
Abstract
Purpose
In traditional flexor tendon repairs, suture knots can be sites of weakness, impair tendon healing, stimulate an inflammatory response, and increase the bulk of the tendon repair. Because of this, there has been an increased interest in knotless flexor tendon repair using barbed suture. Since knots are not required, it may be possible to increase the strength of the tendon repair by using a large-diameter barbed suture. The purpose of this study was to biomechanically compare a traditional four-strand tendon repair using 3–0 braided polyester with a similar knotless four-strand tendon repair using 0 unidirectional barbed suture.
Methods
Twenty-two matched cadaveric flexor digitorum profundus tendons were lacerated and assigned to repair by a four-strand modified Kirchmayr–Kessler technique using 3–0 braided polyester (n=11) or knotless four-strand modified Kirchmayr–Kessler repair using 0 unidirectional barbed suture (n=11). Repaired tendons were linearly distracted to failure at 20 mm/min after 1 N preload. Maximum load and load at 2-mm gap formation were recorded. Maximum load and load at 2-mm gap formation were compared with the Student's t test, and p values≤0.05 were considered significant.
Results
The mean maximum load of the barbed, knotless suture repair was higher than that of the traditional repair (52 vs. 42 N). There was no difference between the two groups in the mean load required to produce a 2-mm gap.
Conclusions
The four-strand knotless tendon repairs using a large-diameter unidirectional barbed suture were stronger than the traditional four-strand repairs using 3-0 braided polyester, and had similar 2-mm gap resistance.
Introduction
As techniques in flexor tendon repair have advanced, the merits of early mobilization, reduction of bulk at the repair site, and minimization of gapping have been established [1–8]. Many different suture repair techniques exist, but all require the placement of one or more knots located within or external to the tendon repair site [9–12]. However, knots are a site of weakness and may rupture or unravel [13, 14]. When located within the tendon repair site, knots may impede tendon healing, stimulate an inflammatory response, impede vascularization, and hinder gliding by increasing tendon cross-sectional area. Knots that are located external to the repair can impair gliding within the flexor tendon sheath, and are a potential nidus for adhesion formation [8–10, 13–18].
Because of the problems associated with knots, combined with advances in barbed suture technology, knotless tendon repair using barbed suture has been re-examined in a number of recent studies with mixed results [19–23]. One possible advantage of a knotless repair that has not been examined is the potential to use a suture of substantially larger diameter than would be possible in a traditional repair due to the excessively bulky knots that would be created. It is possible that large-diameter barbed suture can be used to increase the strength of flexor tendon repairs without the use of knots. The purpose of this study was to compare the maximum load of a knotless flexor tendon repair using a large-diameter (0) barbed suture with the maximum load of a traditional four-strand repair using 3-0 suture. Because large-diameter suture is not used in traditional flexor tendon repair, the large-diameter barbed suture was compared to a smaller commonly used suture material in order to maintain clinical relevance. A secondary measurement was load at 2-mm gap formation (gapping resistance). The null hypothesis was that the mean maximum load of two repair techniques would be the same.
Materials and Methods
Twenty-two flexor digitorum profundus (FDP) tendons were harvested from the index, long, ring and small fingers of six paired fresh frozen cadaveric hands. The specimens were harvested after thawing for 24 h at room temperature immediately before the study was performed. In two hands belonging to the same cadaver the FDP tendon of the small finger was hypoplastic and was not used. The entire length of each FDP tendon was harvested, from the musculotendinous junction to the distal insertion. After harvest, each tendon was sharply divided at a point 8 cm proximal to the distal end, approximating a laceration at the junction of Zones II and III. The tendons were assigned to one of two repair groups, using either a traditional four-strand repair (n=11) or knotless four-strand repair with barbed suture (n=11). Traditional repairs were performed on tendons from the left hand, and knotless repairs on tendons fromthe right hand. In order to make a side-by-side comparison of the two repair techniques, each tendon in a matching tendon pair was assigned to a different repair group. For example, in a given cadaver, the left index finger FDP tendon was assigned to the traditional repair group and the contralateral right index finger FDP was assigned to the knotless repair group. Biomechanical testing was performed directly after the repairs were completed. Tendon desiccation was prevented by wrapping the specimens in saline-soaked gauze between repair and biomechanical testing.
Tendon Repair
The traditional four-strand repairs were performed using 3–0 braided polyester (Ethibond, Ethicon Inc., Somerville, NJ). A modified four-strand Kirchmayr–Kessler technique was used, with a single knot located external to the repair site. The longitudinal core sutures were placed in the middle of the tendon substance. The transverse passes were placed 7 and 10 mm from the tendon laceration. The transverse passes were placed superficial to the longitudinal passes. The single knot was made with four square knot throws. An epitendinous suture was not performed.
The knotless four-strand repairs were performed using a 0 diameter absorbable, unidirectional, barbed glycolic–carbonate suture (V-Loc 0, Covidien Inc., Mansfield, MA). A modified four-strand Kirchmayr-Kessler technique as described by Zeplin et al. was used (Fig. 1) [22]. As with the traditional repair, the transverse passes were placed 7 and 10 mm from the tendon laceration, with the transverse passes made superficial to the longitudinal passes. An epitendinous suture was not performed.
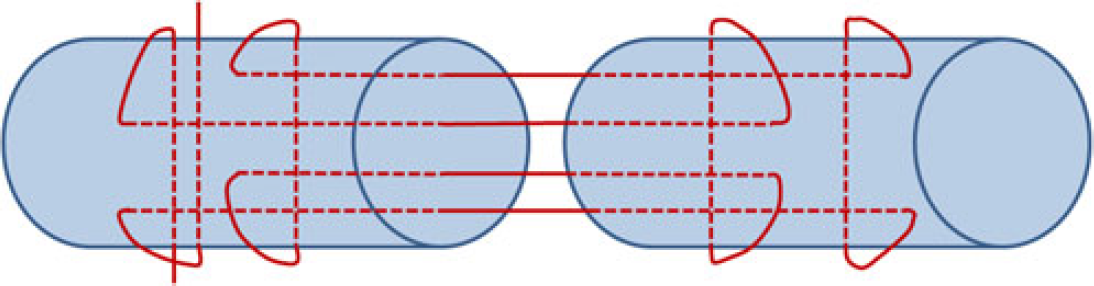
Demonstrates the knotless four-strand modified Kirchmayer–Kessler repair technique used. One end of the suture contains a locked loop, not shown
All repairs were performed by the senior author and two other surgeons. The surgeon who performed a traditional four-strand repair in one tendon also performed the knotless repair on the corresponding digit of that cadaver's contralateral hand.
Biomechanical Testing
Repaired tendons were mounted in the soft tissue clamps of a tensile testing machine (Instron Corp., Norwood, MA). In order to prevent tendon slippage within the clamps, the clamp surfaces were lined with anti-slip tape (3M, St. Paul, MN). A digital micrometer caliper was placed just outside each side of the repair site (14 mm from the laceration) to record gap formation. A 1 N preload was applied to each specimen, followed by distraction at 20 mm/min until failure. The maximum load (in newton) and the load at 2 mm gap formation (in newton) were digitally recorded using a computer software program (Bluehill, Instron Corp., Norwood, MA).
Statistical Analysis
Using data from a pilot study, an a priori power analysis was performed to ensure adequate sample size (G*Power 3.1.3, Heinrich-Heine University, Dusseldorf, Germany). For a power of 0.80, 11 tendons were needed in each group to detect a difference of 10 N in maximum load. The mean maximum load and the mean load at 2-mm gap formation for both groups were compared using a paired Student's t test (SPSS Inc., Chicago, IL). p values≤0.05 were considered statistically significant.
Results
The mean maximum load and the mean load at 2 mm gap formation for the traditional and knotless repair groups are shown in Fig. 2. The maximum load for the knotless repairs (52.3 ± 2.5 N) was higher than the maximum load for the traditional repairs (42.3 ± 2.7 N; p=0.01). There was no significant difference in the average load required to produce 2-mm gap formation for the knotless (10.9 ± 2.8 N) and traditional repair groups (11.7 ± 2.5 N; p=0.62).
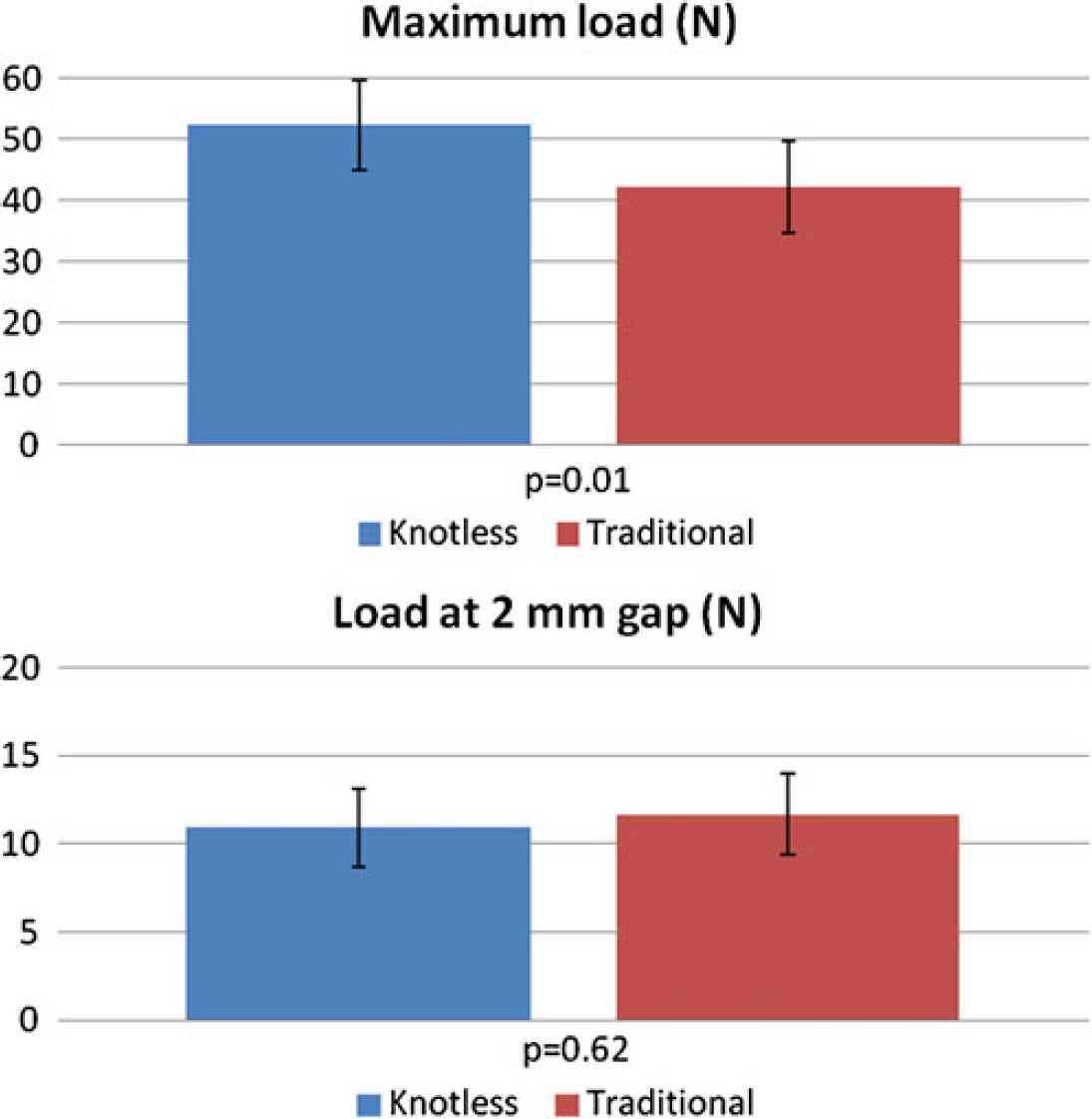
The maximum load (in newton) and load at 2 mm gap formation (in newton) are shown for the two repair groups. Error bars represent the 95 % confidence interval
Discussion
The idea of using barbed suture or barbed devices in flexor tendon repair is not new [24]. Between 1945 and 1968 at least four specialized barbed sutures or devices were described, but none was widely adopted [25–33]. There are two currently available barbed sutures, which are differentiated by the directionality of their barbs. One is a bi-directional barbed suture made of monofilament polypropylene (Quill, Angiotech Pharmaceuticals, Inc., Vancouver, BC). The suture has a curved needle on each end, and a central non-barbed segment that divides the suture into two halves. Each half of the suture has a spiral of barbs that point away from the needle, resulting in barbs pointing in one direction on one half of the suture, and barbs pointing in the opposite direction on the other half of the suture. This configuration allows one half of the suture to resist pull-out in one direction, and the other half to resist pull-out in the opposite direction. The other available barbed suture is unidirectional and is made of glycolic–carbonate (V-Loc, Covidien, Mansfield, MA). This suture has a curved needle on one end, and a small loop on the opposite end used for locking the starting point. The entire length of the suture has unidirectional barbs pointing away from the needle. With this configuration, the barbs resist pull-out in one direction, and the locked loop prevents pull-out in the other direction. It should be noted that barbed suture is inherently weaker than non-barbed suture of the same diameter, and the tensile strength of barbed sutures is generally comparable to that of non-barbed suture one or two sizes smaller [19].
To date, four studies have compared the biomechanical performance of knotless flexor tendon repairs using ***bidirectional barbed suture (Quill™) with that of traditional flexor tendon repair techniques. There are substantial differences between these studies, including variability in the diameter of the conventional and barbed sutures used, the types of traditional repairs used, and whether human cadaveric or porcine flexor tendon models were used. Furthermore, each of the studies used a different and novel suture configuration for the knotless repair [19–21, 23]. Because of this, it is difficult to summarize the findings of these studies. However, taken together, they demonstrate that bi-directional barbed suture can be used to create knotless flexor tendon repairs with at least equivalent maximum tensile load and 2-mm gapping resistance. The studies also suggest that when barbed suture is used, greater than two strands are required to achieve an equivalent strength to a traditional repair; all of the studies that compared traditional and knotless two-strand repairs demonstrated higher maximum tensile loads in the traditional repairs [20, 23]
One study has evaluated unidirectional barbed suture (V-Loc™) for knotless flexor tendon repair. In 2011, Zeplin et al. compared traditional two- and four-strand modified Kirchmayr–Kessler techniques with two- and four-strand knotless Kirchmayr–Kessler techniques in a cadaveric model [22]. The traditional repairs were performed with 3–0 polydioxanone, and the knotless repairs were performed with 3–0 unidirectional barbed suture (V-Loc™). For the two-strand repairs, the traditional technique was stronger than the knotless technique. However, for the four-strand repairs, there was no difference in maximum load when comparing the traditional and knotless repair techniques.
The purpose of the current study was to compare the biomechanical characteristics of a traditional flexor tendon repair technique with those of a knotless flexor tendon repair technique using a very large-diameter unidirectional barbed suture. The results of this study suggest that a large-diameter unidirectional barbed suture can be used to create a knotless flexor tendon repair that has greater tensile strength and equivalent gap resistance when compared to asimilar traditional repair. One limitation of this study is that like those studies described above, a single continuous load to failure, rather than cyclical loading, was used to test the tendon repairs. Another limitation is the technique that was used to measure gap formation. Digital micrometer calipers were placed just outside the repair site, and their displacement was used to measure gap formation. However, this was an indirect measure of gap formation, and likely included deformation and stretch that occurred at the repair site prior to actual gapping, resulting in artificially lower loads at 2-mm gap formation.
In our experience from this study, handling the 0-diameter barbed suture was more difficult than handling the 3–0 braided polyester. In addition, the loop at the end of the barbed suture was large relative to the size of the tendon, and seating it against the tendon with a low profile was technically challenging. This and other characteristics of the barbed suture may affect work of flexion, a variable that was not measured in this study. Work of flexion has been correlated with multiple factors, including suture size [34] and configuration, [35] whether the FDP is repaired or partially resected [36], how the flexor tendon sheath is managed [37, 38], time from injury [39], and the presence of edema [40], or compressive dressings [40]. It is certainly possible that the large diameter of the barbed suture, as well as friction between the exposed barbs or locking loop of the suture and the synovial lining of the flexor tendon sheath could have important effects on work of flexion. This issue warrants further investigation.
One strength of the study was the assignment of opposite repair techniques to matching cadaveric flexor tendon pairs, thereby creating two closely matched repair groups and increasing the validity of the comparison. Another strength is that the traditional and knotless repair techniques were very similar in terms of suture configuration, isolating the difference in the two techniques to the suture material used. In other studies in which barbed and non-barbed sutures are used in different configurations, it is impossible to know how much of the difference in biomechanical characteristics is the result of the repair configuration, and how much is due to the characteristics of the barbed suture itself.
In conclusion, the four-strand knotless Kirchmayr–Kessler repair using large-diameter unidirectional barbed suture resulted in higher maximum load and similar 2-mm gap formation when compared to the traditional four-strand Kirchmayr–Kessler repair using 3–0 braided polyester. Suture handling was more difficult with the large-diameter barbed suture. How knotless flexor tendon repairs using barbed suture perform in a cyclical loading model or in vivo is not known and may warrant further study.
Footnotes
The authors declare that they have no conflict of interest.