
Abstract
Introduction
The Moberg neurovascular advancement flap, first described in 1964, has proven to be ideal for soft tissue defects of the thumb pulp measuring ≤1.5 cm in size [8]. For such small defects, this technique provides sufficient skin coverage allowing preservation of length and most importantly good restoration of sensation and function [2,5]. Modifications to the Moberg flap have allowed coverage of deficits >1.5 cm but have been hampered by the residual defect located at the donor site. In 1968, O'Brien proposed the use of a split thickness skin graft to cover the donor deficit [9]. The disadvantages of a skin graft such as immobilization, risk of graft failure, and contracture render this technique less attractive. Others have avoided grafting with V–Y modifications to the Moberg flap [1,3,4,10]. However, tension at the donor site often occurs and may result in incomplete closure or in skin necrosis. In these instances, splinting in the flexed position to decrease tension or dressing changes to encourage epithelialization when complete primary closure is not feasible is required [4,7]. As a consequence, scar hypertrophy, contractures, joint stiffness, and delayed mobilization may prolong return to function. Dellon demonstrated that defects of up to 3 cm could be resurfaced using an extended palmar flap with dissection into the thenar eminence [3]. Two rotational flaps are used to close the donor deficit. Although providing good closure, this technique requires extensive dissection and is technically difficult.
We present a new modification of the Moberg–O'Brien technique that utilizes the skin of the first web space to fill the proximal defect caused by the mobilization of the flap. This simple technique provides tension-free closure and avoids the need for immobilization or dressing changes. Excellent esthetics and function is achieved by deepening the first web space with a Z-plasty and hence increasing the relative length of the thumb.
Operative Technique
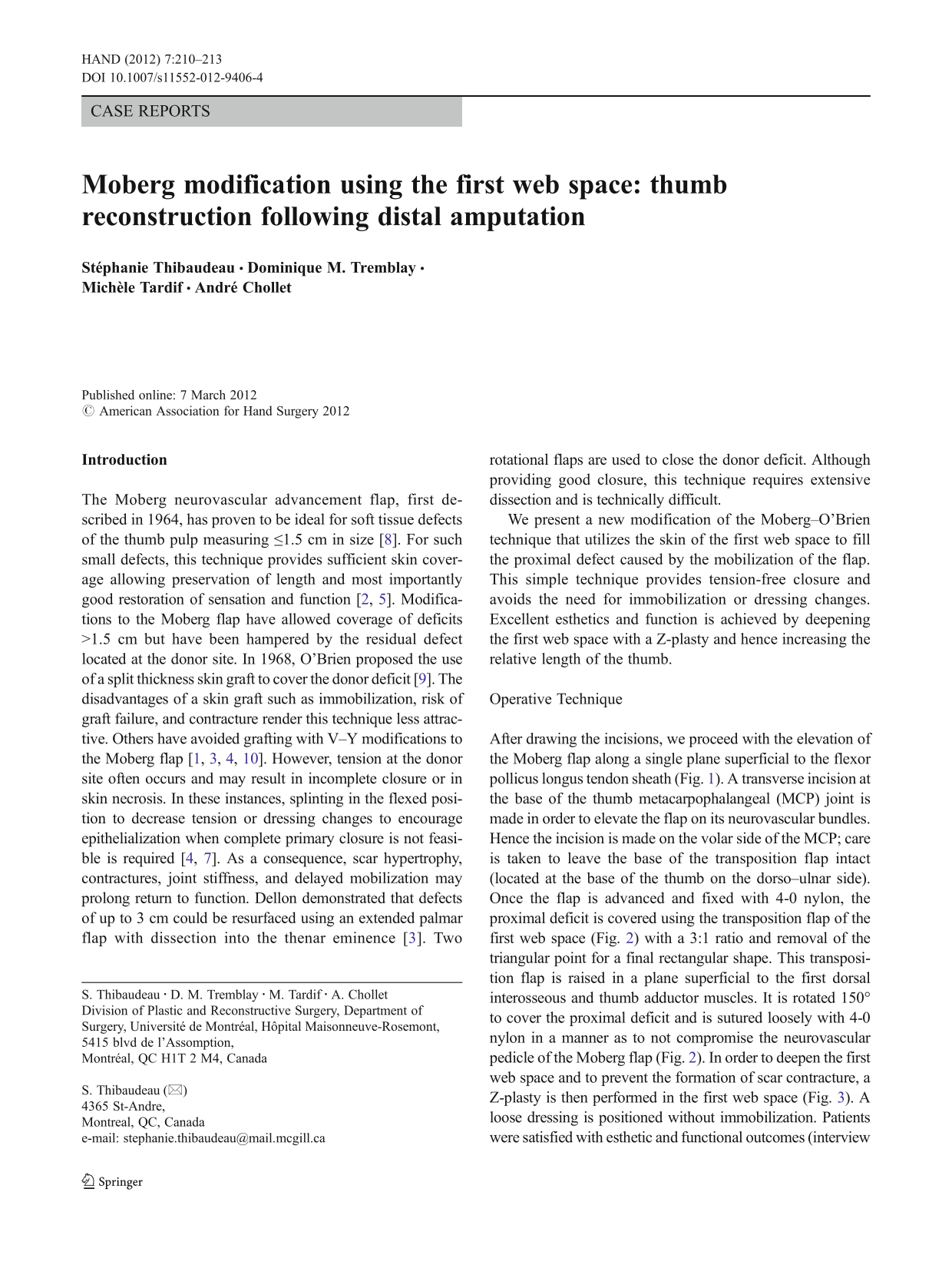
After drawing the incisions, we proceed with the elevation of the Moberg flap along a single plane superficial to the flexor pollicus longus tendon sheath (Fig. 1). A transverse incision at the base of the thumb metacarpophalangeal (MCP) joint is made in order to elevate the flap on its neurovascular bundles. Hence the incision is made on the volar side of the MCP; care is taken to leave the base of the transposition flap intact (located at the base of the thumb on the dorso–ulnar side). Once the flap is advanced and fixed with 4-0 nylon, the proximal deficit is covered using the transposition flap of the first web space (Fig. 2) with a 3:1 ratio and removal of the triangular point for a final rectangular shape. This transposition flap is raised in a plane superficial to the first dorsal interosseous and thumb adductor muscles. It is rotated 150° to cover the proximal deficit and is sutured loosely with 4-0 nylon in a manner as to not compromise the neurovascular pedicle of the Moberg flap (Fig. 2). In order to deepen the first web space and to prevent the formation of scar contracture, a Z-plasty is then performed in the first web space (Fig. 3). A loose dressing is positioned without immobilization. Patients were satisfied with esthetic and functional outcomes (interview and at follow-up visit). For the purpose of this paper, we present the readers with three cases.

Case 1—operative technique: Moberg-O'Brien flap. Two mid-axial incisions dorsal to the neurovascular bundle and one transverse incision at the base of the first metacarpal are drawn according to the Moberg–O'Brien flap. The transverse incision must not cross the base of the transposition flap, which is based on the dorso–ulnar aspect of the side of the thumb and extending across the first web space. The tracings for the Z-plasty of the first web space are completed. The flap is elevated along a single plane superficial to the flexor pollicis longus tendon sheath
Case 1—operative technique: transposition flap

Case 1—operative technique: Z-plasty
Case Report
Case 1
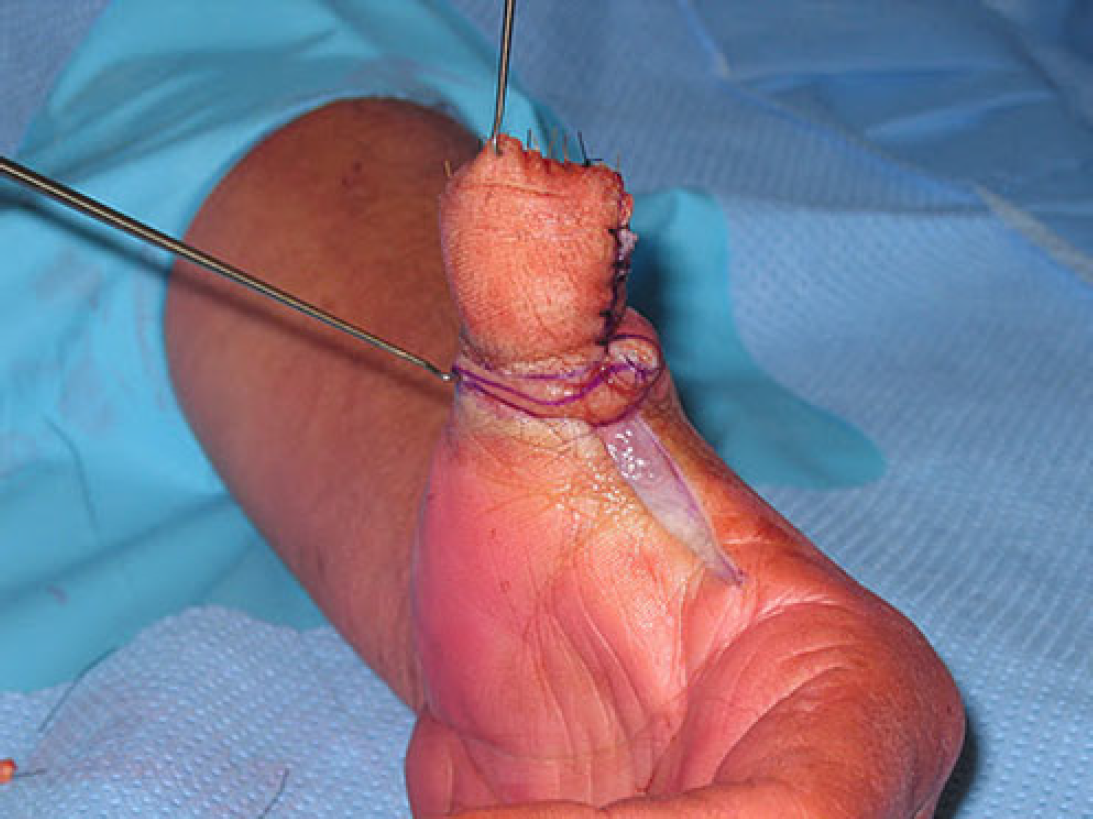
A 61-year-old man had a work-related accidental guillotine amputation of his left thumb at the level of the interphalangeal joint. The patient was a right-handed smoker with an unremarkable past medical history. The patient's operation was uneventful and postoperative immobilization was not required (Fig. 4). At his five day postoperative follow-up, the patient had no complaints and was already demonstrating good mobilization (Fig. 5). The patient was absent for his 2-week follow-up, as he had returned to work. At his 6-month follow-up, the patient reports normal sensation in his left thumb and is satisfied with the esthetics outcome of his operation (Fig. 6). His range of motion (ROM) was satisfactory as well as his grip and pinch strength (Tables 1 and 2).

Case 1—immediate postoperative result

Case 1—5 days postoperative follow-up

Case 1—6 months operative follow-up. The relative length of the left thumb to the others fingers is esthetically pleasing and the patient reported that lay people rarely notice his amputation
Assessment of functional postoperative (6-month) outcome
Dominant hand is in bold and injured hand in italics
Normal 2 PD (point discrimination) is defined as ≤6 mm
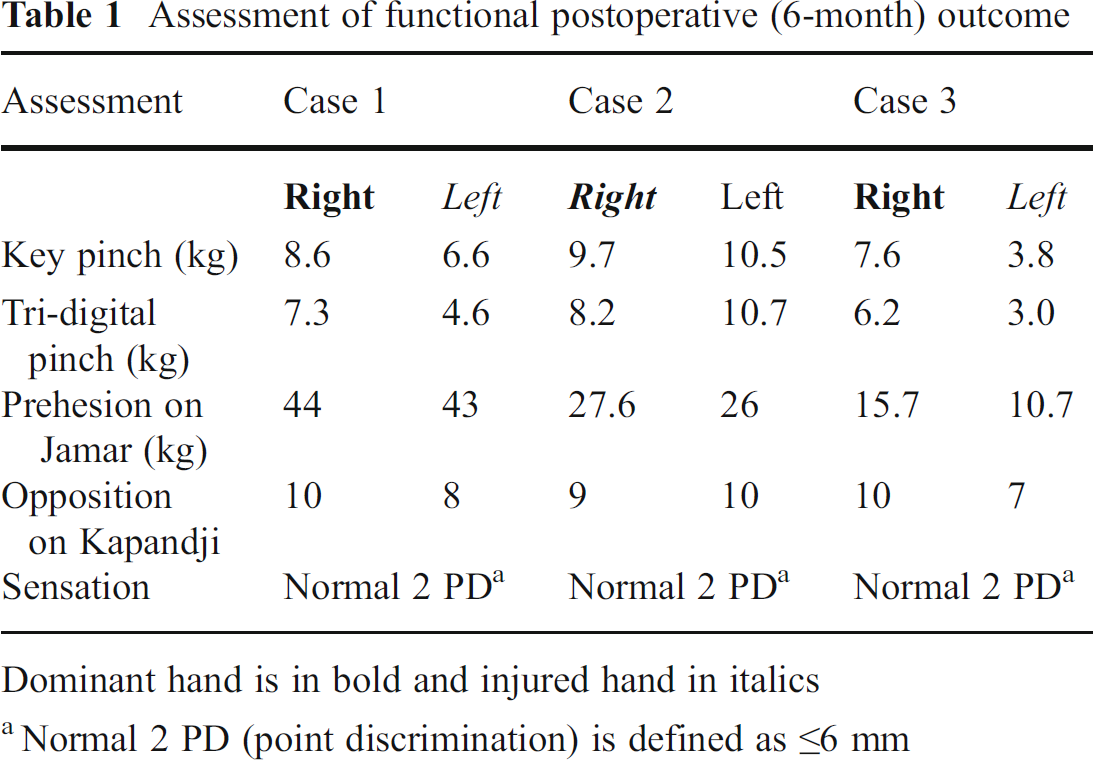
Postoperative range of motion at the thumb metacarpophalangeal joint
Dominant hand is in bold and injured hand in italics
Case 2
A 72-year-old retired man had guillotine amputation of right thumb at the interphalangeal joint. The patient is a right-handed nonsmoker with a history of arterial hypertension. We performed the above-described surgical technique. Secondary to significant edema, complete primary closure was not possible and we left a 1.5-cm square area for granulation. One week postoperatively, the patient had no complaints. No postoperative splinting was used but the dressings slightly restricted his range of motion. The patient was encouraged to resume light activities of daily living and was to progress his level of activity according to his pain threshold. At his 1-month postoperative follow-up, the patient had resumed his regular activities and his ROM and strength was satisfactory (Fig. 7; Tables 1 and 2). Healing at the transposition flap and first web space was excellent.

Case 2—1-month postoperative follow-up. Range of motion exercises: satisfactory abduction and opposition
Case 3
A 70-year-old retired worker who suffered an accidental guillotine amputation of his left thumb at the interphalangeal joint. He underwent a Moberg flap with our modification. He is a right-hand dominant smoker with several comorbidities including arteriosclerosis, sarcoma of right hip, and hypertension. His postoperative follow-up was uneventful. He describes being satisfied with the esthetic result; however, he presents with hypersensibility of his thumb stump. He declined desensitization therapy with our occupational therapist mainly due to his limited mobility secondary to his sarcoma of the right hip currently in remission. Due to his weakened health status he no longer does manual work and could not comment on his level of function with manual work (Tables 1 and 2 for the results of ROM and strength).
Discussion
The Moberg flap and its described modifications including burrow triangles, local rotation flaps, V–Y closure, and skin grafts for donor deficits provide good soft tissue coverage with innervated and well-vascularized tissue [3,4,9,10]. These techniques restore sensation, provide good long-term functional outcome and result in patient satisfaction [2,5]. In the study by Baumeister et al., all deficits smaller than 2 cm were successfully treated and no flaps were lost [2]. Modifications to the Moberg flap had similar outcomes compared with the original technique. Hence, for deficits of 1.5 to 2 cm in size, the Moberg flap and its modifications are excellent choices for amputations of the distal thumb.
We present a new modification that is simple and has the advantage of limiting tension upon closure as well as excellent esthetic appearance. The skin of the first web space provides a sufficient amount of well-vascularized tissue that can be tailored as a transposition flap to the size of the donor defect. This local transposition flap provides tension-free closure and avoids the need for skin grafting, dressing changes, or postoperative immobilization which reduces the likelihood of contractures. Unlike the extended palmar advancement flap, this technique avoids extensive dissection into the thenar eminence. This Moberg modification is time effective and allows for rapid postoperative mobilization. In our field of practice where the majority of our patient's injuries are secondary to work accidents, this modification is advantageous for the patient, hand therapists, employer, and surgeon.
This technique is also esthetically acceptable as the skin laxity prevents narrowing at the base of the thumb which is often seen with V-Y closure. The use of Z-plasty to eliminate first web space contractures is well known. Fraulin and Thomson have shown that four-flap Z-plasty with 120° angles are best to deepen the first web space [6]. We found that a one standard Z-plasty is sufficient to deepen the first web space and concomitantly close our donor deficit site. A four-flap Z-plasty could also have been used. This provides the patients with increased relative length of the thumb compared to the other digits of the hand. Finally, the remaining scars are minimal and are partly hidden in the first web space and palmar creases of the thumb resulting in high patient satisfaction.
This study is limited by the small number of cases. Our future intention is to acquire a greater case series, in which we present more objectified measurements of functional outcome in the immediate and long-term follow-up.
In conclusion, we believe that this newly described modification improves patient functional outcome by avoiding skin grafting and allowing rapid mobilization. We would recommend this technique for distal thumb tip amputations measuring less than 2 cm.