
Abstract
Introduction
The reduction and association of the scaphoid and lunate (RASL) is a procedure to treat chronic static scapholunate (SL) dissociation which involves open excision of the SL ligament, debridement of the joint surfaces to facilitate fibrous union, reduction of the SL, and fixation with a headless compression screw to allow for independent rotation of the two bones along the screw axis [11,15,16]. Several variations with temporary or permanent SL screw fixation have been described [1,5,6,13]. Although complications have been reported, there have been no reports of avascular necrosis (AVN) of the scaphoid related to SL screw fixation.
Case Report
A 28-year-old right hand dominant female with no previous history of wrist pain sustained an injury to her left wrist in a motor vehicle collision. She had wrist pain, underwent radiographs (reported as normal), and was subsequently referred to an orthopedic surgeon. Repeat radiographs of the wrist were interpreted as unremarkable (Fig. 1). She was diagnosed with a nonspecific left wrist sprain and was told to gradually resume activities as tolerated.

PA (
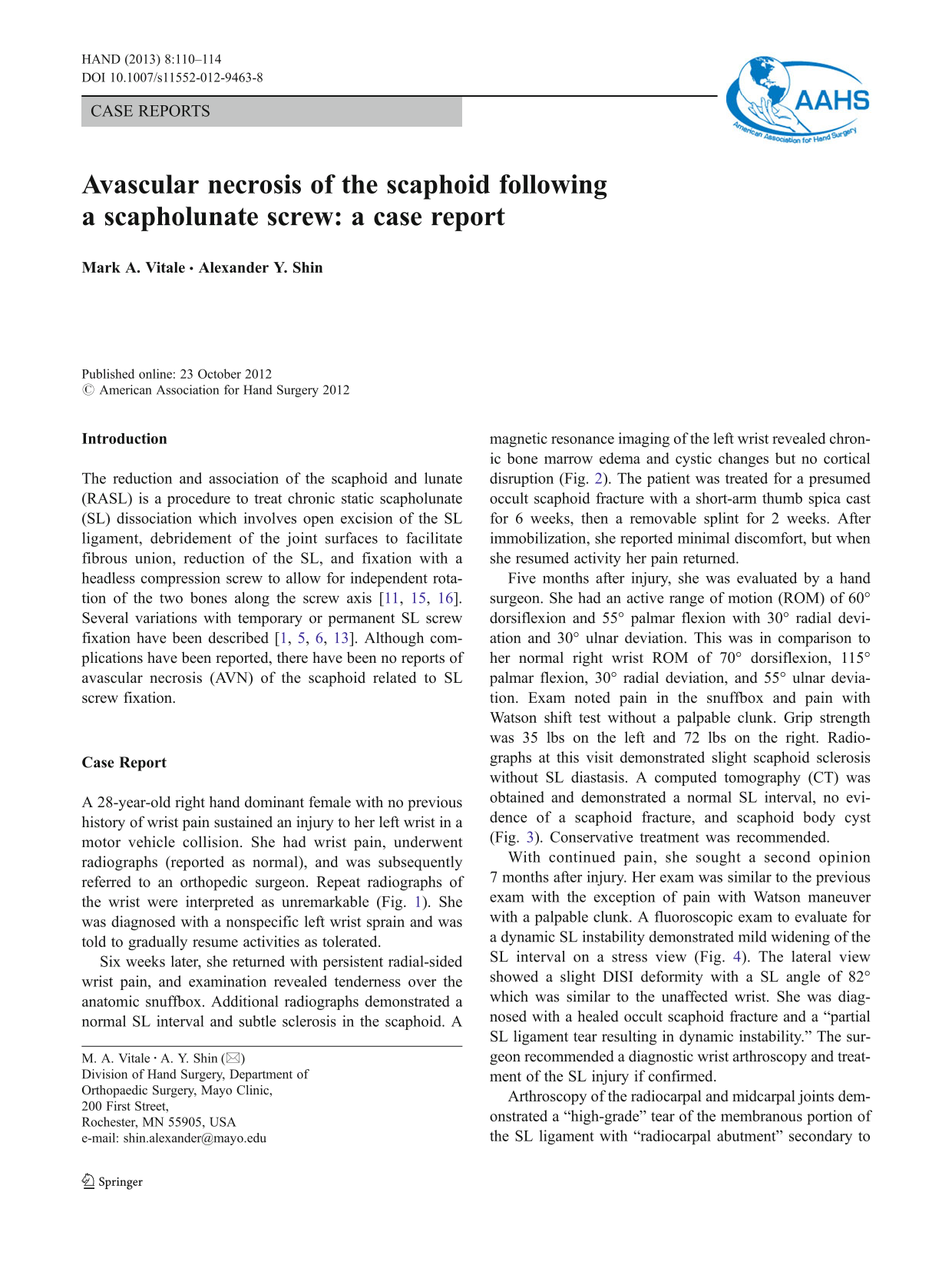
Six weeks later, she returned with persistent radial-sided wrist pain, and examination revealed tenderness over the anatomic snuffbox. Additional radiographs demonstrated a normal SL interval and subtle sclerosis in the scaphoid. A magnetic resonance imaging of the left wrist revealed chronic bone marrow edema and cystic changes but no cortical disruption (Fig. 2). The patient was treated for a presumed occult scaphoid fracture with a short-arm thumb spica cast for 6 weeks, then a removable splint for 2 weeks. After immobilization, she reported minimal discomfort, but when she resumed activity her pain returned.
T1 coronal (
Five months after injury, she was evaluated by a hand surgeon. She had an active range of motion (ROM) of 60° dorsiflexion and 55° palmar flexion with 30° radial deviation and 30° ulnar deviation. This was in comparison to her normal right wrist ROM of 70° dorsiflexion, 115° palmar flexion, 30° radial deviation, and 55° ulnar deviation. Exam noted pain in the snuffbox and pain with Watson shift test without a palpable clunk. Grip strength was 35 lbs on the left and 72 lbs on the right. Radiographs at this visit demonstrated slight scaphoid sclerosis without SL diastasis. A computed tomography (CT) was obtained and demonstrated a normal SL interval, no evidence of a scaphoid fracture, and scaphoid body cyst (Fig. 3). Conservative treatment was recommended.

Coronal (
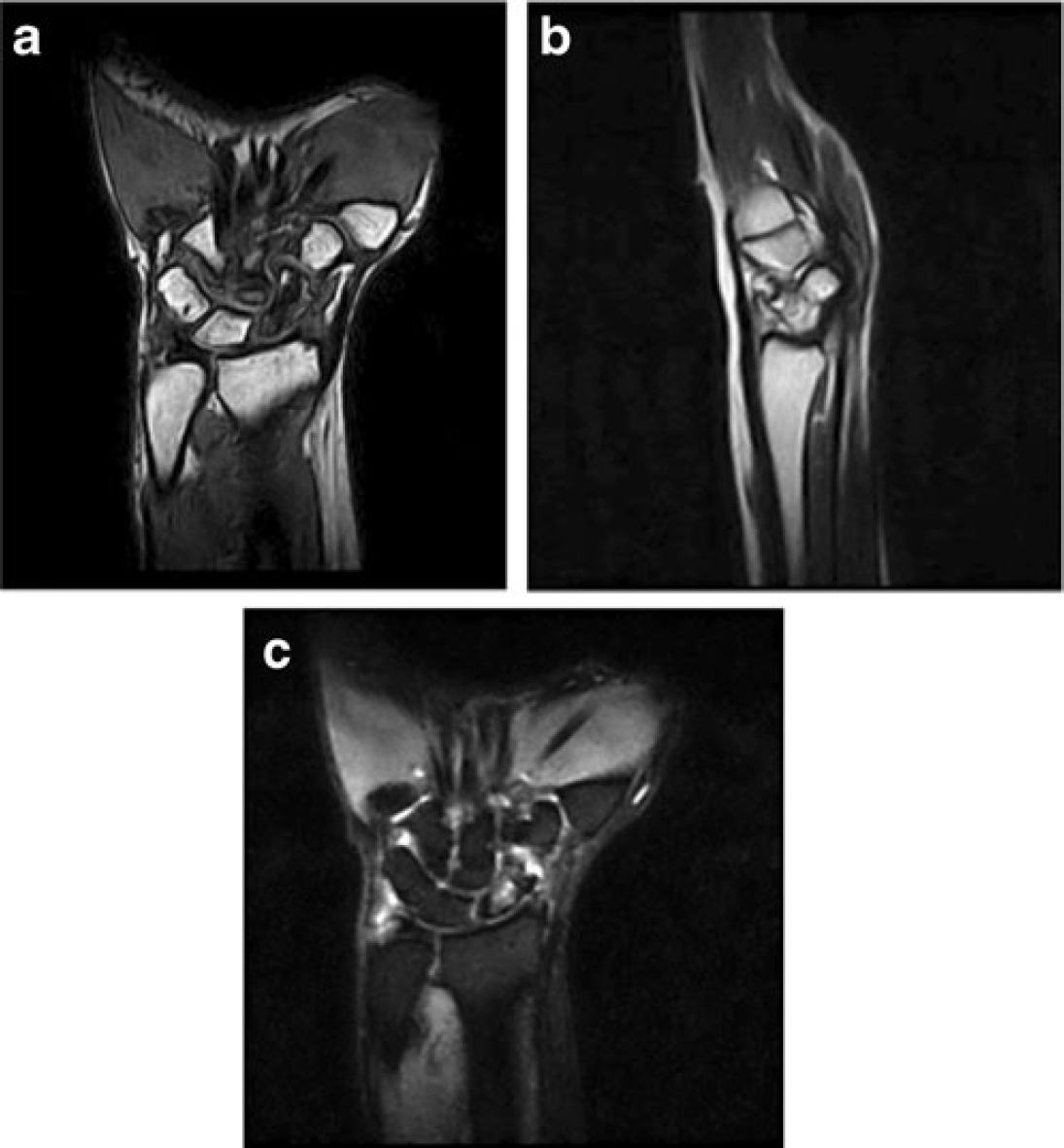
With continued pain, she sought a second opinion 7 months after injury. Her exam was similar to the previous exam with the exception of pain with Watson maneuver with a palpable clunk. A fluoroscopic exam to evaluate for a dynamic SL instability demonstrated mild widening of the SL interval on a stress view (Fig. 4). The lateral view showed a slight DISI deformity with a SL angle of 82° which was similar to the unaffected wrist. She was diagnosed with a healed occult scaphoid fracture and a “partial SL ligament tear resulting in dynamic instability.” The surgeon recommended a diagnostic wrist arthroscopy and treatment of the SL injury if confirmed.
PA (
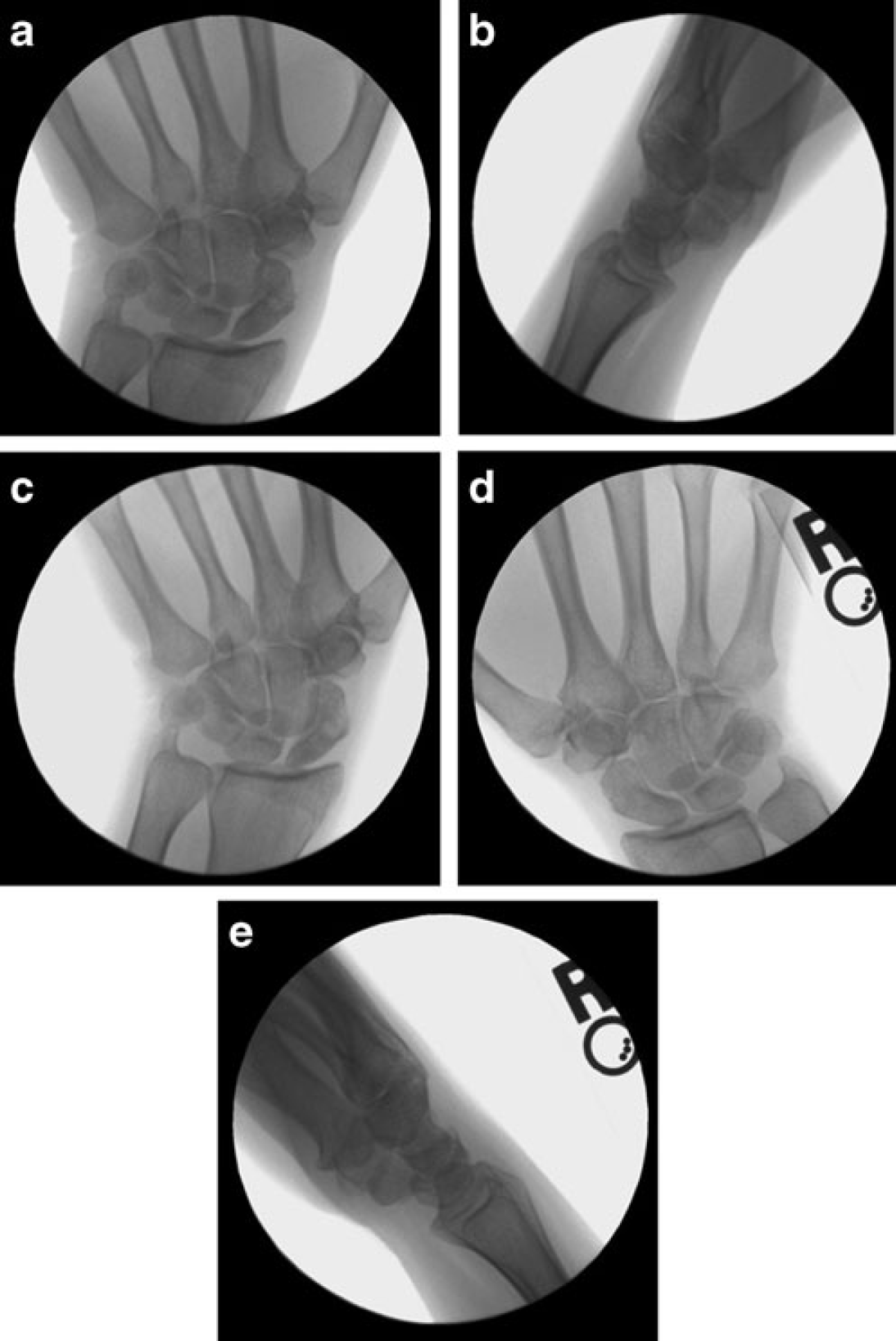
Arthroscopy of the radiocarpal and midcarpal joints demonstrated a “high-grade” tear of the membranous portion of the SL ligament with “radiocarpal abutment” secondary to SL rotation (Fig. 5a-e). Visualized from the midcarpal portals, the SL interval revealed no diastasis at rest (Fig. 5c), but “significant” diastasis with a manual Watson shift test (Fig. 5d). There was no arthroscopic evidence of a scaphoid fracture at the proximal or distal poles. Continued conservative treatment was recommended.
Arthroscopic images of left radiocarpal joint from the three to four portal
Two weeks later (8.5 months status post injury), after a discussion of the arthroscopic findings and treatment options, the patient was offered surgery consisting of an open examination of the SL ligament and a RASL procedure if SL instability was confirmed. A dorsal ligament sparing approach was performed and chronic attenuation of the dorsal SL ligament which was not amenable to repair was reported. After a radial styloidectomy and reduction of the SL interval, the SL articulation was held reduced with a single 22.0-mm by 2.0-mm cannulated headless compression screw. The osteocartilaginous fragments off the scaphoid were debrided, and the SL ligament was secured with a 3-0 braided nylon suture. The dorsal intercarpal ligament was secured to the insertion of the scaphoid with a braided nonabsorbable #2 suture.
The patient was immobilized for 12 weeks. At 2 months postoperatively, the patient noted slowly improving post-surgical pain but never felt complete resolution. Examination revealed continued decreased wrist ROM and grip strength with dorsal tenderness. Radiographs revealed maintenance of reduction of the SL interval, but changes consistent with AVN of the scaphoid were present (Fig. 6). Pain increased in the radial aspect of her left wrist over the ensuing weeks, and at 5 months postoperatively, active ROM of the left wrist was 50° volar flexion and 40° painful dorsiflexion, and grip strength diminished to 20 lbs compared to 60 lbs in her right hand. Radiographs revealed progressive AVN of the scaphoid with sclerosis of the proximal pole and collapse and degenerative changes of the radioscaphoid articulation (Fig. 7).

PA (

PA (
Ten months status post surgery (17 months since initial injury), she reported severe pain and stiffness of her left wrist preventing her from many activities of daily living. She was counseled regarding salvage options and has chosen not to pursue these at this time.
Discussion
The RASL procedure is an established technique for the treatment of reducible chronic static SL dissociation in the absence of significant arthrosis [11,15,16]. Long-term follow-up of the RASL procedure demonstrated diminished pain, maintenance of 80 % of the flexion–extension arc, and grip strength comparable to the contralateral side at an average of 6.4 years follow-up [19]. Postoperative pain and DASH scores indicated low level of disability and radiographs revealed decreases in the SL gap and SL angle in all patients. Only 3 of 31 patients required additional surgeries, and complications were reported including osteolysis around the screw in one case and two other patients were classified as treatment failures with progression of SLAC wrist later treated with salvage procedures. No cases of AVN were reported.
Reported complications from the RASL procedure or its modifications have been sparse [1,5,6,11,13,15,16]. In 2011, Cognet et al. reported their results of a modified RASL in seven patients after arthroscopic debridement of the SL ligament [6]. Their technique was an arthroscopic rather than an open approach, and the SL surfaces were not decorticated. Additionally, wrists were immobilized for only 2 weeks. Loosening of the SL screws with partial destruction of the lunate and/or scaphoid was present in all cases. The screws were removed in all patients within 6 months and four patients required salvage procedures.
There have been limited reports of scaphoid AVN after scaphoid fracture repair [8,9], SL ligament repair and dorsal capsulodesis [2], and three-ligament tenodesis [7], but AVN of the scaphoid following SL screw fixation with the RASL procedure or other methods of SL screw fixation has not been reported to our knowledge. There are several potential etiologies for the development of AVN in this patient. One possibility is that surgical exposure may have disrupted the major blood supply to the scaphoid, the dorsal ridge vessels [4,10,18]. Additionally, the SL screw insertion itself may have directly disrupted intraosseous vascular channels to the scaphoid. Furthermore, multiple K-wire insertions for either placement of the SL screw or for joysticks to facilitate reduction may have caused thermal necrosis to the scaphoid and surrounding soft tissues.
Pre-existing Preiser's disease may have been a contributing factor in the present case, although Preiser's is classically thought to represent an idiopathic atraumatic cause of AVN of the scaphoid in contrast to the acute traumatic injury in this case. Additionally, AVN of a nonunited occult scaphoid fracture may have been present prior to surgery, although this is less likely in the setting of a completely nondisplaced fracture which appeared healed radiographically. If either Preiser's disease or AVN of a scaphoid nonunion was in fact part of the pathophysiology of this patient's presentation, however, the scaphoid may have not had the structural integrity to accept SL screw fixation. It is interesting to note that this patient's diagnosis of SL ligament injury was not apparent until 7 months after her initial injury, as AVN of the scaphoid has been described as a cause for SL ligament dissociation and carpal instability [14]; it remains possible that a developing Preiser's disease may have resulted in attenuation of the SL ligament and/or avulsion of the osseus attachments of the SL ligament.
Concomitant scaphoid fracture and SL ligament injury, once thought to be mutually exclusive injuries except in high-energy perilunate fracture dislocations, represent a combined injury pattern that has likely been historically underappreciated; several authors have examined acute scaphoid fractures arthroscopically or via open surgical exploration and reported an incidence of partial or complete SL ruptures ranging from 8 to 71 % [3,12,17,20]. A history of a healed scaphoid fracture with a SL ligament injury may represent a situation worthy of special consideration in the treatment of SL instability. The use of the RASL technique or other modifications of SL screw fixation for SL reconstruction in the face of a previous scaphoid fracture should be carefully evaluated and may represent a relative contraindication to this procedure.
Footnotes
The authors declare that they have no conflicts of interest, commercial associations, or intent of financial gain regarding this research.