
Abstract
Case Report
History
An otherwise healthy 6-year-old African-American male presented to our institution with bilateral flexion deformities of his thumbs. The child had undergone bilateral trigger thumb releases at 1 year of age. The parents noted little to no improvement after surgery, and the thumb deformity seemed to progress. The parents stated that the child had considerable difficulty in voluntarily extending the thumb from the palm, which limited the dexterity and function of the hand.
Physical Examination
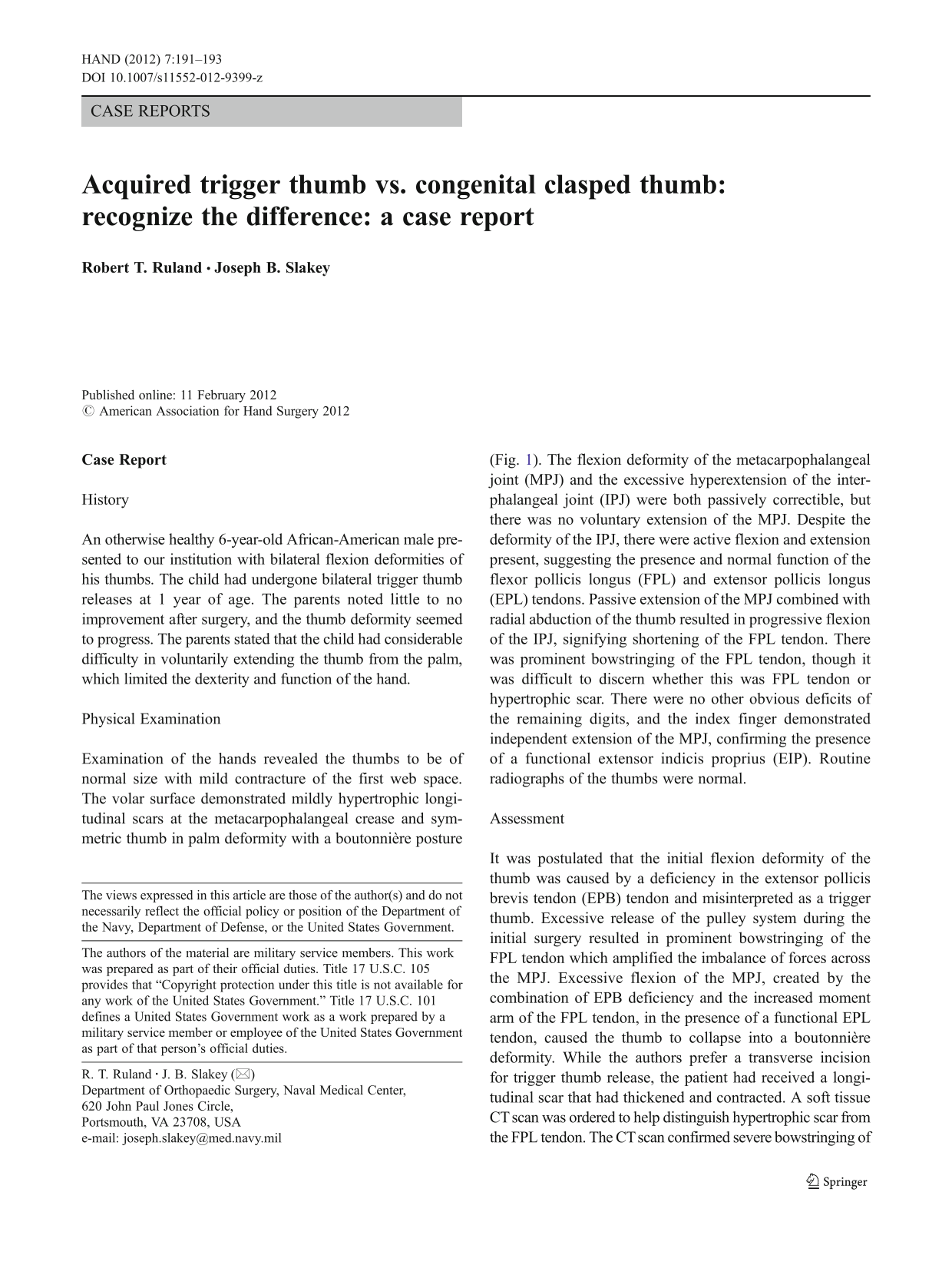
Examination of the hands revealed the thumbs to be of normal size with mild contracture of the first web space. The volar surface demonstrated mildly hypertrophic longitudinal scars at the metacarpophalangeal crease and symmetric thumb in palm deformity with a boutonnière posture (Fig. 1). The flexion deformity of the metacarpophalangeal joint (MPJ) and the excessive hyperextension of the interphalangeal joint (IPJ) were both passively correctible, but there was no voluntary extension of the MPJ. Despite the deformity of the IPJ, there were active flexion and extension present, suggesting the presence and normal function of the flexor pollicis longus (FPL) and extensor pollicis longus (EPL) tendons. Passive extension of the MPJ combined with radial abduction of the thumb resulted in progressive flexion of the IPJ, signifying shortening of the FPL tendon. There was prominent bowstringing of the FPL tendon, though it was difficult to discern whether this was FPL tendon or hypertrophic scar. There were no other obvious deficits of the remaining digits, and the index finger demonstrated independent extension of the MPJ, confirming the presence of a functional extensor indicis proprius (EIP). Routine radiographs of the thumbs were normal.

Thumb in palm deformity with a boutonnière posture
Assessment
It was postulated that the initial flexion deformity of the thumb was caused by a deficiency in the extensor pollicis brevis tendon (EPB) tendon and misinterpreted as a trigger thumb. Excessive release of the pulley system during the initial surgery resulted in prominent bowstringing of the FPL tendon which amplified the imbalance of forces across the MPJ. Excessive flexion of the MPJ, created by the combination of EPB deficiency and the increased moment arm of the FPL tendon, in the presence of a functional EPL tendon, caused the thumb to collapse into a boutonnière deformity. While the authors prefer a transverse incision for trigger thumb release, the patient had received a longitudinal scar that had thickened and contracted. A soft tissue CT scan was ordered to help distinguish hypertrophic scar from the FPL tendon. The CT scan confirmed severe bowstringing of the FPL tendon (Fig. 2). The combination of a congenital thumb in palm deformity and bowstringing of the flexor tendon lead to the progressive shortening of the FPL musculotendinous unit.
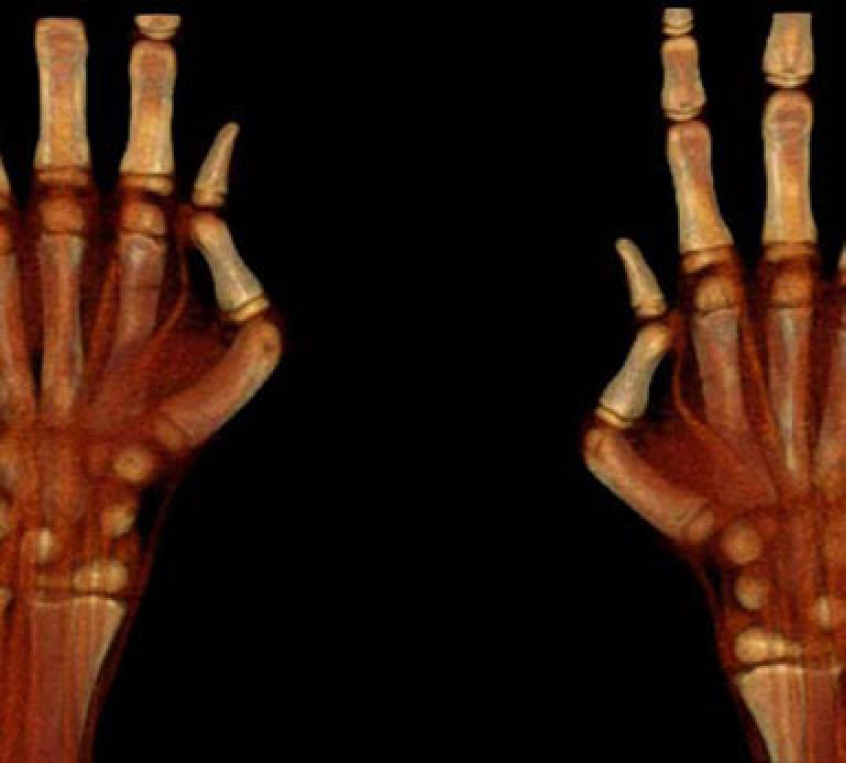
CT scan demonstrating bowstringing of the FPL
Surgical Procedure
A successful surgical procedure needed to address three fundamental problems: (1) EPB deficiency, (2) shortening of the FPL musculotendinous unit, and (3) absence of a functional pulley system. It was postulated that FPL lengthening alone would not result in a permanent correction and that pulley reconstruction was imperative to prevent recurrent bowstringing.
Exploration of the flexor tendon sheath through the previous volar approach to the thumb revealed a dysfunctional pulley system. Fibrous tissue preventing reduction of the tendon was removed extraperiosteally. To maintain the tendon in a reduced position, lengthening of the shortened FPL musculotendinous unit was required. Using a separate incision over the FCR tendon proximal to the wrist crease, the musculotendinous junction of the FPL was exposed and subjected to fractional lengthening. With the thumb in radial abduction and the MPJ in full extension, the FPL tendon now rested against the bone with slight IPJ flexion. (prior to the FPL fractional lengthening, this position resulted in 90° of IPJ flexion.) To maintain corrected thumb position, a K-wire was passed from the tip of the thumb across the MPJ. Through a separate longitudinal incision over the dorsum of the wrist, a 1-cm wide strip of extensor retinaculum from the second to the fifth compartments was harvested and utilized to create a new pulley for the FPL tendon at the level of the MPJ.
After addressing the foreshortened FPL and reconstructing the pulley system, attention was directed toward the EPB deficiency. Through the longitudinal incision over the index MPJ, the EIP was harvested. The tendon was rerouted subcutaneously from proximal to the extensor retinaculum to the insertion site of the EPB at the base of the proximal phalanx of the thumb. A vestigial EPB tendon was identified, though no proximal muscle attachment was seen. The tendon transfer was secured to the vestigial EPB tendon.
All wounds were closed with 5.0 chromic suture. Once dressed, a long arm cast or thumb spica cast, which included the IPJ, was applied, maintaining the first web space. Pin removal occurred 6 weeks later, followed by the application of a hand-based orthoplast thumb spica splint with a web space extension to prevent adduction contracture. The IPJ was kept free for active range of motion. The splint was worn full time for 6 weeks and then continued at night for another 3 months. At 6 months post-surgery, the thumb maintained its new posture (Fig. 3) and had active extension of both the MPJ and IPJ and a weak but functional FPL. The parents were pleased with the result and wished to proceed with correction of the opposite thumb.

Six months post-op
Discussion
Persistent flexion deformity of the pediatric thumb can be acquired or congenital and can be related to abnormalities of either the flexor or extensor mechanism. Pediatric trigger thumb and congenital clasped thumb are overwhelmingly the most common conditions resulting in a flexed posture [2]. An in-depth discussion of other etiologies is beyond the scope of this article.
In the first 3–4 months of life, the infant holds the thumb in the palm with the other digits [10]. Only when the infant begins to incorporate the thumb into grasp does the persistent flexion posture become apparent [3]. Differentiating acquired trigger thumb from congenital clasped thumb is critical, especially if surgical correction is considered.
Several key features help to distinguish these two very different entities. Pediatric trigger thumb, although somewhat controversial, appears to be an acquired condition and is typically unilateral [4,7–9]. The clasped thumb, a congenital deficiency of the extensor mechanism with familial tendency, is much less common than the trigger thumb and is typically bilateral [3].
Both conditions present with persistent flexion deformity of the thumb. In addition to fusiform thickening of the flexor tendon at the level of the MPJ (Notta's node), the trigger thumb has a characteristic flexion of the IPJ that typically cannot be passively extended. Efforts to extend the IPJ may cause pain or a palpable click, as the nodular tendon is pulled distal to the pulley. The authors believe that Notta's node is almost universally present in a typical pediatric trigger thumb. The supple clasped thumb's characteristic flexion deformity is at the MPJ and is passively correctible, but cannot be voluntarily extended [6]. If there is EPL deficiency, in addition to the absence of the EPB, then a flexion deformity can occur at the IPJ also, but it is still passively correctible. Recognizing these fundamental differences is critical, if a splinting regimen is unsuccessful [1,5] and surgery is considered. A trigger thumb release, in the presence of EPB deficiency, may accentuate the MPJ flexion deformity in an already unbalanced digit. Excessive release of the pulley system, which effectively increases the moment arm of the FPL, in the presence of an intact EPL, can lead to a boutonnière posture.
A proper history and thorough clinical examination will help differentiate the etiology of a persistent flexion deformity of the pediatric thumb. The authors offer a surgical solution for a difficult reconstructive problem that may have been avoided, if properly identified.