
Abstract
Purpose
Enchondromas are the most common benign bone tumor affecting the hand. Standard treatment has consisted of curettage with bone grafting. It has become increasingly common for surgeons to use biologic cement in these cases. The purpose of this study was to evaluate different treatment options used to fill voids after curettage of hand enchondromas to determine if any provide more rigid fixation.
Methods
A cadaveric model of hand enchondromas was designed by making a standardized size corticotomy (0.6×1.0 cm) in 60 cadaver metacarpals. Resultant voids were then filled with either no material, bovine demineralized bone matrix (Synthes Paoli, PA, USA), or one of two different calcium phosphate bone cements: a carbonated apatite (Synthes Norian SRS Skeletal Repair System) and a hydroxyapatite (Stryker HydroSet) calcium phosphate. An apex dorsal three-point bend was applied to the metacarpals through an MTS machine, and load to failure and stiffness were recorded.
Results
Biomechanically, load to failure for intact metacarpals was significantly superior to those in which a corticotomy was created (p=0.04). There was a significant increase in load to failure between the metacarpals treated with the calcium phosphate bone cement and the negative controls (p=0).
Conclusions
In a biomechanical analysis of a cadaveric model of hand enchondromas, calcium phosphate bone cement provided significantly increased strength as compared to curettage alone and approximated the strength of intact metacarpals. It is unknown whether the use of biologic cements in this clinical setting leads to less postoperative immobilization, earlier digital motion, a quicker return to work, or increased patient satisfaction.
Keywords
Introduction
Enchondromas are the most common benign bone tumor affecting the bones of the hand. Traditionally, treatment of enchondromas of the hand with curettage and autograft has been considered the gold standard [7,14,15,18]. While long-term outcomes with this approach are good, taking autograft comes with donor site morbidity. In order to avoid this, several authors began to support simple curettage without bone grafting as an acceptable treatment for enchondromas of the hand [11,17,20]. In 2002, Goto et al. [10] proposed that replacement of the cortical window following curettage may lead to a faster recovery of the mechanical strength of the bone. As allograft bone became more readily available, it became an attractive alternative to autograft in filling post-curettage cavities in hand enchondromas [3,22].
Bone substitutes represent yet another option, which both avoid the donor site morbidity of autograft, as well as the potential disease transmission that could theoretically occur with allograft. Materials that have been studied in the hand literature include calcium phosphate bone cement [21], hydroxyapatite cement [13], and sterile plaster of Paris [2,8]. Yasuda et al. reported on ten cases of hand enchondromas treated with curettage and cavity filling with calcium phosphate bone cement. They found radiographic evidence of bony incorporation of calcium phosphate bone cement at final radiographic review, and all patients regained full range of motion postoperatively [21]. Similarly, in a prospective study of patients treated with curettage of a hand enchondroma and subsequent cavity filling with hydroxyapatite bone cement, there were no complications and all patients regained full hand function [13]. No local recurrences were seen after hand or foot enchondromas were treated with curettage and cavity filling with sterile plaster of Paris [8]. These articles suggest that bone substitute materials may provide a suitable alternative to allograft or autograft bone in the treatment of hand enchondromas.
While these techniques provide satisfactory long-term results, little has been studied regarding the more immediate postoperative period. Following curettage of an enchondroma, regardless of the void filler, most investigators support a period of postoperative immobilization until there is some radiographic evidence for healing. Keeping digits immobilized may lead to a delay in digital function and return to work. While all the treatment options previously discussed are acceptable for treating enchondromas of the hand, surgical techniques which allow for immediate postoperative range of motion and function are certainly appealing.
The purpose of this study is to determine the most rigid modality of metacarpal reinforcement after simulated curettage of an enchondroma. The hypothesis is that treatment of hand enchondromas with biologic cement is superior biomechanically to treatment with curettage alone, or curettage and bone grafting, and that the addition of biologic cement will approximate the strength of intact bone.
Materials and Methods
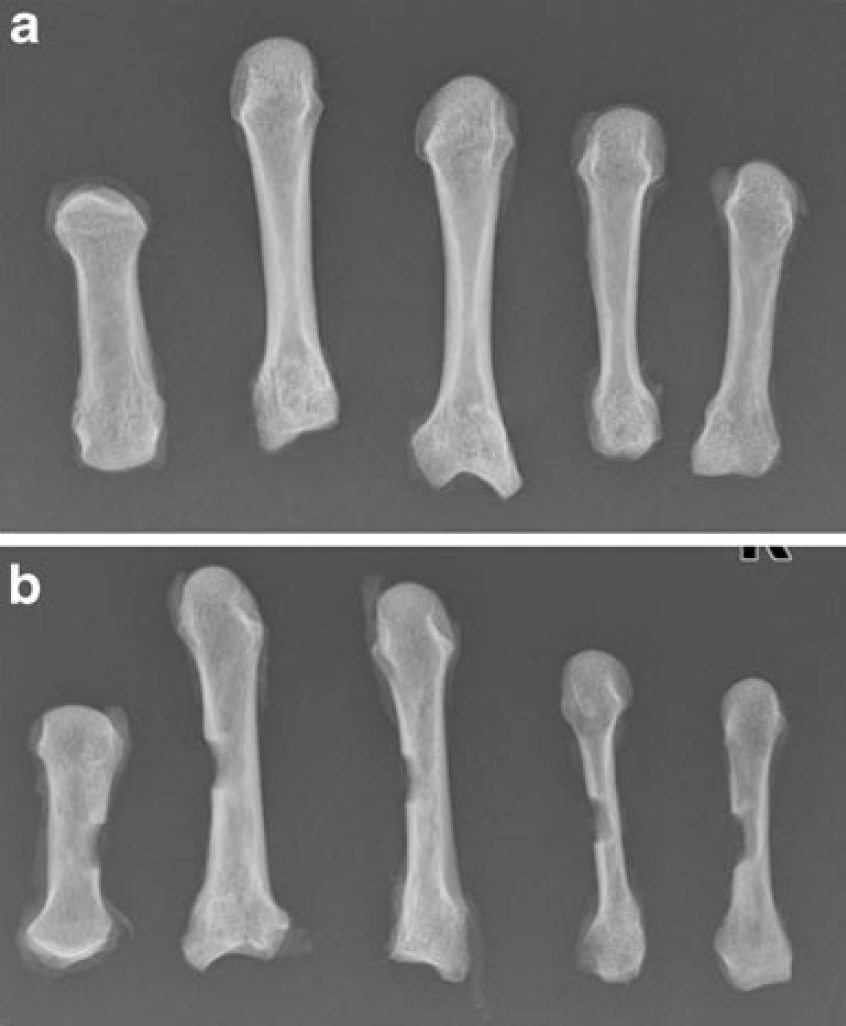
Twelve fresh frozen cadaver hands (60 digits) with a mean age of 55 years at the time of death were available for study. These cadaver hands were utilized to create a hand enchondroma model. Once thawed, hands were manually cleared of all soft tissues. Metacarpals were isolated and labeled thumb, index, middle, ring, and small accordingly. A highspeed burr was used to create a 1.0-cm×0.6-cm corticotomy on either the radial or ulnar side of the metacarpal, at the center point of the length of the ray as measured with a digital caliper. Clinically, enchondromas are often accessed from the radial or ulnar side of the metacarpal to avoid the extensor and flexor tendons. This particular size corticotomy was selected after the variability of the volar to dorsal dimensions of all metacarpals (thumb through small finger) was determined to accommodate the smallest of metacarpals in this study. The smallest metacarpals had volar to dorsal dimensions of greater than or equal to 0.6 cm in this cadaver sample. The proximal to distal dimension of 1 cm was selected to provide adequate access to the intramedullary canals. As little is published regarding the average size of enchondromas of the hand, local hand surgeons and musculoskeletal oncologists with academic affiliations were questioned and agreed that a 0.6-cm×1-cm corticotomy would be clinically appropriate. After the corticotomy was made, cancellous bone was removed from the medullary canal with a small curved curette. This replicated removal of the cartilaginous contents of an enchondroma. The resultant void represented the simulated enchondroma. Radiographs were taken from both intact samples and samples after corticotomy (Fig. 1). Bone mineral density by means of DEXA scanning was attempted, but technical limitations of the DEXA scanner available prevented the bone mineral density of such small bones from being acquired.
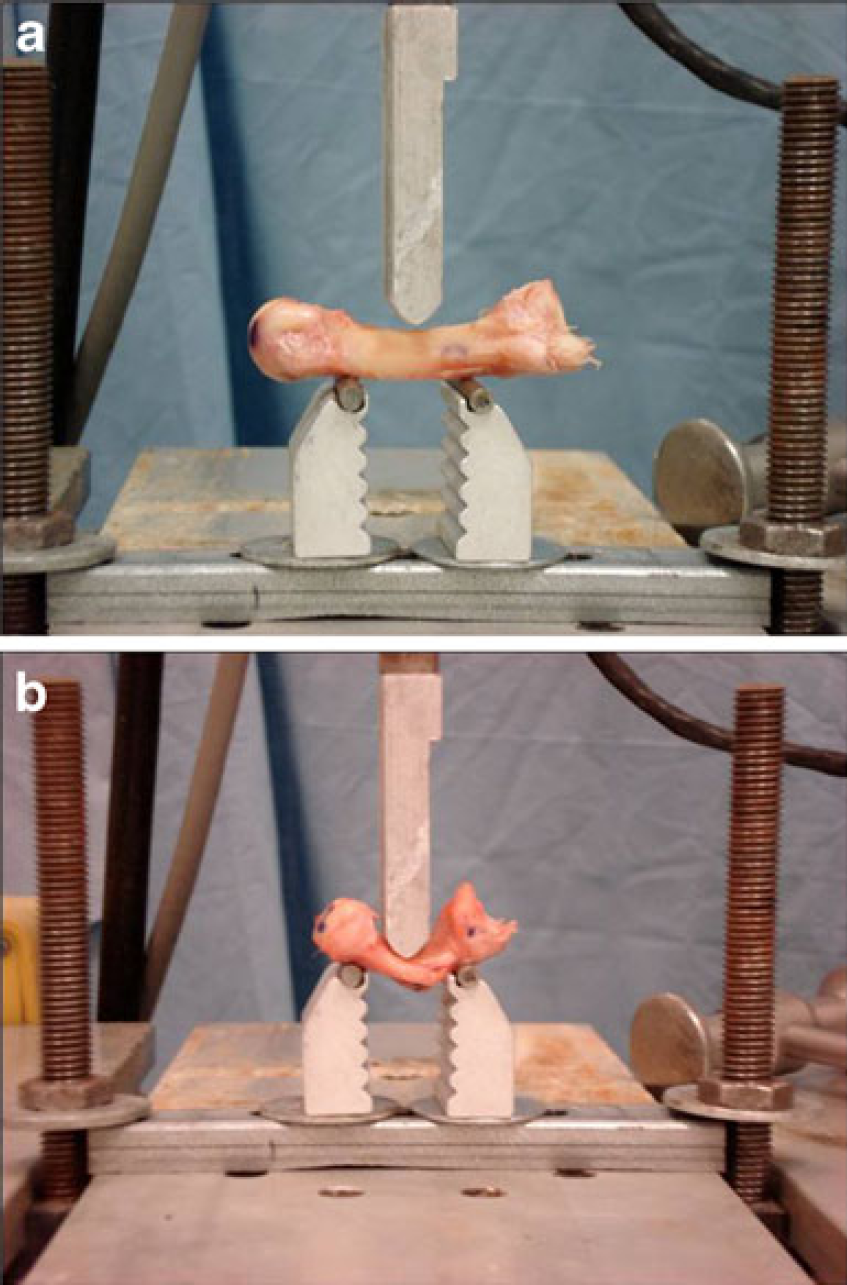
A pilot study was undertaken to assure that metacarpals could be tested in a three-point bending on an MTS machine. As stated previously, there have been no known publications describing biomechanical testing of hand enchondromas. Therefore, available literature for biomechanical testing of metacarpal fractures was used to guide the pilot study. Metacarpal fractures typically result in apex dorsal angulation because of the palmar force exerted by the interossei [1,4,6,16]. In this study design, the apex dorsal force commonly observed with metacarpal fractures was replicated with a three-point bend [5]. Since fracture of the digit is the primary concern after surgical curettage for treatment of a hand enchondroma, it was reasonable to use metacarpal fracture literature to guide the pilot study design. Metacarpals were tested at constant rates (0.1 mm/s) for load to failure, and failure was defined as the point of fracture (Fig. 2). Results from the pilot study supported the feasibility of the project design.
Individual metacarpals were then randomly assigned to one of the four test groups, consisting of 15 metacarpals per group. The first group of metacarpals, group 1, was kept intact and utilized as a positive control. Group 2 served as the negative controls. The five metacarpals of one hand in this group had corticotomies alone, with no fill material. The other ten metacarpals had corticotomies created that were filled with bovine demineralized bone matrix to simulate allograft bone grafting. Group 3 was treated with a carbonated apatite bone void filler, and group 4 was treated with a hydroxyapatite bone void filler.
Bovine demineralized bone matrix was selected to use in the negative control group—group 2. This material was thought to provide no additional structural stability when used to fill the bone voids of simulated enchondromas and therefore represented allograft cancellous bone. The demineralized bone matrix was fingerpacked into the voids while the metacarpals were at room temperature, as is done clinically.
The calcium phosphate bone cements used in groups 3 and 4 were prepared according to the manufacturer's recommendations [12,19]. The material used in group 3 was an injectable, moldable, and biocompatible calcium phosphate bone cement that sets at body temperature into a carbonated apatite. It reportedly achieves maximum compressive strength of 50 MPa, which is four to ten times that of cancellous bone, after setting for 24 h. The material used in group 4 was a calcium phosphate cement that converts to hydroxyapatite after curing at body temperature.
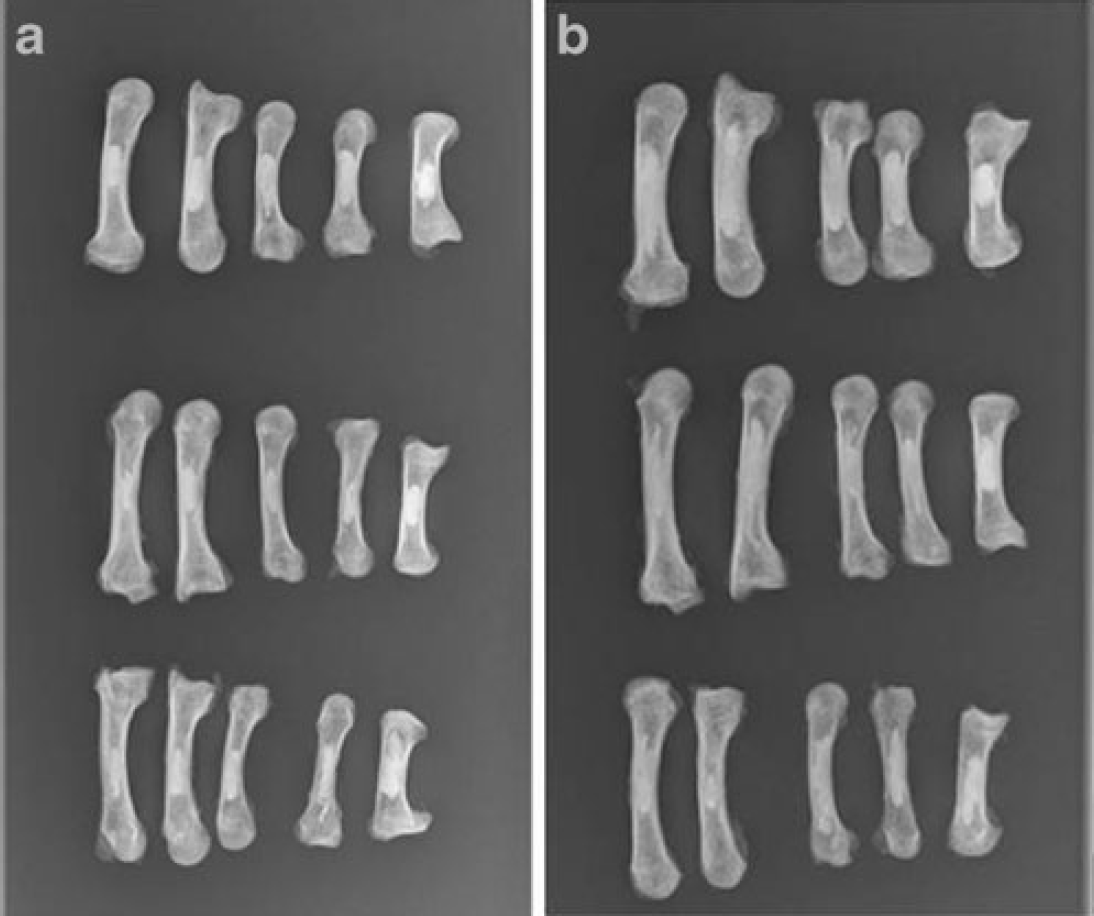
Like the demineralized bone matrix, the calcium phosphate bone cements were handpacked into the bone voids. While each calcium phosphate cement material was in its liquid phase, it was injected into the corticotomy site (Fig. 3). The cement was packed by hand into the void, refilling as needed, until dry. The same person handpacked all voids to standardize the amount of pressure applied. Radiographs were taken of the filled voids to assure uniformity of fill (Fig. 4). Physiologic conditions were simulated with a 37 °C bath of phosphate buffered saline (PBS). The calcium phosphate bone cement samples were placed into the PBS bath and allowed to cure in this bath solution for 24 h. Only after having cured for 24 h were the metacarpals in groups 3 and 4 tested on the MTS machine.

Handpacking of simulated metacarpal enchondromas with calcium phosphate bone cement
Statistics
As there was no precedence for biomechanical testing of hand enchondroma fixation techniques in the literature, a power analysis was devised based on the data from the pilot study. The pilot study found that the average intact metacarpal load to failure was 1,288±441 N. We chose to set 100 N as a significant difference in peak load to failure. Power analysis revealed that a sample size of 60 specimens with 15 in each group was sufficient to detect a clinically significant load of 100 N (standard deviation, 30 N/30 %) with 95 % power and alpha equal to 0.05. MINITAB 15 statistical software was utilized. The statistical methods applied were ANOVA with a Bonferroni post hoc analysis. Statistical significance was set at p=0.05.
Results
Intact metacarpals in group 1 were tested in apex dorsal three-point bending to failure to establish the native strength of cadaver metacarpals. A force displacement curve was created for each metacarpal showing peak load to failure (Fig. 5). The average load to failure for intact metacarpals was 1,152.3±520.7 N and the stiffness was 1,130.3±479.6 N/mm.
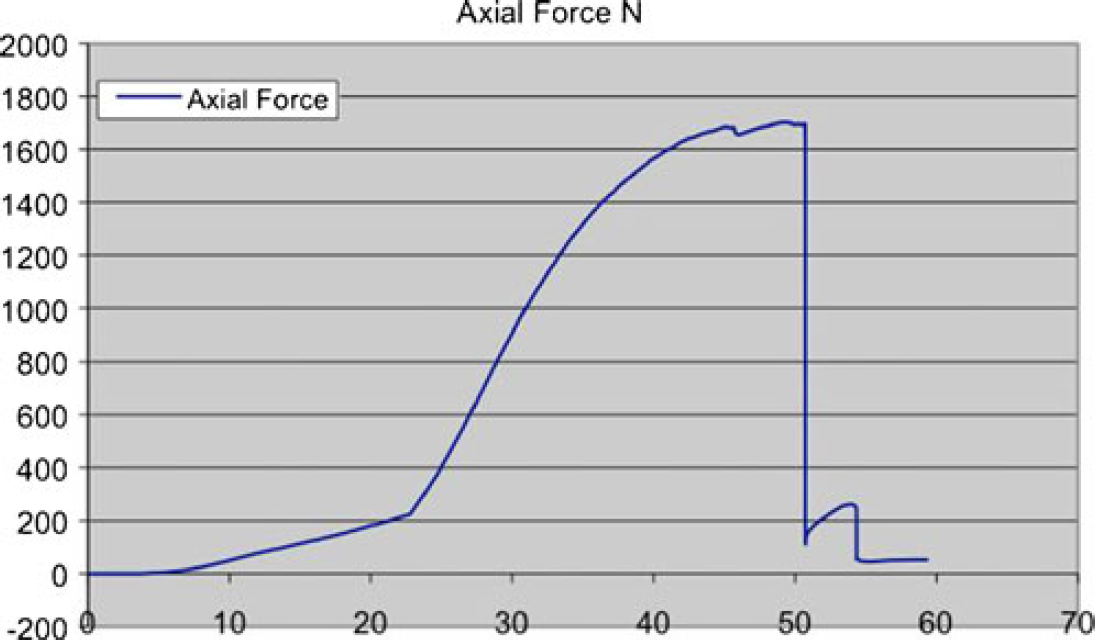
Force/displacement curve of group 1 (intact metacarpal). Peak load is the apex of the curve, and stiffness is derived from the slope of the curve
In group 2, the five metacarpals from one hand had standard sized corticotomies created (1.0 cm×0.6 cm) as previously described. These voids were left unfilled. The two other hands in group 2 had corticotomies filled with bovine demineralized bone matrix. All 15 of these metacarpals were taken together as a negative control group. The negative controls had diminished load to failure compared with the intact samples, with an average ultimate load to failure of 803.3 ± 352.8 N. The stiffness of the negative controls was 828.0 ± 344.7 N/mm. When the ten metacarpals treated with bovine demineralized bone matrix were compared to the corticotomy alone samples in a subgroup analysis, there was no difference in peak load (p=0.199). Intact samples were statistically significantly stronger than the negative control samples taken as a whole (p=0.04).
In groups 3 and 4, carbonated apatite and hydroxyapatite, respectively, there was an increase in peak load and stiffness over the negative controls. The peak load to failure for carbonated apatite calcium phosphate cement-treated samples on average increased to 1,496.5±542.8 N, and stiffness increased to 1,289±329.1 N/mm. Hydroxyapatite calcium phosphate cement treatment increased the peak load to failure to 946.0±476.4 N and stiffness to 1,000.7±408.8 N/mm. Hydroxyapatite-filled voids tended to be stronger than the negative controls, but this did not reach significance (p=0.359). Carbonated apatite samples in group 3, however, biomechanically exceeded the strength of the negative control samples (p=0) and were also statistically significantly stronger than the hydroxyapatite samples from group 4 (p=0.006) (Fig. 6).
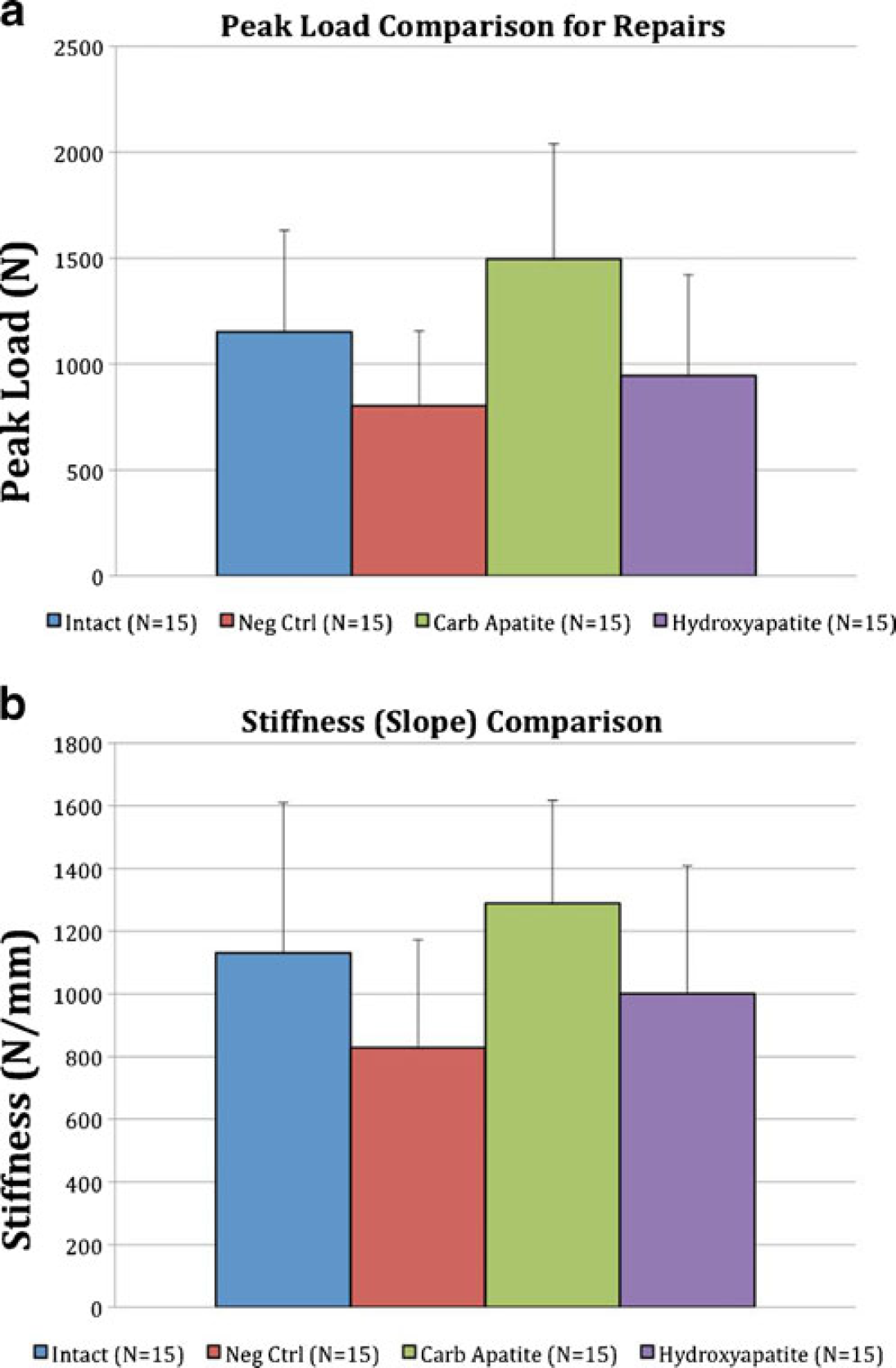
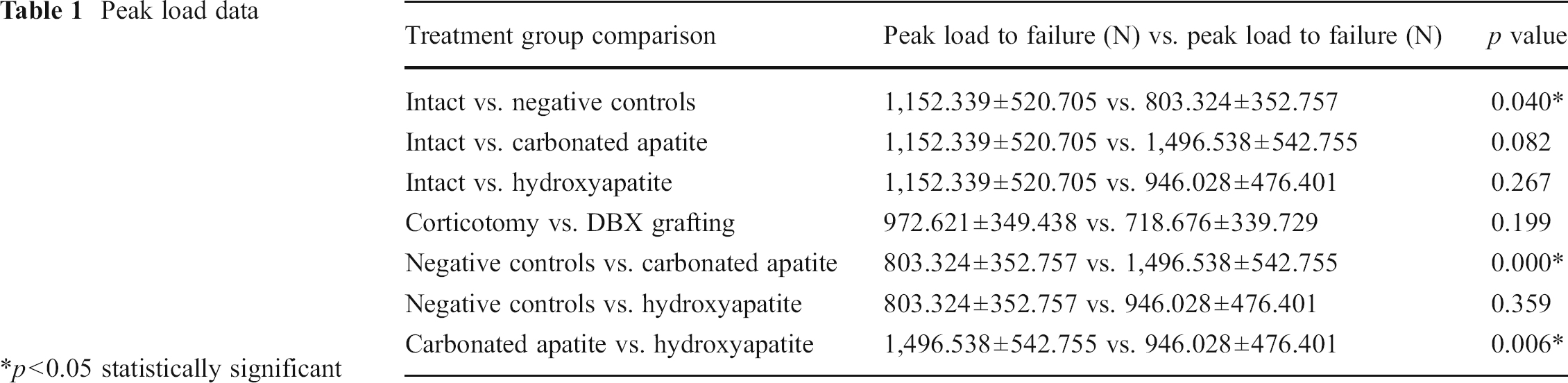
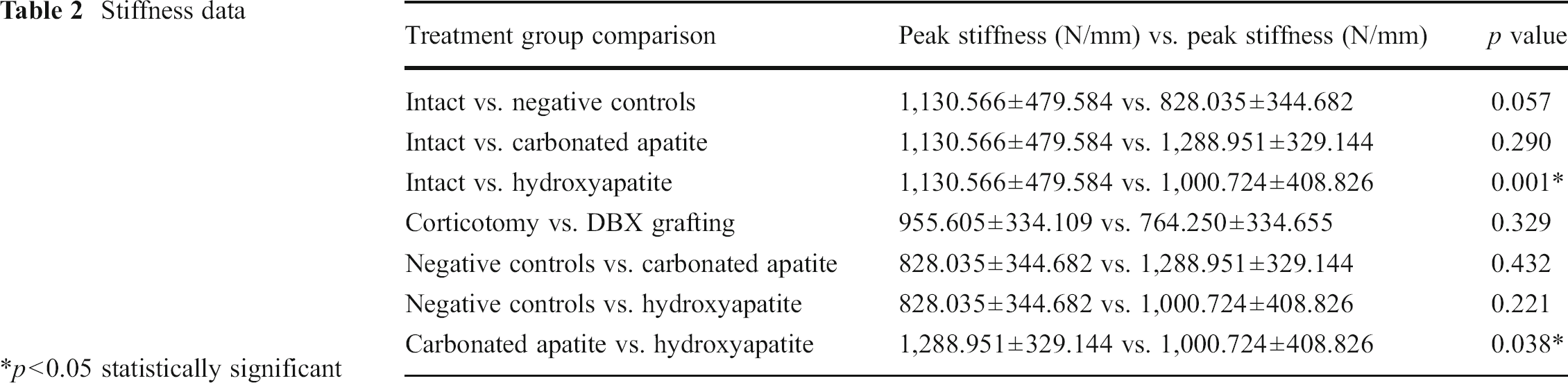
Peak load data (Table 1) revealed that intact metacarpals as well as metacarpals treated with carbonated apatite calcium phosphate bone cement are statistically significantly stronger than the negative controls in group 2. Interestingly, the carbonated apatite samples from group 3 were also found to be statistically significantly stronger for peak load than the hydroxyapatite calcium phosphate bone cement samples in group 4. Stiffness data (Table 2) revealed that the intact samples trended towards being stiffer than the negative controls, but did not meet statistical significance (p=0.057). The carbonated apatite-treated metacarpals, however, are significantly stiffer than the negative controls (p=0.001) and the hydroxyapatite-treated metacarpals (p=0.038).
Peak load data
p<0.05 statistically significant
Stiffness data
p<0.05 statistically significant
Discussion
This is the first study to describe and biomechanically test a cadaveric model of enchondromas of the hand. The study demonstrated that the intact metacarpal is significantly weakened by creating a corticotomy and bone void, whether or not the void is filled with demineralized bone matrix allograft. Treating an enchondroma of the hand with simple curettage with or without bone grafting biomechanically weakens the bone to nearly 70 % the strength of an intact bone, making it more susceptible to fracture. Based on this finding with demineralized bone matrix, it is inferred that cancellous bone grafting, whether autogenous or allogenic, likely does not confer any biomechanical strength to a hand enchondroma until time has passed for healing to occur. Therefore, no immediate biomechanical increase in stability is achieved. Healing and bone graft incorporation must occur before mechanical stability can be restored to that of native bone and thus postoperative immobilization may be wise.
Adding the support of a biologic calcium phosphate cement increases the strength of simulated hand enchondroma samples over that of the negative controls, and the carbonated apatite samples reached statistical significance. This finding indicates that in a hand enchondroma model where carbonated apatite calcium phosphate bone cement is used as a bone void filler, the metacarpals are stronger when subjected to bending than those treated with curettage alone and nearly as strong as intact metacarpals. In our study, carbonated apatite bone cement demonstrated superior biomechanical properties to hydroxyapatite calcium phosphate. However, in clinical practice, the additional strength may not provide any added benefit. The increased strength provided by both calcium phosphate cements may be sufficient to allow for early postoperative digital range of motion.
There are several criticisms that could arise in regard to this study. First, the corticotomy model does not show the typical cortical expansion seen in hand enchondromas. As this is a biological process of remodeling that occurs in the body over an extended amount of time, there is no way to accurately replicate this using a cadaver model. Second, hand enchondromas typically occur in the proximal phalanges and ulnar metacarpals [9]. In this study, all metacarpals, not just the ulnar metacarpals, were used for testing, but proximal phalanges were not studied. Third, the average cadaver age was 55 years at the time of death, which is older than the average approximately 30-year-old patient with a symptomatic hand enchondroma. To address cadaver age and possible detrimental effects of aging on the bones used in this study, we attempted to determine bone density with a DEXA scan. Unfortunately, limitation in the institution's DEXA machine prevented bone mineral density analysis of such small bones. In addition, while the corticotomy size was standardized by measurement with a digital caliper, the volumetric capacity of the voids was not calculated. Bone voids were, however, handpacked by one person in order to standardize the force of packing. Radiographs were also taken of both the carbonated apatite and the hydroxyapatite-packed samples to provide two-dimensional imaging of the packing material.
Finally, this model strictly looks at three-point bending to failure. It is important to note that biologic cements are strongest in compression. In the real world, fingers are subjected to forces in multiple planes. Therefore, it could be hypothesized that other forces may show inferior loads to failure if tested. However, this may be difficult to replicate biomechanically. Therefore, additional studies evaluating other loads to failure such as torsion may provide further incite into improving clinical outcomes for patients with enchondromas of the digits.
In conclusion, this study biomechanically evaluated the strengths of different fillers commonly used after curettage of hand enchondromas. Standard treatment of hand enchondromas with curettage and bone grafting through a corticotomy window leaves the metacarpal biomechanically weakened in the immediate postoperative period and therefore potentially in need of the external support of a splint or cast until healing has occurred. Filling the void after curettage of a hand enchondroma with calcium phosphate bone cement biomechanically increases the strength of the affected metacarpal to nearly that of an intact metacarpal, suggesting that this technique may allow for earlier unrestricted digital motion after curettage. A future trial comparing different techniques for treating hand enchondromas would be necessary to determine whether biologic cements offer any significant clinical advantage over autografts or allografts with respect to postoperative motion, return to work, or patient satisfaction.
Footnotes
The authors declare no conflicts of interest, commercial associations, or intent of financial gain regarding this research.