
Abstract
Background
Penetrating injuries to the hand are a common occurrence in the emergency room, and embedment of foreign bodies is suspected in many of these cases. The existing literature offers little information on retained foreign bodies. The aim of this study was to identify characteristics, determine prevalence, and observe outcomes for retained foreign bodies in the wrist and hand.
Methods
Four hundred thirty-seven consecutive hand and wrist radiographs in 437 patients from the emergency department of a level 1 trauma center were reviewed for the presence of retained foreign bodies. Location, size, number, and type of foreign body were recorded. Patient demographics, mechanism of injury, associated injuries, and treatment were obtained from medical records. All subsequent hospital and outpatient encounters were reviewed. Follow-up period was 18 months (range, 1–40).
Results
Of 437 cases, 65 patients (15 %) had at least one retained foreign body. Nineteen patients underwent removal of foreign body at initial presentation. The average size of foreign bodies removed was 6 mm, compared to 3 mm for those retained. Of 46 patients where the foreign body was left in situ, two (4 %) developed symptoms directly related to the retained foreign body. One of these patients underwent removal.
Conclusions
This study supports the safe removal of foreign bodies which are easily accessible or when part of a broader procedure to repair injured structures. Otherwise, we advocate expectant management for all other patients, as the likelihood of persistent symptoms is low and only 2 % of retained foreign bodies required removal later.
Keywords
Background
More than 11 million patients are seen annually in US emergency departments for traumatic wounds and lacerations [6]. Nearly one third of these wounds involve the fingers, hand, or wrist. Additionally, a retained foreign body (FB) is present or strongly suspected in over 10 % of the cases [11]. Some foreign bodies are easy to detect or result in direct injury to vital structures, whereas others can remain asymptomatic and go unnoticed. The failure to treat or diagnose retained foreign bodies in the hand is among the top ten claims for most malpractice carriers, resulting in the fifth highest amount of indemnity awards to patients [12]. The management of these foreign bodies continues to be a matter of debate and without a consensus regarding their treatment.
The existing literature offers little information on the characteristics or prevalence of retained foreign bodies in the wrist and hand. Furthermore, there are no outcome data on patients with retained foreign bodies. The percentage of retained foreign bodies that will cause “problems” down the line is unknown.
In general, current literature states that neurovascular (or potential) injury, tendon laceration, cosmetic deformity, functional impairment, and chronic pain are indications for wound exploration and foreign body removal. Contraindications to removal include deep embedding or inaccessibility, unacceptable iatrogenic risks to neurovascular structures during the retrieval process, minute size, inert material, and asymptomatic presentation [1,14,20]. However, the basis of these recommendations is anecdotal experience and isolated cases reports and not evidenced based.
At our institution, embedded foreign bodies in the wrist and hand are generally treated acutely in the emergency department by removal of those that are easily visible and accessible. Foreign bodies are removed in the operating room only if it is encountered as part of a broader procedure necessitating general anesthesia to repair other injured structures. The purpose of this study is to identify characteristics, determine prevalence and outcomes, and describe the effects of retained foreign bodies in the wrist and hand.
Materials and Methods
We conducted an IRB-approved retrospective chart review of consecutive patients who had hand and/or wrist plain radiographs in the emergency department of an urban, university hospital from January 2009 through January 2010. A hand surgery fellow and an attending radiologist examined the radiographs on Centricity™ PACS-IW (GE Healthcare IT, Little Chalfont, UK) to determine if a foreign body was present. If there was no foreign body identified, then there was no further investigation for that particular patient.
After identification of a foreign body was made on plain radiography, its location, size, quantity, and character of the foreign body were obtained from the radiographs and medical records. Size of the foreign body was measured in its largest dimension on the radiographs. If there were multiple foreign bodies identified, then the size and location of the largest body were noted. Locations were classified according to zones outlined by Verdan et al. [21] for the volar side and Kleinert et al. [13] for the extensor side. An orthopedic surgery resident reviewed the patients' corresponding medical records to document associated injuries, treatment, and complications. The medical records from all subsequent hospital admissions, emergency department, and outpatient encounters were reviewed on the hospital electronic medical record systems (EPIC-Epic Systems Corporation, Verona, WI; Sovera HIM-CGI Group Inc., Montreal, Canada; Centricity Enterprise, GE Healthcare IT, Little Chalfont, UK).
Chi-square analysis and Fisher's exact test were used to evaluate any correlation between foreign body removal and any of the aforementioned foreign body characteristics. Statistical significance was set at p≤0.05.
Results
During the study period, there were 437 plain radiograph series of the hand and/or wrist obtained in 437 patients. Of these 437, 65 patients (15 %) presented with at least one embedded foreign body (Table 1). There were 55 males and 10 females with an average age of 38 years (range, 16–88 years). Of the 65 patients with foreign bodies, 19 were lost to follow-up. For the remaining 46 patients, follow-up period averaged 18 months (range, 1–40).
Demographic information of patients with foreign bodies of the wrist or hand
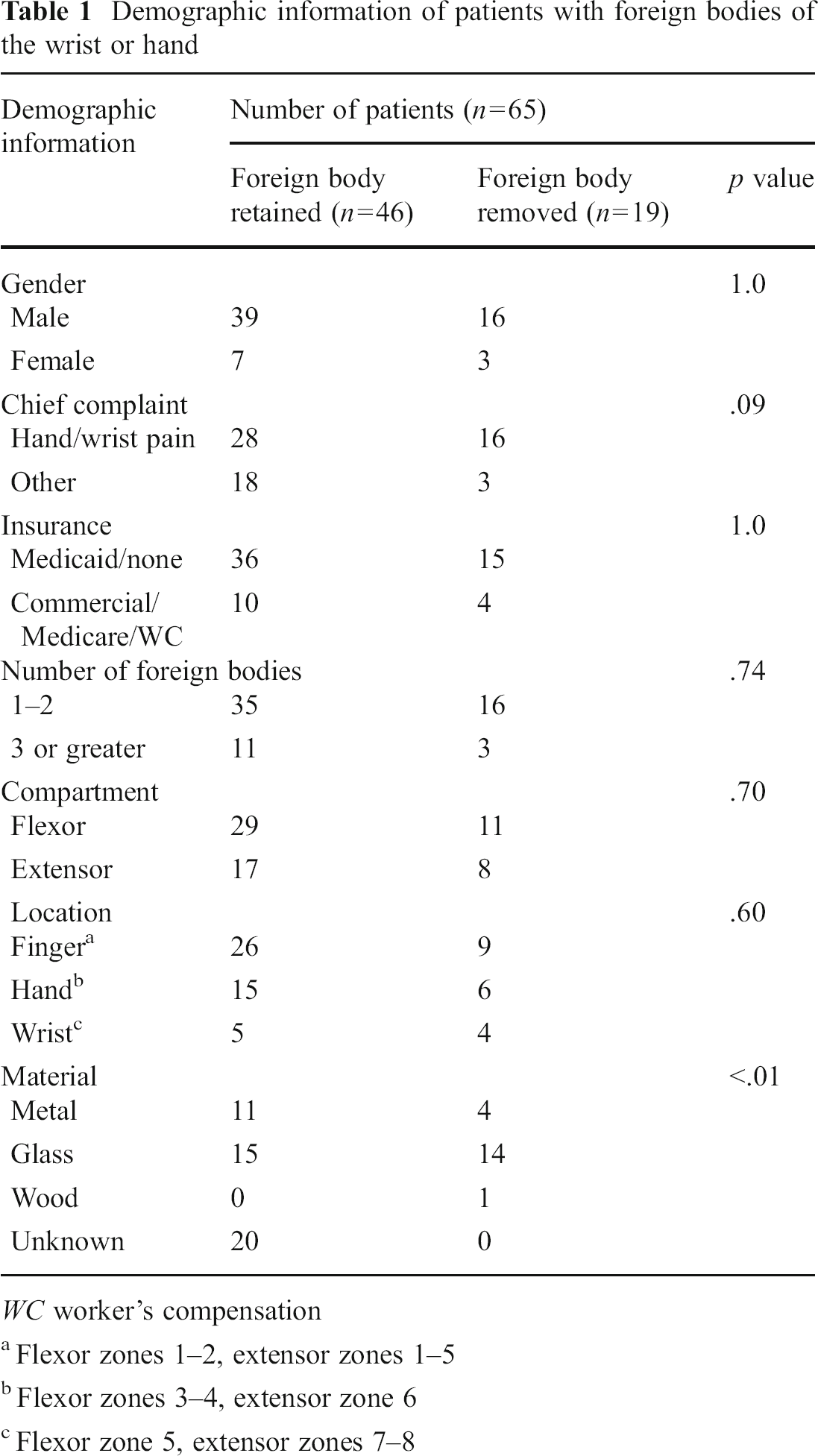
WC worker's compensation
Flexor zones 1–2, extensor zones 1–5
Flexor zones 3–4, extensor zone 6
Flexor zone 5, extensor zones 7–8
As demonstrated in Table 2, 19 of the 65 (29 %) patients who were diagnosed with foreign body embedment underwent removal of the foreign body at the time of initial presentation. Fifteen patients had their foreign body removed in the emergency department; 14 under local anesthetic and 1 under conscious sedation. Four patients had foreign bodies removed in the operating room. All four had concomitant injury to the limb requiring operative repair, and the foreign body removal was a secondary procedure. The most common material removed was glass (14), followed by metal (4) and wood (1) (p<.01). There was a significant difference between the size of foreign bodies removed versus those left in situ, 6±5 mm (range, 1–23 mm) vs. 3±4 mm (range, 1–22 mm), respectively (p=.03).
Characteristics of patients undergoing removal of foreign bodies at time of initial presentation
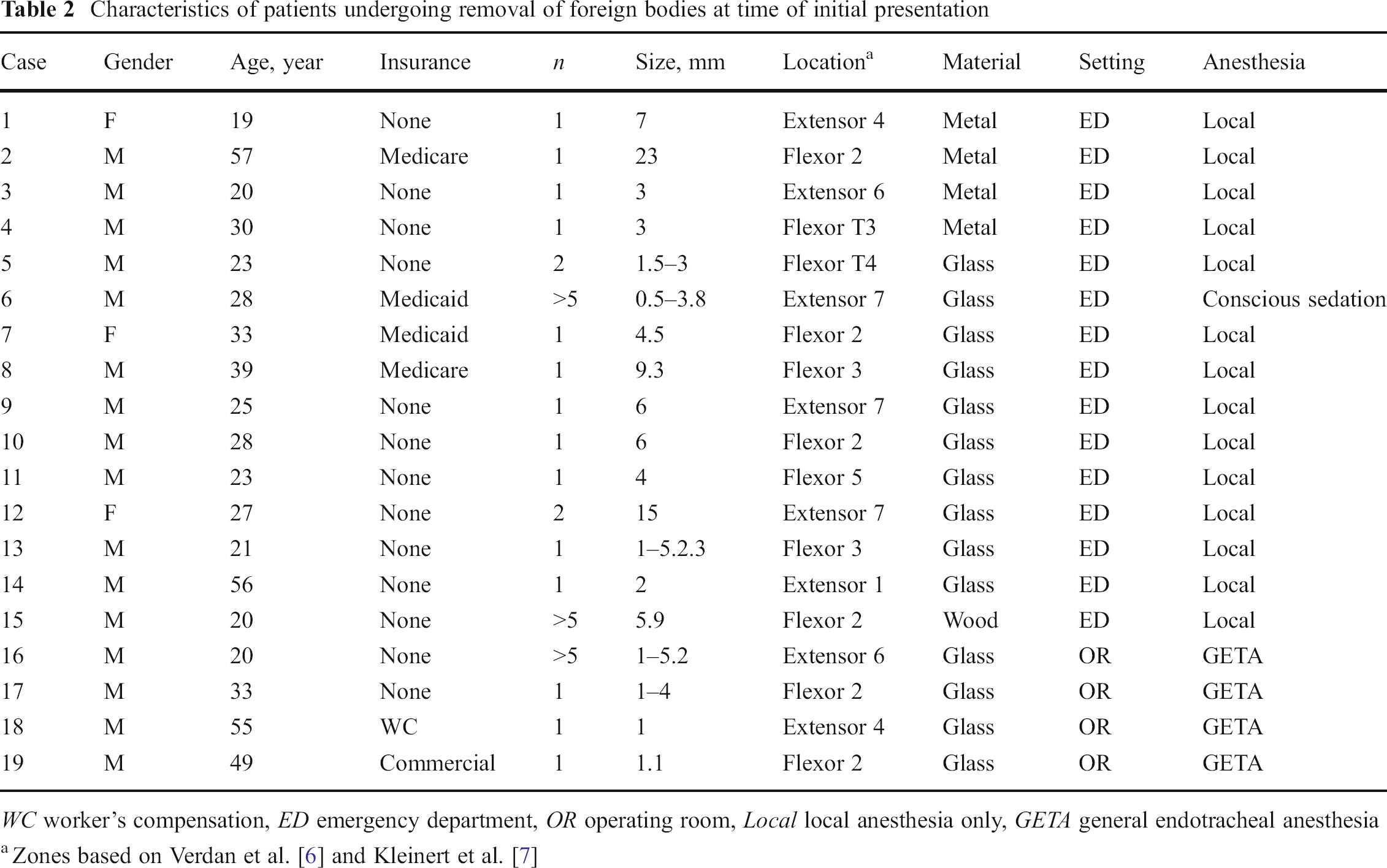
WC worker's compensation, ED emergency department, OR operating room, Local local anesthesia only, GETA general endotracheal anesthesia
In the 46 patients in whom a FB was left in situ, two (4 %) patients reported symptoms due to the presence of the retained foreign body. One patient presented with localized pain and swelling from an injury sustained approximately 8 weeks prior to initial presentation. The 3-mm foreign body was in the web space between the ring and small finger on the volar aspect of the hand. This patient received symptomatic treatment. At the most recent follow-up at 33 months, the patient had no hand-related complaints. The other patient presented with ulnar sided hand pain and limited small finger range-of-motion 2 months after the initial injury. This patient went to the operating room for an elective removal of a 3-mm piece of glass at the base of her fifth proximal phalanx 95 days following the initial embedment.
Fourteen patients presented with more than two discrete foreign bodies. Three of these patients had their foreign bodies removed. Two of these three patients went to the operating room for complex wound closure as the primary procedure and had concomitant foreign body removal in the same setting. The third patient had FB removal done under conscious sedation in the emergency department.
The fingers were the most common location for the presence of foreign bodies, followed by the hand, then wrist. Table 3 shows that nearly half (4/9) of the patients with foreign bodies present in the wrist had them removed. Forty patients (61.5 %) had retained foreign bodies in the flexor compartment of the hand or wrist, and 11 patients underwent removal.
Distribution of foreign bodies in the wrist or hand by location
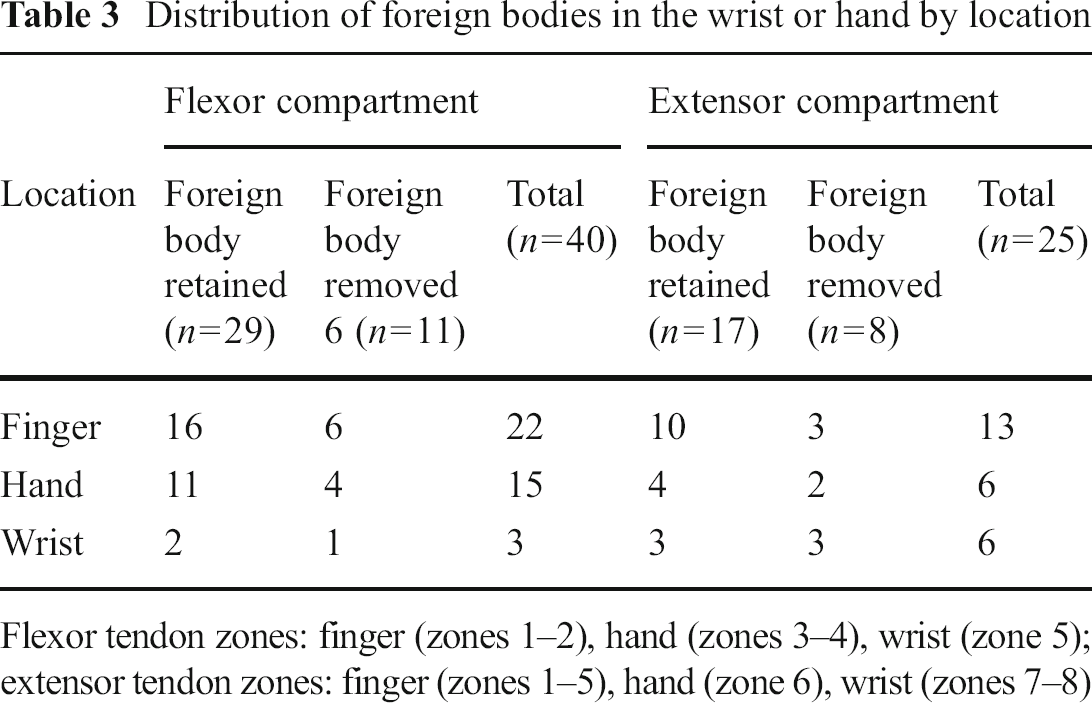
Flexor tendon zones: finger (zones 1–2), hand (zones 3–4), wrist (zone 5); extensor tendon zones: finger (zones 1–5), hand (zone 6), wrist (zones 7–8)
Discussion
While there have been many case reports documenting complications due to a retained foreign body in the extremity [3,7,10,16,22,23], there have not been any noteworthy longitudinal studies examining a larger cohort of patients. Because case reports are inherently biased toward abnormal outcomes, we believe that there is an over magnification and emphasis on complications from foreign body embedment in the wrist and hand in the literature. Our objective was to determine outcomes of this injury pattern in a cross section of the population in order to gain a better understanding of the magnitude of complications associated with retained foreign bodies.
In the present study, we showed that 15 % of all emergency room patients with hand or wrist radiographs had at least one foreign body present. Although this is a relatively high prevalence of foreign body in the wrist and hand, we found a rather low risk of complications (4 %) from foreign bodies left in situ. Furthermore, only one patient (2 %) in our studied population required delayed removal of the retained foreign body due persistent symptoms.
Another interesting finding of the present study is that just 29 % of patients underwent foreign body removal at the initial presentation. Similar to other studies, the vast majority of FB removal in our population was performed in the emergency room under local anesthesia [2,18–20]. Although not specifically stated in the medical records, the presumption is that foreign bodies removed in the emergency room are more accessible or superficially embedded and hence posed a lower risk to the patient. Although one of our a priori hypotheses was that removal of superficial foreign bodies is more common, we were unable to provide objective data because of the limitations in using plain radiographs only for imaging. Computed tomography or magnetic resonance imaging would have allowed a more accurate measurement of the FB from the surface of the skin; however, these imaging modalities were not routinely employed for our patients. In general, however, the literature shows strong support for radiographic detection of glass and metal foreign bodies, albeit with wooden and gravel foreign bodies detected at lower rates [1,5,15,17]. Glass foreign bodies larger than 2 mm in size have a nearly 100 % detection rate, and fragments between 0.5 and 2 mm have slightly limited detection ability [4].
Our analysis showed a statistically significant association between foreign body size or material and its removal. Removed foreign bodies were generally larger; however, there was a wide range in size for those removed and retained. The association between the foreign body material and the necessity for removal is one documented in the literature. Prior studies have shown a higher likelihood for complications with glass or wood foreign bodies [8,9,19]. However, in this series, there was only 1 of 15 patients with a retained glass foreign body who required removal at a later time.
Taken together, the present study supports immediate removal of wrist and hand foreign bodies if it can be done readily (and safely) in the emergency room or when associated injuries necessitate a trip to the operating room. The treatment of retained foreign bodies remains a multifactorial challenge in which the clinician must evaluate the mechanism of injury, character of wound, and risks of foreign body removal when making a decision in treatment. However, we observed that a FB left in situ poses minimal risk to surrounding soft tissues and neurovascular structures.
The limitations of our study include its retrospective nature. Furthermore, since the study was conducted at a single institution, the patient demographics may not reflect the general population. Additionally, some patients from this series may not have followed up at our institution, affecting the longer term outcomes. However, given our patient demographics and insurance status (Table 1), it is highly unlikely that they would have presented elsewhere for follow-up since we are the only institution in the greater metropolis area to accept uninsured or underinsured patients. Finally, we have only been able to follow these patients on average for 18 months, and it is possible that with longer follow-up, more patients with retained foreign bodies could present with symptoms.
Footnotes
Acknowledgments
The authors declare that they have no conflict of interest with the subject of this report.
The authors declare that they have no conflict of interest.