying erythema, and the intervening segment of soft tissue in the middle third of the forearm was clinically normal. The wound was irrigated with copious amounts of normal saline prior to closure.
Over the subsequent week, clinical improvement with pain, swelling, and erythema was noted daily. Improved finger movement and hand use were noted almost immediately. The incisions continued to heal well with no evidence of additional drainage or recurrence. Final speciation from the blood and wound cultures revealed Hia as the causative agent. The organism was sensitive to ampicillin and the patient's antibiotic therapy was switched to oral amoxicillin/clavulinic acid. Despite a rapid clinical improvement, resolution of the patient's leukocytosis was slow, not reaching normal levels until over a week after surgery. Furthermore, the patient developed a thrombocytosis (maximum platelet count 1,559×109/L) postoperatively that took an additional 2 weeks to resolve. At 3 weeks following surgery, the patient's functional assessment revealed slightly decreased thumb interphalangeal joint flexion relative to the unaffected contralateral side. Despite this, her left upper extremity hand function was within normal limits for her age.
Discussion
H. influenzae is a small Gram-negative rod that was first identified as a pathogen after being isolated from patients with purulent conjunctivitis by Koch [8]. Pittman later identified nonencapsulated strains of Hi as well as six antigenically distinct encapsulated strains that could be identified serologically, now defined as serotypes a to f [12]. She also recognized that serotype b was responsible for almost all cases of Hi meningitis. Population-based studies subsequently confirmed that Hib is responsible for the vast majority of all invasive Hi disease in unvaccinated children [2,18]. The introduction of Hib conjugate vaccines over two decades ago has led to a substantial fall in childhood Hib disease [6].
With the decrease in Hib disease, non-type b Hi has become a more important cause of Hi disease. Serotypes a (Hia) and (Hif) have been reported as the most common cause of invasive encapsulated non-b Hi disease in children [14,17]. In one Brazilian study, Hia meningitis incidence replaced that of Hib meningitis following the introduction of routine childhood immunization [13]. Investigators in Utah reported five invasive Hia cases with a virulence pattern similar to cases caused by Hib [1]. Hia invasive infections have been reported among Native American children in two studies. Millar et al. reported 76 Hia invasive infections cases occurring among Navajo and White Mountain Apache children from 1988 to 2003 [10]. Most infections were due due to meningitis or pneumonia. Although cases of septic arthritis and cellulitis were included, upper extremity involvement or abscess formation was not specified. Hammitt et al. [4] reported an outbreak of five Hia infections which occurred in three Alaskan native infants in two remote villages, one of which suffered a septic left elbow. In a large Canadian study, 25 cases of invasive Hia infection were identified [9]. None had documented upper extremity involvement. Patients with Hia infection were noted to be more likely to have an underlying condition.
In the case presented, no history of underlying illness was identified. Similarly, no preceding upper respiratory tract or otitis media was documented. Despite this, it is likely that our patient's infection resulted from hematogenous spread from oropharyngeal colonization as documented in other cases [4]. Although the history of a fall preceding the patient's illness was likely non-contributory, we cannot rule out the fact that the inflammation secondary to minor trauma predisposed the left upper extremity to hematogenous seeding.
Although cases of pyomyositis secondary to Hib infection have been described [3,5,7,11,15], there are no previous documented cases of Hia soft tissue infection in the hand leading to abscess formation. To this end, Hi infections are rarely encountered in the plastic surgical literature. Although our surgical management of the Hia infection did not differ from that of any other pyogenic pathogen, the postoperative finding of marked thrombocytosis that lagged behind the patient's clinical improvement was in keeping with a Hi infection [16]. This case illustrates that although the widespread use of conjugated vaccines has led to decreased rates of Hib infection, H. influenzae should still be considered as a causative organism in infections of the upper extremity.