
Abstract
Introduction
Twenty-five patients (19 males and six females) were included in the study based on: chronic symptoms of distal radioulnar joint instability, demonstrable instability on examination, MRI evidence of radioulnar ligament deficiency, and arthroscopic findings of foveal disruption of the radioulnar ligament.
Materials and Methods
Exclusion criteria were: distal radius malunion, congenital malformation of the sigmoid notch, DRUJ arthritis, and less than 24 months minimum follow-up. Mean age was 35 years old with a mean interval from injury to surgery of 5 months. Surgery began with arthroscopic confirmation of the chronic foveal detachment followed by open reconstruction of the radioulnar ligament using the palmaris longus tendon. The specific method employed three drill tunnels corresponding to the true anatomic points of attachment of the radioulnar ligament. Patients were examined post-operatively at 2 weeks, 4 weeks, 6 weeks, 12 weeks, and 6 months.
Results and Discussion
Final evaluation averaged 51 (±14) months following surgery. Measures obtained before and after treatment included: wrist range of motion, forearm range of motion, grip strength, examination findings of distal radioulnar joint instability, and Disabilities of Arm, Shoulder, and Hand (DASH) scores. Pre-operative and postoperative measures were compared using the paired Student's t test, accepting a p value of 0.05 as statistically significant. All patients healed the reconstruction without major complications and demonstrated distal radioulnar joint stability at the 6-week examination. Mean ranges of motion, in degrees, pre-/post-operative were: wrist flexion 53 (±13)/61 (±10), wrist extension 53 (±13)/62 (±15), supination 65 (±12)/74 (±7), and pronation 66 (±11)/71 (±8). Grip strengths expressed as % contralateral pre-/post-operative were: 57 (±23)/79 (±25). The differences in these measures were not found to be statistically significant. The mean pre-/post-operative DASH scores were: 62 (±16)/7 (±3). This difference was found to be statistically significant.
Conclusion
Reconstruction of the RUL with a free palmaris longus tendon graft using the truly anatomic points of original RUL attachment at both the ulna and radius restored DRUJ stability and improved DASH scores without limiting forearm or wrist motion.
Introduction
Patients may present with distal radioulnar joint (DRUJ) instability in an acute, sub-acute, or chronic time sequence relative to the initial injury. This report only addresses patients presenting with chronic DRUJ instability. Instability should be distinguished from laxity [8]. Laxity refers to the demonstration of increased amplitude when performing a ligament integrity test on physical examination and may be physiologically normal. Instability refers to the pathological state of symptomatic joint dysfunction due to the abnormal loss of ligament constraint to the joint. Although multiple anatomic structures contribute to stability of the DRUJ, the primary stabilizer is the radioulnar ligament (RUL) [3,5,10,13,17,20]. The RUL originates from the fovea of the distal ulna, arising through vertically oriented Sharpey's fibers that blend with the inferior borders of the fibrocartilage disk and contribute to the integrated structure referred to as the triangular fibrocartilage complex (TFCC) [12]. Despite the blending of tissue planes that occurs in the TFCC, the volar and dorsal limbs of the RUL are distinct anatomic structures that can be tracked all the way from the fovea to their insertions at the volar and dorsal margins of the sigmoid notch [21].
Previously described reconstructions of the RUL include a free tendon graft passing through a drill tunnel that exits the anatomic point of origin at the ulnar fovea [1,8,19]. In these previous reconstructions, it has been the radial attachments of the free tendon graft that have not replicated the normal anatomy of the RUL. These prior reconstructions have utilized a single sagittal plane drill tunnel proximal to the lunate fossa and radial to the sigmoid notch for radial-sided attachment of the graft. Biomechanical testing of this routing showed that DRUJ stability is not fully restored [4]. Clinical assessment of this routing also showed that stability is not optimally restored and further efforts to more closely replicate the normal anatomy of the radioulnar ligament were warranted [7]. With the prior procedures, one can manually test DRUJ mechanics intra-operatively and see that stability is not fully restored, commensurate with the laboratory data [4]. Careful stability testing post-operatively, once the graft has fully healed, produces the same incomplete result. Depending on the degree of scar tissue formation, some of these patients also exhibited decreased forearm pronation and supination.
Review of the detailed anatomy of the RUL led to the current reconstructive method [5,12,21]. The same radial-sided RUL attachments used in the current clinical reconstruction were subjected to cadaveric testing, evaluating the restoration of stability in neutral, supination, and pronation as well as any effect upon limiting pronation and supination [11]. Reattaching the RUL through intra-articularly created coronal drill tunnels in the radius fully restored DRUJ stability in all three positions of forearm rotation and did so without limiting pronation or supination [11].
Hypothesis Reconstruction of the RUL with a free palmaris longus tendon graft using the truly anatomic points of original RUL attachment at both the ulna and radius will restore DRUJ stability and improve DASH scores without limiting forearm or wrist motion.
Methods and Materials
Thirty-two patients were retrospectively identified by CPT code search of the practice research database as having undergone free tendon graft reconstruction of the radioulnar ligament. Inclusion criteria were: chronic symptoms of DRUJ instability, demonstrable instability on examination, MRI evidence of RUL deficiency, and arthroscopic findings of foveal disruption of the radioulnar ligament. Exclusion criteria were: distal radius malunion, congenital malformation of the sigmoid notch, DRUJ arthritis, and less than 24 months minimum follow-up. On this basis, seven patients were excluded, leaving 25 patients (19 males and six females) with an average age of 35 years for review. Patients were initially treated with therapy, non-steroidal anti-inflammatory agents, intra-articular corticosteroid injection, ergonomic activity modification, and dynamic stabilization therapy exercises (Fig. 1). Some patients treated in the practice were sufficiently palliated by these methods that they did not feel the need for surgery, but these patients were not captured by our search methods and are not counted in this report. The remaining patients of this study ultimately elected surgery at an average of 5 months from initial injury. Surgery began with arthroscopic confirmation of the chronic foveal detachment followed by open reconstruction of the RUL using the palmaris longus tendon. The specific method employed three drill tunnels corresponding to the true anatomic points of attachment of the RUL. According to practice research protocol, all patients undergoing surgery for any diagnosis complete a Disabilities of the Arm, Shoulder, and Hand (DASH) questionnaire pre-operatively. Additional pre-operative measures obtained for the DRUJ specifically included: wrist range of motion, forearm range of motion, grip strength, examination findings of DRUJ instability, and MRI demonstration of RUL deficiency. Post-operatively, patients were examined at 2 weeks, 4 weeks, 6 weeks, 12 weeks, and 6 months. Post-operative measures obtained included: wrist range of motion, forearm range of motion, grip strength, and examination findings of DRUJ instability. Final evaluation was by DASH scores at a mean of 51 (±14) months following surgery. Not obtained post-operatively for comparison to pre-operative findings were: MRI demonstration of RUL integrity and arthroscopic demonstration of RUL integrity. Pre-operative and post-operative measures were compared using the paired Student's t test, accepting a p value of 0.05 as statistically significant.
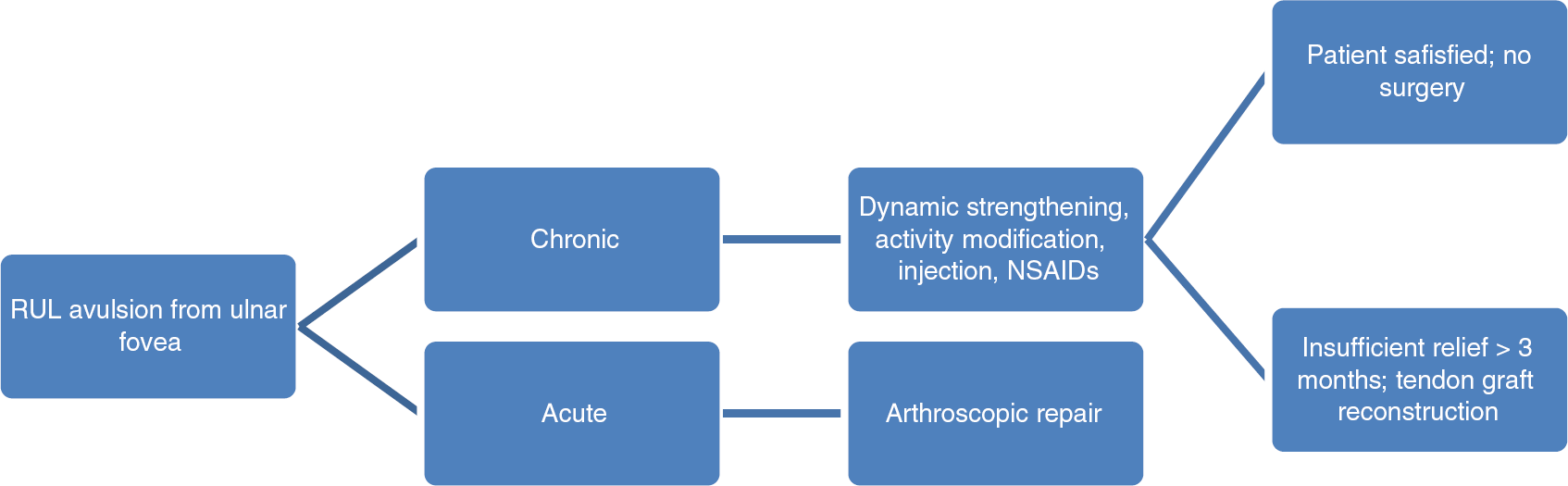
Flowchart for the management of RUL avulsion from the ulnar fovea
Method of Physical Examination for RUL Integrity
To improve accuracy in the context of physiologically normal laxity (as opposed to pathologic instability), all assessments are made by comparing the symptomatic, traumatized side to the contralateral, asymptomatic side that is assumed to represent a normal internal control and reference standard for that particular patient. The patient sits relaxed at a table across from the examiner and places both elbows on the table with the hands pointing to the ceiling. The two sides are then sequentially tested back and forth, multiple times, to arrive at an accurate comparison. The examiner stabilizes the ulna with one hand between thumb and fingertips (left hand of examiner to right hand of patient and vice versa) and then grasps the radial metaphysis with the other (Fig. 2). While keeping the ulna stable as a reference, the DRUJ is loaded, slightly compressing radius to ulna, to enhance the feel of the joint surfaces moving relative to each other. The radius is then translated dorsally and volarly relative to the fixed ulna until reaching the limit of tissue resistance. Specific findings observed are the amplitude of excursion, the quality of the two end points, and any symptoms produced during the examination. Testing is first performed in neutral forearm rotation where laxity is the greatest. Testing is then done with the forearm positioned at the limits of supination and pronation. Typically, at the limits of forearm rotation, physiologically normal laxity is reduced, and the discrepancy with pathological instability becomes more evident. Testing is repeated back and forth between the two sides and in the various positions of forearm rotation until the examiner is able to make a clear determination.

The examiner stabilizes the patient's distal ulna between thumb and forefingers. The examiner grasps the patient's radius with his other hand and translates the radius volarly and dorsally, noting amplitude and quality of the end point
Surgical Technique
The patient is positioned supine on a hand table with an overhead boom for arthroscopy using finger trap traction. After the induction of anesthesia, the RUL integrity examination is repeated on the uninvolved side and the affected side, noting any discrepancies compared to the awake examination. After prepping and draping, surgery begins with arthroscopy of the DRUJ using a 1.9-mm arthroscope and opposing dorsal radial and volar ulnar portals according to a previously described technique [6]. Avulsion of the RUL from the ulnar fovea is confirmed before proceeding with the open incisions and free tendon graft reconstruction (Fig. 3). The primary working incision is a 4-cm L-shaped midaxial incision at the distal ulna with the transverse limb in the ulnar wrist crease. The most important precaution observed during every step of the case is meticulous protection of the dorsal ulnar cutaneous nerve branch. The DRUJ is entered volar to the base of the ulnar styloid. This leads directly to the fovea and leaves the structure of the extensor carpi ulnaris subsheath undisturbed. Post-traumatic scar and loose tissue not already debrided during the arthroscopy are cleared, permitting visualization of the volar and dorsal margins of the sigmoid notch, deep to the remaining amount of fibrocartilage disk (quantity varies case by case).

The integrity of the RUL insertion to the ulnar fovea is tested with direct DRUJ arthroscopy, with the 1.9 mm arthroscope in the volar ulnar portal and shaver/probe in the dorsal radial portal
Three total drill holes are created, each by the same series of steps: landmark the path with a 1.4-mm K-wire, confirm fluoroscopically, sequentially expand the diameter of the hole with drill bits (2.0, 2.5, 2.8, and 3.2 mm). The locations of the drill holes correspond precisely to the true anatomic points of attachment of the original RUL. The first is from the volar margin of the sigmoid notch immediately adjacent to the undersurface of the fibrocartilage disk passing coronally through the radial metaphysis to exit at the insertion of the brachioradialis (Fig. 4). The second passes from the dorsal margin of the sigmoid notch immediately deep to the fibrocartilage disk to an exit a few millimeters away from the first (Fig. 5). The third passes from the ulnar fovea to the proximal subcutaneous border of the ulna (Fig. 6). The first two radial tunnels represent the uniquely different technique described in this article. The ulnar tunnel is standard, similar to previous descriptions.

The first drill tunnel is made from the volar margin of the sigmoid notch across to the footprint of the brachioradialis

The second drill tunnel is made from the dorsal margin of the sigmoid notch across to the footprint of the brachioradialis

The third drill tunnel is made from the ulnar cortex to enter the fovea
A free palmaris longus graft is harvested from the ipsilateral wrist and each end is secured with a 3–0 non-absorbable braided Krackow suture with long tails. The graft is passed through the ulnar tunnel such that the limb of the palmaris graft exiting the proximal end of the ulnar tunnel passes volar to the styloid base to reach the fovea, crosses the other limb (to which it is anchored with a suture) and passes onwards to become the dorsal limb of the RUL reconstruction (Fig. 7). The limb of the palmaris graft exiting the distal end of the ulnar tunnel becomes the volar limb of the RUL reconstruction. These limbs are retrieved through the two drill tunnels in the radius using suture passers inserted from a second small counter incision overlying the tunnels' exit points at the brachioradialis insertion (Figs. 8 and 9). Once they have been pulled through and tensioned (Fig. 10) they can be shortened and a new Krackow suture placed to keep the ends of the grafts just inside the exit points of the tunnels such that the two 3–0 braided sutures tie to each other over the bone bridge at the footprint of the brachioradialis. Final tying of sutures that tension the tails of the graft is not performed until first the DRUJ is congruently reduced in mid-supination and held there by two extra-articular 1.4-mm K-wires placed across four cortices from ulna to radius.

The palmaris longus graft is first threaded through the ulnar drill tunnel

Through a small counter incision radially at the exit point of the two drill holes, with careful protection of the superficial radial nerve, suture retrievers are passed back to the ulnar wound to retrieve the two ends of the palmaris longus graft

Each end of the palmaris graft that has been fixed with a 3–0 non-absorbable braided Krackow suture is captured by one the two suture retrievers passed through the radial tunnels from the radial side

Once the graft ends are successfully tensioned through the radial drill holes, they may then be shortened so that only suture material is tied over the bone bridge between exit points to avoid the bulk of a tendon weave
The reconstruction is immobilized in a sugar tong splint for 4 weeks, at which point the K-wires are removed. The patient spends an additional 2 weeks in a below elbow orthoplast splint before beginning active forearm and wrist range of motion exercises. Light strengthening is not initiated until 8 weeks, heavy strengthening until 3months.
Results
All 25 patients demonstrated distal radioulnar joint stability to physical examination stress testing at the 6 month visit. Mean ranges of motion, in degrees, pre-/post-operative were: wrist flexion 53 (±13)/61 (±10), wrist extension 53 (±13)/62 (±15), supination 65 (±12)/74 (±7), and pronation 66 (±11)/71 (±8). Grip strengths expressed as % contralateral pre-/post-operative were: 57 (±23)/79 (±25). The differences in these measures were not found to be statistically significant. The mean pre-/post-operative DASH scores were: 62 (±16)/7(±3). This difference was found to be statistically significant. Improvements in the DASH score were contributed to by less pain overall but primarily by the ability to better perform tasks requiring complex movement patterns with resistance in work and sports. All the patients were able to continue their original occupations and return to their chosen recreations once fully healed. Specific complications sought out but not identified were: infection, pin migration or breakage, loss of graft fixation, wound breakdown, injury to the dorsal cutaneous branch of the ulnar nerve, superficial radial nerve, or lateral antebrachial cutaneous nerve.
Discussion
The inherently unstable DRUJ relies heavily on ligamentous support [3,10,20]. The prime stabilizer is the RUL [5,13,17,21]. Traumatic RUL deficiency can lead to symptomatic instability for some patients. Not all patients with RUL deficiency are highly symptomatic. Whether RUL deficiency leads to DRUJ arthritis over time is also not certain. Therefore, it is not axiomatic that every patient who links a specific traumatic event to the subsequent demonstration of DRUJ instability necessarily needs to undergo surgery [7]. Certainly, patients who lack the history of a traumatic event and demonstrate only physiologic laxity should not be considered candidates for ligament reconstruction. Even for those with true pathologic instability, some less physically demanding patients have been ultimately satisfied with non-surgical care. Radioulnar ligament deficiency appears to be most symptomatic in those patients who perform complex three-dimensional motions of the forearm and wrist against resistance. It is this active group of patients who are most likely to request surgery. Restoration of DRUJ stability is problematic owing to the complexity of the local anatomy. The original reconstructions for DRUJ instability were entirely non-anatomic tethers, primarily employing the extensor carpi ulnaris [14]. The next generation of reconstructions achieved anatomic replication of the ulnar foveal attachment but not the radial attachments [1,8,19]. These do not fully restore DRUJ stability in the lab setting or clinically [4,7,8]. Nine patients underwent palmaris longus tendon graft reconstruction with a single sagittal plane drill tunnel in the distal radius; two of the nine patients developed recurrent instability and the average forearm arc of motion was reduced 14° compared to pre-operative [19]. Twelve out of 14 patients surveyed at a mean of 2.2 years post-operatively were felt to have achieved stability following a similar reconstruction, although only nine of 14 had pain relief [1]. Pronation was reduced to 84 % of contralateral, supination to 80 % of contralateral; no patient outcomes measures were used in the study [1]. The next step in the evolution of RUL reconstruction replicates the true anatomic points of insertion both at the ulnar fovea and at the volar and dorsal margins of the sigmoid notch. The expectation is that by more accurately reproducing the original anatomy, better stability will be achieved with less opportunity for reduced motion. Whether this method is actually any better than others cannot be determined as the only studies available are level IV case series.
Even if comparison of one level IV case series to another were of benefit, we are all still hampered by the lack of better measurement tools. The objective physical measurements employed in this study (range of motion and grip strength) are of little use in demonstrating that the surgery has helped the patient in that they are not very deranged preoperatively. Even though each of these objective measures did improve with surgery (supination the most), the differences were not statistically significant. The purpose in measuring them during this study was simply to make sure that they were not dramatically worsened by the surgical intervention. The pre-operative arthroscopic demonstration of chronic anatomic detachment of the RUL at the fovea is a very objective assessment of the pathologic state [6,15,16]. If we had performed post-operative arthroscopy, that would have demonstrated whether the graft was still attached or had failed during rehabilitation, but anatomic attachment does not guarantee clinical stability. Similarly, MRI is a less accurate, but still objective, measure of attachment, but it also is not a measure of clinical stability [2,9,18]. The objective assessment of stability continues, for the time being, to be dependent on the manual ligament stress test performed by the examiner [6,7]. The more experienced and specialized the examiner, the more likely his examination will accurately reflect the state of the RUL. But, we do not yet have in our field any universally agreed upon criteria for the ligament integrity examination, a grading system, or intra-/inter-observer statistics derived from a gold standard.
The pre-operative to post-operative comparison that best reveals any improvement experienced by the patients is the DASH score, which is a subjective measure, but relevant in that it reflects patient satisfaction with limb function. The DASH has value in that it is more regionally specific than a broad measure such as the SF-36 and can be compared across various upper extremity conditions. The weakness of the DASH is that it is not specifically directed to the complex wrist functions of a patient with DRUJ instability. It would have been better if we had employed a different and more wrist specific outcomes measure. These various shortcomings will continue to limit conclusions that can be drawn for the topic of RUL reconstruction.
Conclusion Reconstruction of the RUL with a free palmaris longus tendon graft using the truly anatomic points of original RUL attachment at both the ulna and radius restored DRUJ stability and improved DASH scores without limiting forearm or wrist motion.
Footnotes
Nothing to disclose.
The authors declare that they have no conflicts of interest, commercial associations, or intent of financial gain regarding this research.