
Abstract
Background
Differentiating chronic from acute injuries of the collateral ligament of the metacarpophalangeal joint (MCPJ) of the thumb can be difficult in the absence of a conclusive history and examination. We aimed to establish the presence of a radiological sign in patients with a chronic injury and the reliability of the sign in differentiating chronic from acute ligament injury.
Method
Consecutive patients undergoing surgical treatment for chronic (n=14) or acute (n=8) ligament injury of the MCPJ of the thumb were identified retrospectively. Six upper limb orthopedic surgeons and four musculoskeletal radiologists were recruited from three regional centers. Observers judged the presence or absence of the sign, an exostosis at the level of the neck of the thumb metacarpal, on radiographs presented on a computer program. The radiographs were then observed in a different random order. The sensitivity, specificity, positive predictive value (PPV), and negative predictive values (NPV) of the radiological sign were evaluated for each observer and the intra- and interobserver error was calculated.
Results
The mean observer specificity and sensitivity for the sign were 84 and 54 %, respectively. The PPV and NPV were 89 and 52 %, respectively. The kappa statistic for intraobserver error was 0.69 and interobserver error 0.34. Conclusions A radiological sign associated with chronic collateral ligament injuries of the MCPJ of the thumb is established. The presence of the sign can increase the confidence of the clinician in differentiating chronic from acute collateral ligament injuries, when history and examination are inconclusive in this respect.
Background
Injury of the collateral ligament of the metacarpophalangeal joint (MCPJ) of the thumb is common, particularly amongst skiers and ball-handling athletes [2], and can lead to disabling joint instability. The mechanism of acute injury to the ulnar collateral ligament is sudden forced abduction, with injury to the radial collateral ligament requiring forced adduction. Chronic injuries to either ligament occur with repeated trauma causing chronic ligamentous laxity [1] or with delayed presentation of acute injury. An injury to the collateral ligament in this study refers to a complete tear of the proper collateral and/or the accessory collateral ligament.
In most cases, clinical evaluation by history and examination allows differentiation of chronic from acute injury. The history for patients with chronic injury can be more difficult to identify, presenting with recurrent trauma, a sense of instability of the thumb, pincer grip weakness, or difficulty grasping objects [6]. The reference standard for diagnosis of an injury is clinical stress examination in flexion and extension [12, 16]. Examination in acute injury reveals bruising, swelling, and tenderness at the MCPJ; these signs are unlikely in chronic injury. Routine investigation includes anteroposterior (AP) and lateral thumb radiographs to identify avulsion fractures and exclude other fractures. If the diagnosis of instability is uncertain, stress radiographs can be performed [16]. Ultrasound and magnetic resonance imaging (MRI) have been used to discriminate simple avulsions from Stener lesions [4, 8, 11].
For acute unstable injuries, an acute repair is advocated [16], with bone anchors giving excellent results [3, 17]. At more than 3 weeks between injury and surgery, “chronic” cases require reconstruction rather than repair [13, 15], with a tendon graft giving good results [5]. Optimal operative planning prior to surgical treatment is more difficult in the minority of patients whose history and examination are inconclusive in relation to the chronicity of the injury. A further means of helping distinguish chronic from acute injury would be useful.
We have observed a radiological sign on plain radiographs of the thumb in patients with chronic injuries of the collateral ligament of the MCPJ. The aim of the study was to establish the presence of this sign in patients with chronic injury and the reliability of the sign in differentiating chronic from acute ligament injury.
Materials and Methods
This was a prospective study on retrospectively collected material (radiographs). Consecutive patients undergoing surgical treatment for chronic (n=14) or acute (n=8) ligament injury of the MCPJ of the thumb under the care of the senior author between 2006 and 2008 were identified by reviewing the operative logbook (Table 1). For the purposes of this study, acute injuries were defined as presenting within 4 weeks of injury and chronic injuries after this period. Patients with acute injuries underwent repair, whereas those with chronic injuries underwent reconstruction.
The chronic and acute ligament injuries to the MCPJ of the thumb

Denotes the number of patients with the radiological sign as determined by the authors after careful scrutiny of the plain radiographs
Only patients with a conclusive history and examination (with respect to chronicity) and consistent intraoperative findings were included. The diagnosis of injury had been established preoperatively based on standard history and examination including stress examination in flexion. All patients had AP and lateral plain radiographs. In 10 cases, plain radiograph stress views or ultrasound stress views were performed for confirmation of instability and one case had an MRI scan. Patients under the age of 16 years were excluded.
The AP and lateral thumb plain radiograph images for each patient were obtained (Institutional Review Board approval was not required by the institution). The authors examined the patients' radiographs to determine which they considered to have the radiological sign as described (Table 1). Six upper limb orthopedic surgeons (five consultants and one hand fellow) and four consultant musculoskeletal radiologists were recruited as observers from three regional centers. A computer slide show was designed to present the images to the clinicians. The 22 sets of radiographs of chronic and acute injuries were arranged in random order determined by a computer random number generator. The series was then repeated in a second random order. The first page demonstrated an example of the radiological sign found in chronic collateral ligament injuries as shown in Fig. 1. The sign is described as a bony exostosis at the thumb metacarpal neck in the distal radial or ulnar aspect on the AP view and often on the dorsal cortex on the lateral view. Each observer judged the presence or absence of the radiological sign for each set of radiographs on the computer slide show.

The radiological sign: an exostosis at the neck of the thumb metacarpal. Anteroposterior and lateral radiographs of the thumb. The sign is indicated by the arrow on the anteroposterior and lateral views
We compared observations for chronic collateral ligament injuries with acute collateral ligament injuries. The sensitivity, specificity, positive predictive value (PPV), and negative predictive values (NPV) of the sign were evaluated for each observer. The mean and standard deviation for these values across the observers was calculated. Each observer assessed the radiographs on two occasions, allowing derivation of the intraobserver error. The intraobserver error and the interobserver agreement were calculated using kappa statistics. In addition, an intraoperative biopsy of the exostosis in a patient undergoing a reconstruction for a chronic collateral ligament reconstruction was obtained.
Results
There were a total of 440 possible responses by observers; from these, four (0.9 %) were not completed. The characteristics of the patients are shown in Table 1. The sensitivity, specificity, PPV, and NPV for the radiological sign are shown in Table 2, both for all cases (a) and for the subset of chronic cases that were confirmed sign-positive by the authors (b). The mean observer concordance for the radiological sign was 86 %, giving an intraobserver error of 14 %. The kappa statistic compares the extent of agreement observed against how much would be expected to occur by chance alone. The kappa value for the intraobserver reliability was 0.69, interpreted as substantial intraobserver reliability [9]. The kappa statistic for the interobserver reliability was 0.34, interpreted as “fair” agreement between observers [9]. The histology of the bony exostosis revealed it was composed of woven bone.
The observations of the sign in chronic collateral ligament injuries versus acute collateral ligament injuries
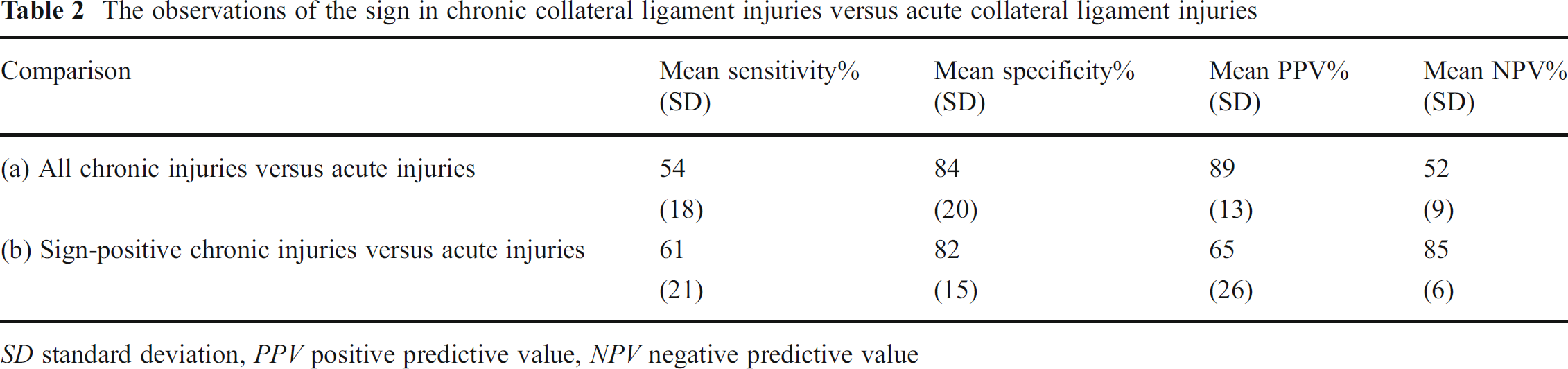
SD standard deviation, PPV positive predictive value, NPV negative predictive value
Discussion
This study has established a radiological sign in patients with chronic collateral ligament injuries of the MCPJ of the thumb. In the context of distinguishing chronic from acute injuries, the sign has good specificity, positive predictive value, and intraobserver reliability and acceptable interobserver reliability. When present, the sign can increase the confidence of the clinician when the chronicity of injury is in doubt. For example, a patient may present with a history of recent injury and pain in the thumb MCPJ, but a clinical examination more consistent with chronic ligament injury. Identification of the sign can aid preoperative decisions regarding the appropriate choice of surgical procedure and help in the preoperative counseling of the patient. The sign shows low sensitivity, which means that absence of the sign cannot be used to exclude a chronic injury.
Exostoses of the thumb in response to injury have previously been described. Wissinger et al. [18] described a series of 10 cases of turret exostoses in the dorsal aspect of the phalanges of the hand as a rare complication of minor trauma. A case of turret exostosis in the distal fifth metacarpal reported by Rubin and Steinburg [14] and of the volar aspect of the distal phalanx of the thumb by Mohanna et al. [10] after similarly minor trauma. The pathogenesis was postulated to be the presence of a wound of the dorsal periosteum followed by the formation of a subperiosteal hematoma. The drainage of the periosteum is obstructed and the maintenance of the osteogenic properties of the periosteum overlying the hematoma results in hematoma ossification over a period of months.
The woven bone seen on the histology of one patient's lesion is consistent with previous histology of the turret exostosis [18]. We postulate that the exostosis develops by a similar mechanism of a contained subperiosteal hematoma adjacent to the distal metacarpal after the collateral ligament rupture. This then ossifies over time, becoming evident on the radiographs of the chronic collateral injury group, but not seen on radiographs of the acute collateral ligament injuries. Of note, the presence of a small hematoma on ultrasound is a strong confirmation of the presence of a collateral ligament rupture and is usually found at the metacarpal side [7]. This would account for the presence of the exostosis at the metacarpal neck as opposed to the most common site of injury of the ligament, the phalangeal side. The 12 patients identified by the authors as having the sign presented at least 2 months after their apparent injury, indicating that the exostosis may take this period of time to develop.
An interesting and unexpected finding in our cohort is that in 6 of the 14 cases, the sign was found on the contralateral side to the collateral ligament injury. This may suggest that the exostosis can be formed from subperiosteal hematoma formation due to the ligament rupture itself or by a contrecoup injury mechanism from the proximal aspect of the proximal phalanx. An alternative explanation for the exostosis might have been that this was a simple osteophyte secondary to degenerative changes. However, on radiological and routine intraoperative review, no cases showed signs of osteoarthritis. We are only able to draw limited conclusions regarding laterality of the sign in this study, as we did not ask observers to document the side on which the sign was identified.
The study was limited by the relatively small number of cases, though the 10 independent observers increased the total number of observations. Contralateral thumb radiographs were not taken, but would rule out the possibility of an underlying symmetrical abnormality. The radiographs were assessed by observers in the absence of their clinical context, as was necessary to ensure blinding to the diagnosis. A study reviewing the use of this sign in clinical practice and its laterality would be of benefit.
A radiological sign associated with chronic collateral ligament injuries of the MCPJ of the thumb is presented. The presence of this sign can help the clinician differentiate between chronic and acute collateral ligament injuries in patients in whom the history and examination are inconclusive in this respect, contributing to the planning of appropriate surgical intervention.
Footnotes
All named authors hereby declare that they have no conflicts of interest to disclose.