
Abstract
Background
Symptoms and psychosocial factors are suggested to account for more of the variation in disability than physical impairment, but perhaps less so at the level of specific tasks. This study assessed the influence of impaired wrist motion on specific tasks on the Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire.
Methods
Sixty-three patients with an operatively treated fracture of the distal radius completed the Pain Catastrophizing Scale (PCS), Pain Anxiety Symptoms Scale, and Center for Epidemiologic Studies Depression Scale (CES-D) just before surgery and the DASH questionnaire 3 months after surgery. Nine questions on the DASH were selected as potentially sensitive to changes in wrist motion and evaluated in bivariate and multivariable analyses.
Results
In multivariable models of factors associated with specific tasks, only “Open a tight or new jar” was affected by wrist flexion and PCS accounting for 33 % of the variation. Motion, pain, and PCS were significant predictors of the DASH score. Among the eight tasks not related to wrist motion, 33 % of the variation in disability with writing was accounted for by PCS and limb dominance; 20 % of disability preparing a meal by pain, CES-D, and PCS; 14 % of disability with making a bed by pain and CES-D; and 23 % of changing a light bulb overhead by age, pain, and fracture type.
Conclusions
After volar plate fixation of a fracture of the distal radius, upper extremity disability based on select items from the DASH questionnaire correlated minimally with impairment of wrist motion, even at the level of specific tasks. Level of Evidence Prognostic Level II.
Introduction
Symptoms (pain in particular), psychological factors (e.g., catastrophic thinking, kinesiophobia which is fear of movement [12], and symptoms of anxiety and depression), and sociological factors (e.g., compensation) account for more of the variation in arm-specific disability than physical impairment [2,3,8,9,17,18]. But one study of patients with impairment after elbow injury found that the influence of impaired motion was more substantial at the level of specific tasks [8].
The aim of this study was to test the null hypothesis that there is no association between loss of wrist flexion and extension and variation in difficulties with specific tasks measured by the Disabilities of the Arm, Shoulder, and Hand (DASH) when accounting for other demographic, personal, and injury factors. Secondary study questions addressed the influence of forearm rotation and the influence of psychological factors.
Materials and Methods
Study Design
For this study, we used the 3-month postoperative data from adult patients with an unstable fracture of the distal radius treated with a locking volar plate within 4 weeks of injury in an Institutional Review Board (IRB)-approved clinical trial designed for another purpose [14]. All patients signed an informed consent to participate in the clinical trial. The IRB approved our secondary use of this data.
The inclusion criteria for the current study were: attendance at the 3-month follow-up visit with a valid DASH questionnaire and no injury of the contralateral wrist. Among the 67 patients with a 3-month postoperative evaluation, one had an invalid DASH score and three patients had an injury to the contralateral side. These four patients were excluded, leaving 63 patients in our study cohort.
Patient Characteristics
There were 45 women (71%) and 18 men (29%), with a mean age of 52 (range, 23 to 81 years). There were 16 Arbeitsgemeinschaft für Osteosynthesefragen (AO) type A distal radius fractures (25 %), 6 type B (10 %), and 41 type C (65 %) [4]. The dominant wrist was affected in 29 patients (46 %) (Table 1).
Patient demographics, n=63
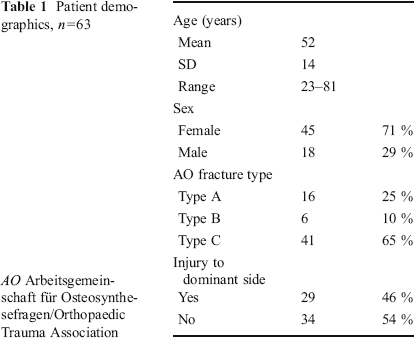
AO Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association
Evaluation
At enrollment prior to surgery, patients completed the Pain Catastrophizing Scale (PCS), Center for Epidemiologic Studies Depression Scale (CES-D), and Pain Anxiety Symptoms Scale (PASS) questionnaires [10,13,15]. The PCS was used to measure catastrophic thinking in response to nociception [15]. A higher score indicates a greater tendency to think the worst [15]. Symptoms of depression were measured using the CES-D questionnaire [13]. This questionnaire consists of 20 questions and a higher score indicates more symptoms of depression [13]. The patients completed the PASS questionnaire to evaluate anxiety associated with pain [10]. This questionnaire consists of four dimensions: fear of pain, cognitive anxiety, somatic anxiety, and escape and avoidance [10,19]. Each dimension score ranges from 0 to 50 and the total PASS score ranges from 0 to 200 points, where a higher score indicates greater pain anxiety [10,19]. One patient had a missing PASS score so we imputed the mean of the group for this missing value.
Three months after surgery, patients completed a questionnaire to measure arm-specific disability, the DASH [5]. This questionnaire consists of 30 questions on a five-point Likert scale [5]. The total score ranges from 0 to 100 points; a higher score indicates greater disability [5].
For this study, we selected nine specific questions we thought might be most affected by a loss of wrist flexion and extension: (1) “Open a tight or new jar,” (2) “Write,” (3) “Prepare a meal,” (4) “Make a bed,” (5) “Change a light bulb overhead,” (6) “Wash or blow dry your hair,” (7) “Wash your back,” (8) “Put on a pullover sweater,” and (9) “Use a knife to cut food” [5]. There were 25 unanswered questions in 13 different patients. Two patients had one missing wrist function-specific task question, and one patient had two missing wrist function-specific questions. We used mean imputation for unanswered questions.
Pain at 3 months was assessed with an ordinal pain scale ranging from 0 representing no pain to 10 representing the worst pain the patient ever had. Four patients did not complete the pain score, so we used mean imputation for those missing values.
Range of motion was assessed at the 3-month follow-up for wrist flexion, wrist extension, pronation, and supination. Motion as the percentage of the unaffected side was calculated.
Statistical Evaluation
A post hoc power analysis on our sample of convenience of 63 patients indicated that a sample size of 63 patients, with an R2 of 0.20 (effect size of 0.25), and α=0.05, an F test with six predictors would yield 82 % power.
The Kolmogorov–Smirnov and Shapiro–Wilk test indicated that only a percentage of injured wrist flexion and percentage of injured wrist extension were normally distributed; the questionnaires were not. Therefore, we chose to use nonparametric tests.
In bivariate analysis, the association between the DASH score and the specific questions from the DASH “Open a tight or new jar,” “Write,” “Prepare a meal,” “Makeabed,” “Change a light bulb overhead,” “Wash or blow dry your hair,” “Wash your back,” “Put on a pullover sweater,” and “Use a knife to cut food” with the continuous independent explanatory variables (age, days injury to surgery, pain, the CES-D, PCS, PASS, and wrist motion) was analyzed using Spearman correlation coefficients. The association between the DASH and the nine specific questions of interest in the DASH with dichotomous independent variables (sex, mobilization (occupational therapy or home exercises), and dominant wrist injured) was analyzed by executing a Mann–Whitney U test. The association of AO fracture type with the DASH and the nine specific questions was analyzed using a Kruskal-Wallis test.
Variables with p<0.10 in the bivariate analysis were inserted in multivariable analysis. Backward stepwise linear regression was used to identify the factors that best account for the variability of the specific questions on the DASH questionnaire.
Results
At enrollment, the median CES-D score was 14 (interquartile range 11), median PCS score was 5 (interquartile range 9), and median PASS score was 59 (interquartile range 46). Three months after surgery, the median DASH score was 9.5 (interquartile range 13) and the median pain score was 1 (interquartile range 1). The mean flexion as a percentage of the uninjured wrist was 74 % (standard deviation 16, range 33–108 %), and mean extension was 85 % (standard deviation 15, range 55–116 %). There were 11 patients with incomplete forearm rotation (Table 2).
Evaluation of results, n63
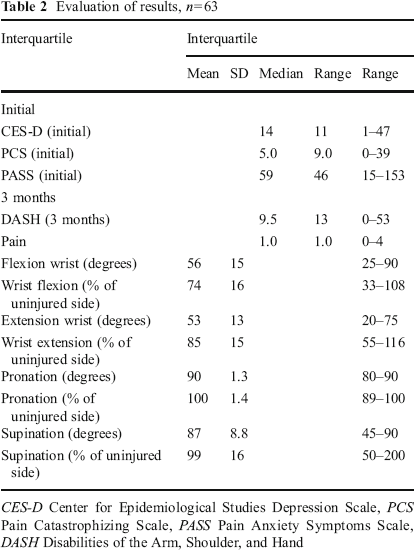
CES-D Center for Epidemiological Studies Depression Scale, PCS Pain Catastrophizing Scale, PASS Pain Anxiety Symptoms Scale, DASH Disabilities of the Arm, Shoulder, and Hand
Total DASH Score
Bivariate analysis showed a significant association between DASH and pain, CES-D, PASS, wrist flexion, and wrist extension (Table 3). In addition, PCS satisfied the criterion for entry in the multivariable analysis. The best model for total DASH score contained pain, PCS, and wrist flexion and accounted for 39 % of the variation in the DASH score (Table 4). The best model without pain included PCS, CES-D, and wrist flexion (adjusted R2 0.27).
Bivariate Statistical analysis
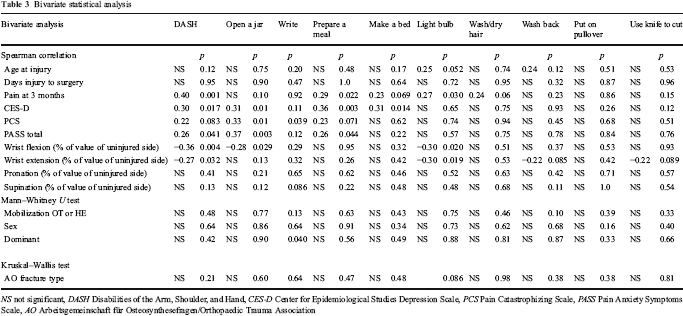
NS not significant, DASH Disabilities of the Arm, Shoulder, and Hand, CES-D Center for Epidemiological Studies Depression Scale, PCS Pain Catastrophizing Scale, PASS Pain Anxiety Symptoms Scale, AO Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association
Multivariable Statistical analysis
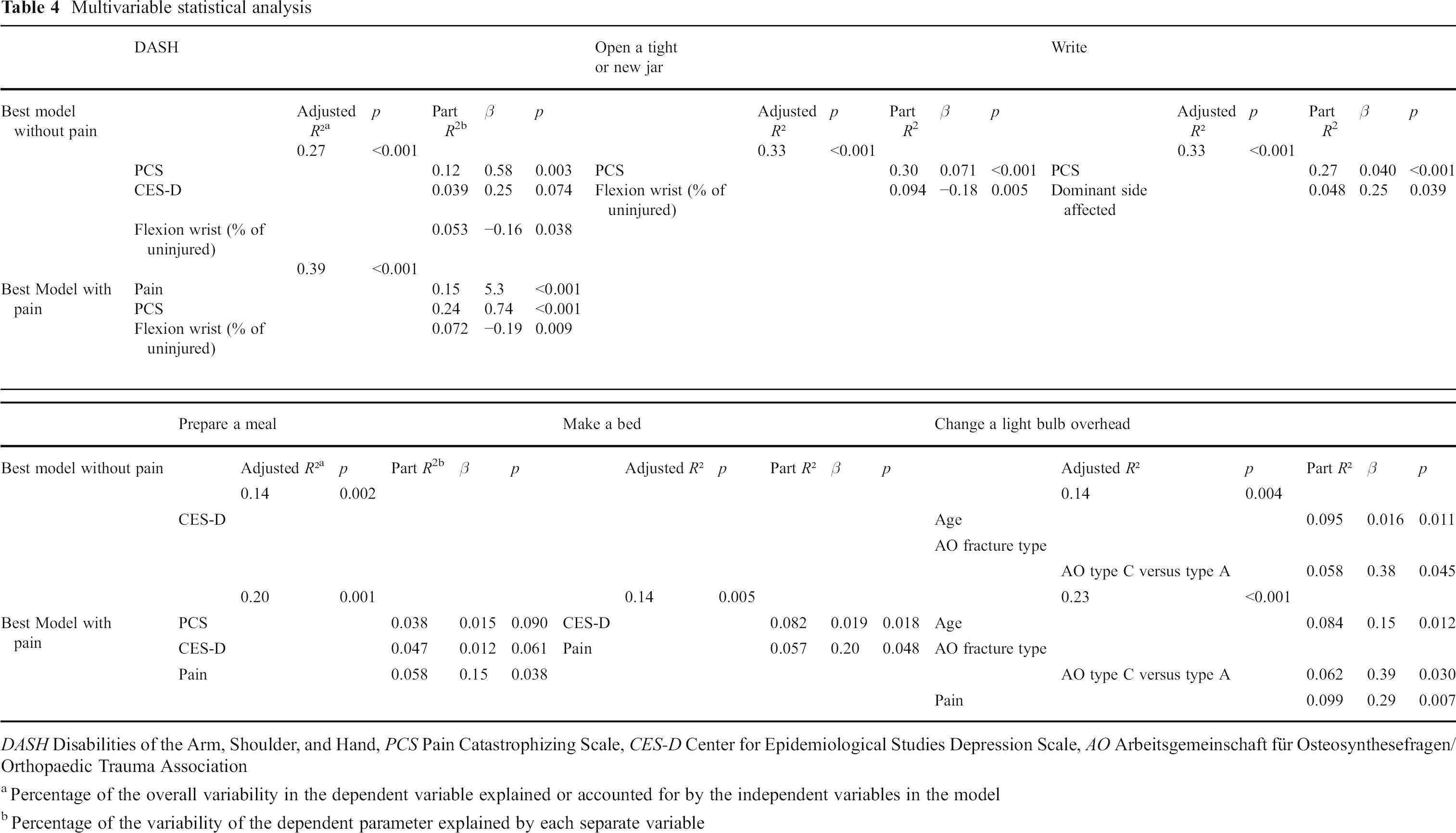
DASH Disabilities of the Arm, Shoulder, and Hand, PCS Pain Catastrophizing Scale, CES-D Center for Epidemiological Studies Depression Scale, AO Arbeitsgemeinschaft für Osteosynthesefragen/Orthopaedic Trauma Association
Percentage of the overall variability in the dependent variable explained or accounted for by the independent variables in the model
Percentage of the variability of the dependent parameter explained by each separate variable
Specific DASH Questions
The correlations of the specific DASH questions with the explanatory variables are presented in Table 3. Forearm rotation did not correlate with any tasks. “Open a tight or new jar” was the only specific question for which impaired wrist motion remained in the best multivariable model, which included PCS and wrist flexion (Table 4). It is notable that a model with wrist flexion alone was not significant (adjusted R2 0.03, p=0.093).
The best models for the other tasks were as follows: PCS and dominant side affected for “Write”; CES-D, PCS, and pain for “Prepare a meal”; CES-D and pain for “Make a bed”; and pain, age, and differences in AO fracture type (type A versus type C) for “Change a light bulb overhead.” There were no significant predictors of “Wash or blow dry your hair,” “Wash your back,” “Use a knife to cut food,” or “Put on a pullover sweater” (Table 3).
Discussion
Variations in difficulty with “Open a tight or new jar,” “Write,” “Prepare a meal,” “Make a bed,” and “Change a light bulb overhead” were best explained by symptoms and psychological factors, but even the best models could explain no more than a third of the variation in difficulty with specific tasks on the DASH. “Open a tight or new jar” was the only specific question for which impaired wrist motion remained in the best multivariable model, but the contribution of impaired wrist motion to the model was relatively small. This contrasts with the findings of Lindenhovius and colleagues that loss of elbow motion determined relatively more of the variability in some task-specific disability than pain compared to the total DASH score [8].
This study should be interpreted in light of several factors. There may be a ceiling effect given that flexion and extension averaged 74 and 85 % of the uninjured side, the mean forearm rotation was near 100 % with only 11 patients having impaired forearm rotation, and the average DASH score (13.5) was not much higher than the mean of the general population (10.1) [6]. Also, the specific questions on the DASH may not reflect the tasks that are most affected by impairment of wrist flexion.
Other shortcomings include the fact that this was a secondary use of data and the original study was designed for a different endpoint [14]; we did mean imputation for missing questions and four patients did not complete the pain score (6 %); and because we imputed the group mean for pain, this might have influenced the importance of pain in our analysis.
In contrast to a prior evaluation of disability related to impairment of elbow motion, we did not find a greater influence of impaired wrist motion at the level of specific tasks. This might reflect a greater influence of elbow stiffness on disability than wrist stiffness or it could be related to a ceiling effect as it has been determined that a greater impairment of wrist motion is needed to affect daily tasks [1,7,11,16,20]. Nevertheless, at least in the setting of recovery from a fracture of the distal radius repaired with a volar plate, although motion was a significant predictor of disability, symptoms and psychological factors explained more of the variation in disability than objective impairment, although most of the variation in disability and difficulty with specific tasks rated by the DASH remains unexplained. Given that this finding is remarkably consistent, the role of cognitive and behavioral therapies in recovery from upper extremity illness and injury merits greater study.
Footnotes
The authors declare that they have no conflict of interest related to this study.