
Abstract
Background
This study addresses factors associated with apparent resolution and recurrence of triggering using data from providers with various treatment strategies.
Method
A retrospective review identified 878 adult patients with 1,210 Quinnell grade 2 or 3 trigger fingers that had one or more corticosteroid injections by one of three surgeons between 2001 and 2011. Two surgeons injected dexamethasone, but one had patients return 1 month after injection and was quick to recommend surgery (strategy A) and the other had patients return 2 months after injection, offered another injection or surgery, and followed the patient's preference. One surgeon used triamcinolone, had patients return only if the injection did not work, and waited at least 3 months to offer surgery. Factors associated with apparent resolution and recurrence of triggering were sought in bivariable and multivariable statistical analysis.
Results
Triamcinolone injection was associated with more frequent apparent resolution (83 %), than dexamethasone injection (30 %). Apparent resolution of triggering was also associated with a delayed surgery treatment strategy (B and C) and the affected finger (long and ring fingers were less likely to resolve). Return with triggering after documented or presumed resolution occurred in 188 fingers (33 %) and was associated with triamcinolone injection, index, long and ring finger, and orally treated non-insulin-dependent diabetes mellitus. Strategy A had the lowest initial apparent resolution rate, the highest proportion of patients having surgery, and the lowest final triggering rate of 10 %.
Conclusion
Both treatment strategy and type of corticosteroid determine apparent resolution and recurrence rates.
Background
Corticosteroid injection into the flexor tendon sheath is a common treatment for idiopathic trigger finger. In contrast with other nonoperative treatments such as splinting and nonsteroidal anti-inflammatory drugs, which may only be palliative, there is good evidence that corticosteroid injection can modify the course of the disease [2, 3, 11–13]. Prior studies have demonstrated that one or more corticosteroid injections can definitively resolve triggering in approximately 50 % of patients [2, 10, 12, 14, 16, 19], but the factors associated with resolution are incompletely defined [17].
Recurrence of symptoms is reported in 13 to 56 % [2, 9, 18, 20] of the trigger fingers injected with insoluble and in 11 to 48 % [3, 7, 23] of the digits injected with soluble corticosteroids. It is not entirely clear why there is so much variability in these reports. In our opinion, it is important to distinguish recurrence or persistence of symptoms such as pain and stiffness from the recurrence or persistence of frank triggering. Table 1 gives an overview of characteristics of four corticosteroids commonly used for trigger finger injection.
Commonly used corticosteroids for injection of idiopathic trigger finger and thumb
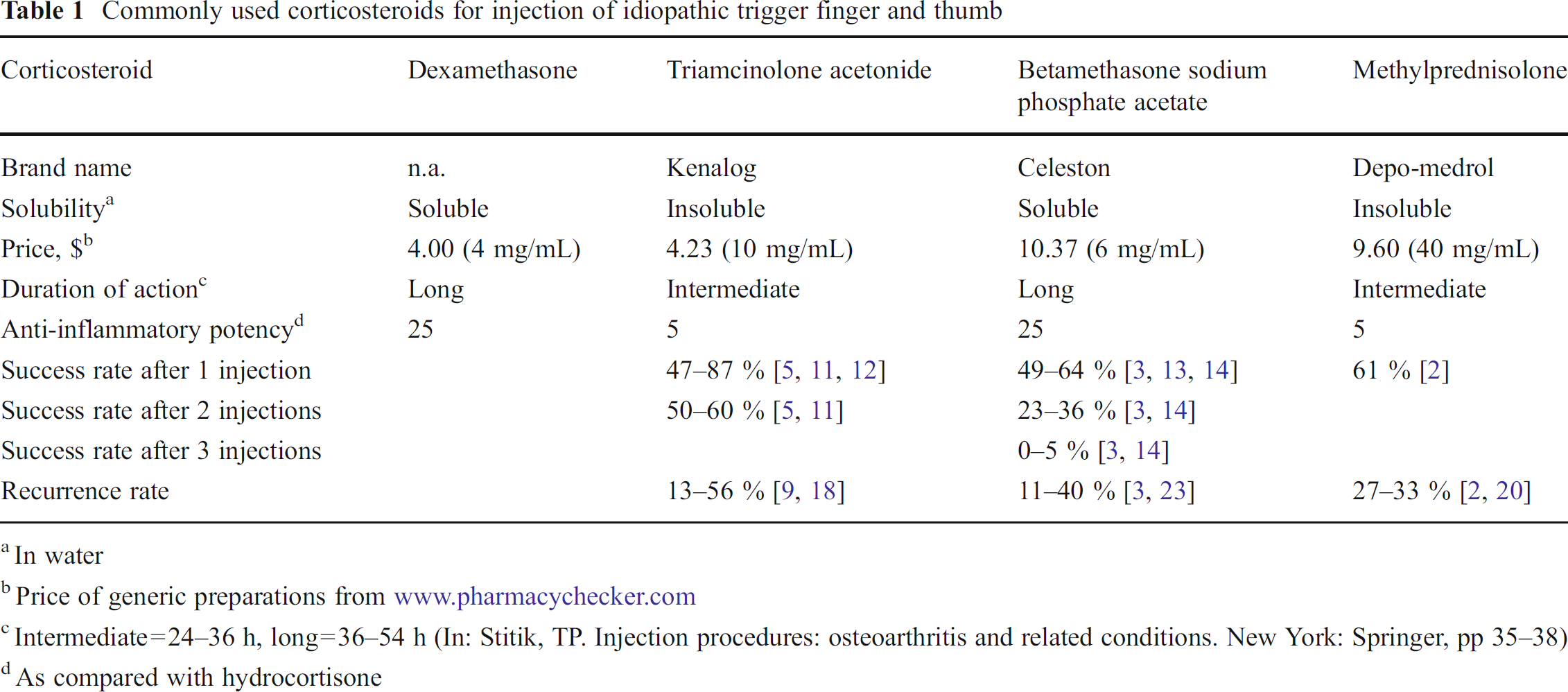
In water
Price of generic preparations from www.pharmacychecker.com
Intermediate=24–36 h, long=36–54 h (In: Stitik, TP. Injection procedures: osteoarthritis and related conditions. New York: Springer, pp 35–38)
As compared with hydrocortisone
The choice of corticosteroid preparation and concentration is a matter of physician preference rather than evidence [1, 17, 18]. Some hand surgeons claim that insoluble steroids are associated with a higher rate of complications [6, 15, 21, 22], while others prefer them because they have a more rapid onset of action [17]. Recommended follow-up (if and when to return) and the decision to offer surgery are sources of variability introduced by the provider.
The purpose of this study was to analyze a large retrospective cohort for factors associated with resolution and recurrence of triggering after one or two initial corticosteroid injections for idiopathic trigger finger. We tested the null hypothesis that resolution of triggering was equal for all three treatment strategies.
Materials and Methods
Patient Selection
Under an institutional review board-approved protocol using billing records, we retrospectively identified 1,491 adult patients who underwent 2,136 corticosteroid injections of one or more trigger fingers between December 17, 2001 and March 16, 2011 at our institution. Fingers were included if they (1) were trigger finger of Quinnell [16] grade 2 or 3 (obvious triggering) and (2) had received dexamethasone or triamcinolone injection. They were excluded if (1) the finger had undergone surgical release in the past or (2) the patients had no or inadequate follow-up. Inadequate follow-up was arbitrarily defined as less than 4 months (121 days) after the first corticosteroid injection with one exception: If resolution of triggering was noted at the patient's last visit, a minimum follow-up of 3 weeks was considered to be sufficient based on our experience.
Of the 2,136 injected fingers, 926 (43 %) were excluded. Surgeon or strategy, age, sex, race, and diabetes mellitus status were comparable between excluded and retained patients. No or inadequate follow-up was side (p<0.001), finger (p=0.011), and steroid (p=0.012) dependent. The cohort for analysis included 1,210 trigger fingers. The demographic overview is shown in Table 2.
Demographic overview of 1,210 injected fingers with real triggering
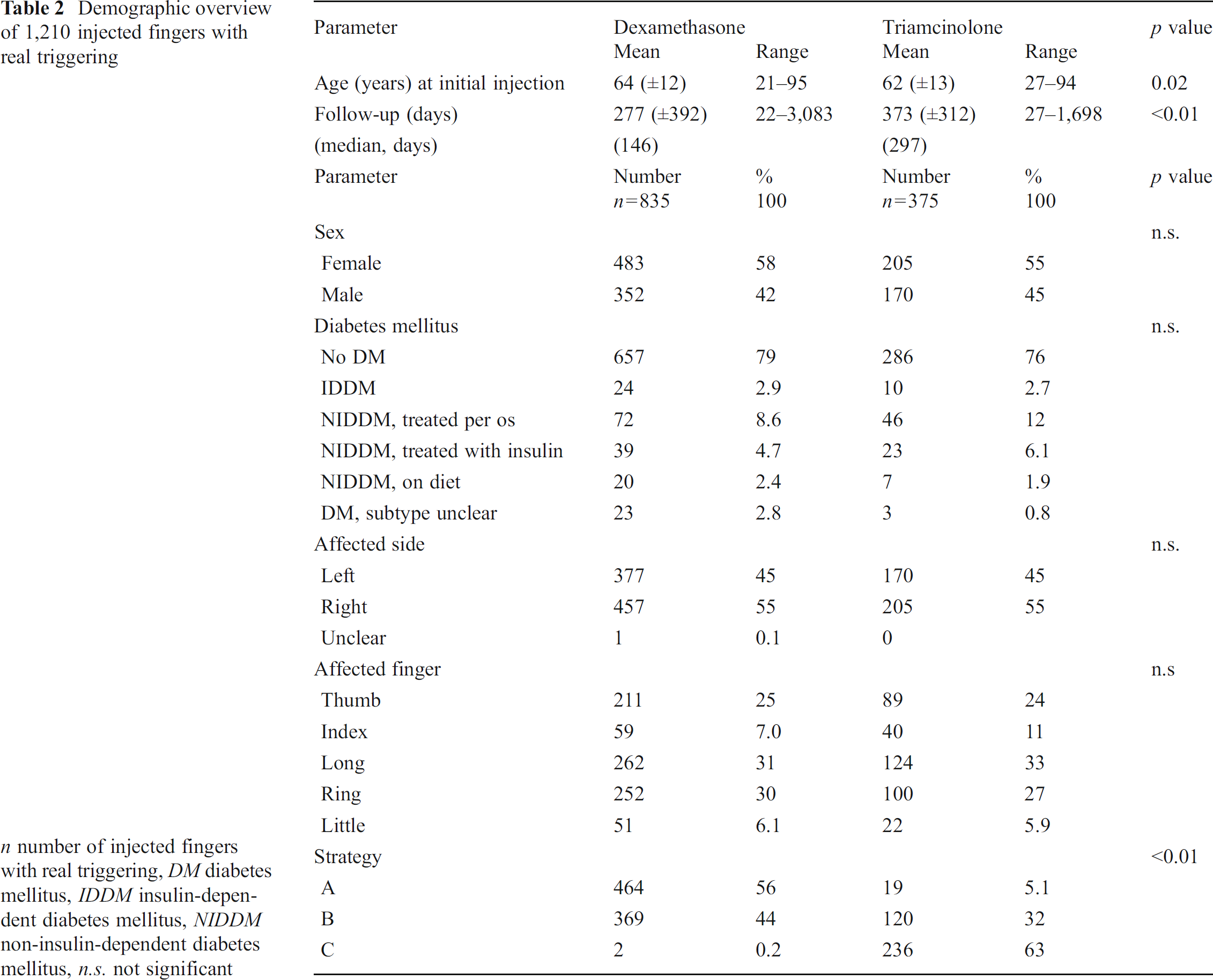
n number of injected fingers with real triggering, DM diabetes mellitus, IDDM insulin-dependent diabetes mellitus, NIDDM non-insulin-dependent diabetes mellitus, n.s. not significant
Three surgeons were involved in the treatment of these patients. Two hand surgeons preferred the use of dexamethasone. Among them, one had patients return 1 month after injection and was quick to recommend surgery (strategy A), and the other had patients return 2 months after injection, offered repeat injection or surgery, and followed the patient's preferences (strategy B). A hand surgeon that used triamcinolone tended to discharge the patient after injection while inviting them to return if there were any problems and waited at least 3 months to offer surgery (strategy C). Open trigger finger release was the surgical treatment in all operative treated patients.
Chart Review and Definitions
Two investigators not involved in the patients' care reviewed medical records retrospectively. The following were recorded: age, sex, race, diabetes mellitus status, affected side and finger, injected corticosteroid (dexamethasone or triamcinolone), number of initial injections per digit (one or two injections into one specific finger within 2 months after the first visit), initial outcome of injections, recurrence and time to recurrence, treating surgeon, time from first injection evaluation, subsequent treatment, and the number of days between the initial steroid injection and surgery where applicable.
The initial result of corticosteroid injection was graded as follows: (1) apparent resolution (documented or presumed resolution) or (2) no resolution or surgery within 4 months. Apparent recurrence was either definite recurrence or presumed recurrence. Definite recurrence was defined as the return of triggering after prior documented resolution of triggering, usually a minimum of 4 to 6 months after the initial injection. One hundred and twelve patients did not return as scheduled after their first injections and therefore had no documentation of initial resolution. However, they returned more than 6 months after injection with triggering. Based on the clinical notes, we presumed they had resolution (retrospectively classified as “presumed resolution”) and recurrence (“presumed recurrence”), but some of these may have been persistent. The final result of the treatment was classified as (1) apparent resolution of triggering or (2) still triggering at last visit documented in the medical record.
Injection Technique
The injections were placed into and around the flexor sheath using a 25- or 27-gauge needle (surgeon's preference) between the distal palmar crease and the proximal digital crease using a 1:1 mixture of 1 % lidocaine (Hospira, Inc., Lake Forest, IL, USA) and either triamcinolone (10 mg/mL; Bristol-Myers, New York, NY, USA) or dexamethasone (4 mg/mL; American Pharmaceutical Partners, Inc., Schaumburg, IL, USA) with a total injection volume of 1.0 to 1.5 mL.
Statistical Analysis
The response variables were apparent resolution of triggering and apparent recurrence of triggering. The explanatory variables were all other data points collected. In bivariate analysis, Pearson chi-square tests and Fisher's exact test (if the expected cell frequency was less than 5) were used to compare two categorical variables, and unpaired T tests or Mann–Whitney U test (if not normally distributed) were used to compare continuous variables. All variables with significant (p<0.05) or near significant (p <0.10) relationships were entered into multivariable binary logistic regression models using the backward conditional method.
Results
Apparent Resolution of Triggering After Injection
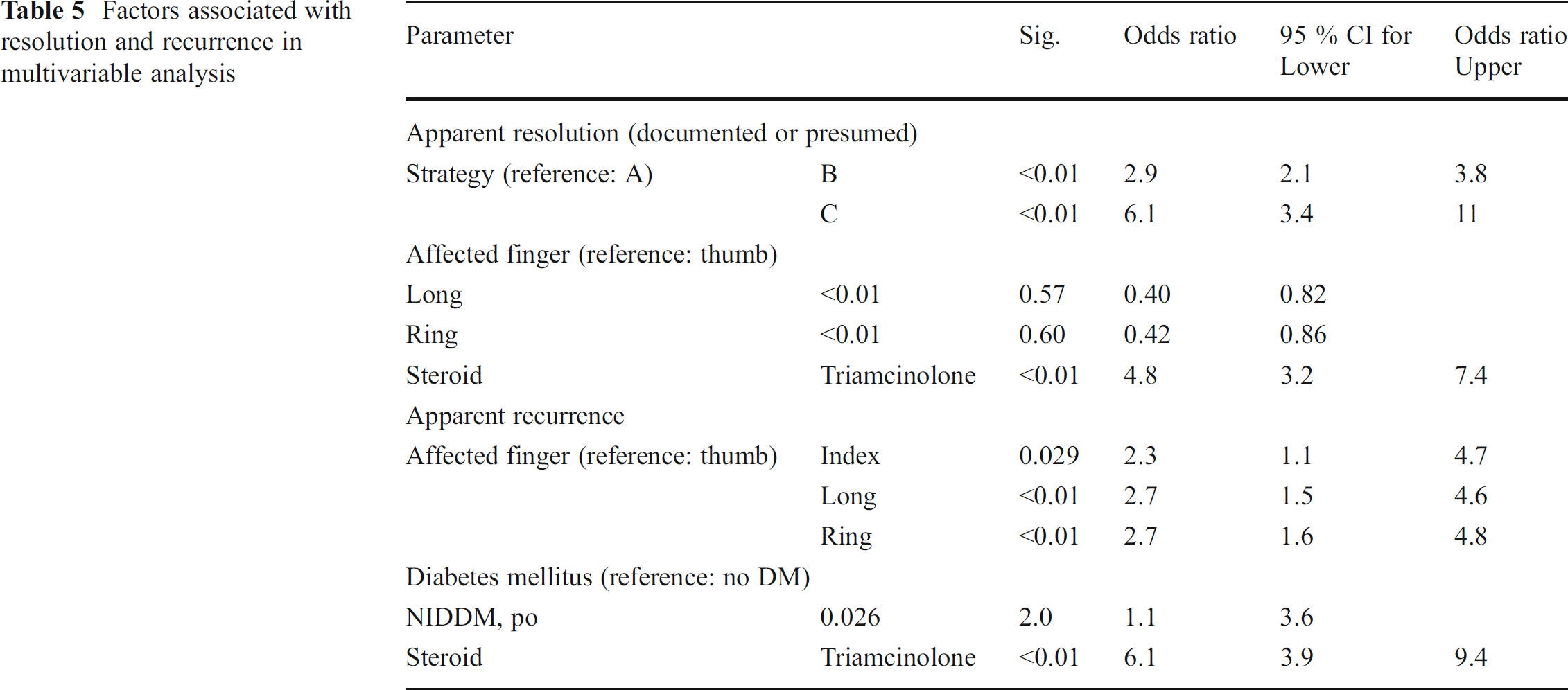
The factors associated with apparent resolution of triggering after injection in bivariate analysis were triamcinolone (83 % compared to 30 % for dexamethasone), the number of initial injections per digit, treatment strategy, and injected finger (Tables 3 and 4). In multivariable analysis, treatment strategies B and C (reference: A) and injection with triamcinolone were identified as independent predictors of apparent resolution of triggering, while long and ring fingers (reference: thumb) were less likely to resolve (Table 5).
Overview of initial results, ordered by steroid, 1,210 injections with adequate follow-up
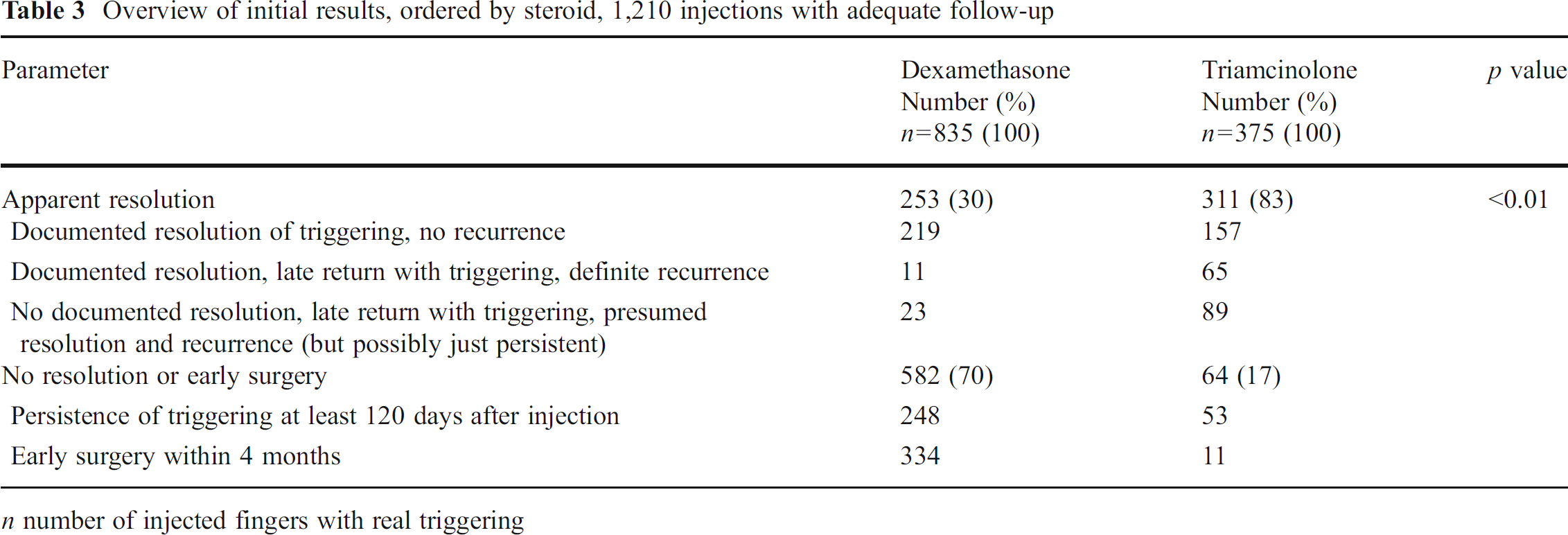
n number of injected fingers with real triggering
Bivariate analysis of apparent resolution
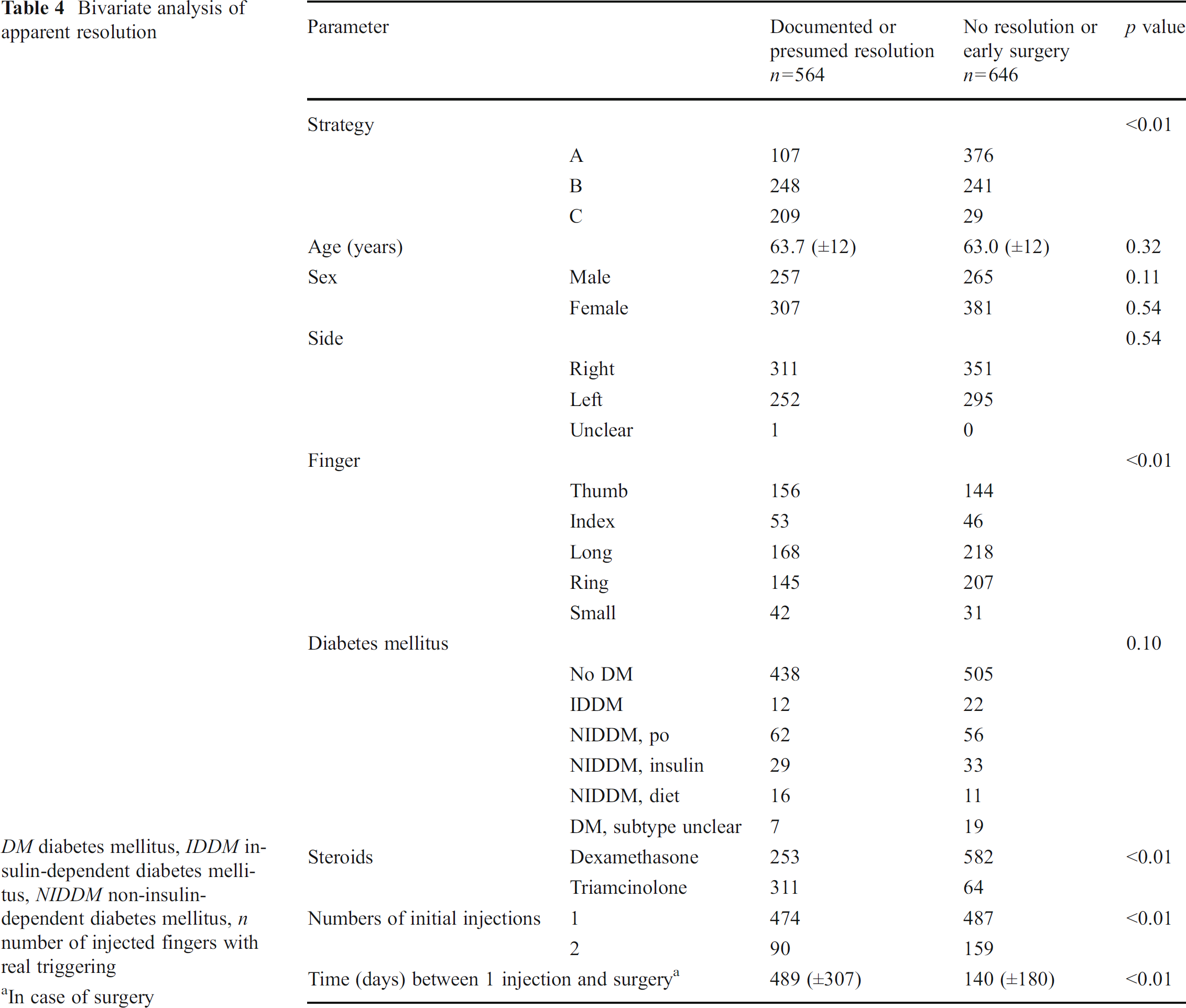
DM diabetes mellitus, IDDM insulin-dependent diabetes mellitus, NIDDM non-insulin-dependent diabetes mellitus, n number of injected fingers with real triggering
In case of surgery
Factors associated with resolution and recurrence in multivariable analysis
Apparent Recurrence of Triggering After Injection
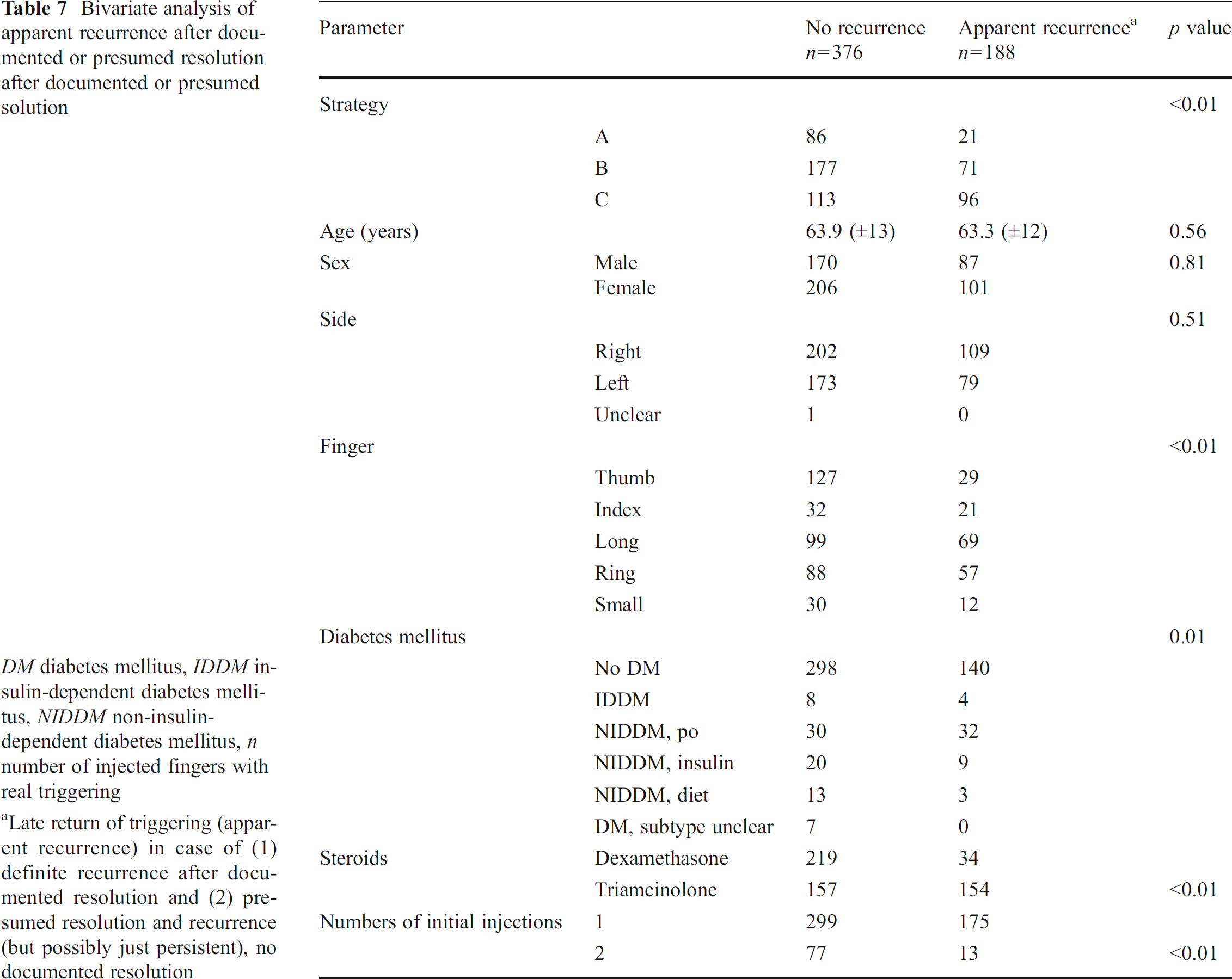
Seventy-six fingers had a documented return of triggering after a documented absence of triggering, and 112 had a presumed recurrence since they had no initial follow-up (Table 6). The mean time to apparent recurrence was 387 days (range, 116 to 2,345 days). Thirty-one patients requested surgery, 128 tried another one to four steroid injections (26 eventually had surgery, 38 had documented resolution, and triggering was persistent or unknown in 64), and 29 had no additional recorded treatment. The apparent recurrence rate was steroid (13 % with dexamethasone vs. 50 % with triamcinolone) and strategy dependent (Table 7). In addition, apparent recurrence of triggering occurred significantly more often in index, long, and ring fingers and patients with orally treated non-insulin-dependent diabetes mellitus (NIDDM) and less often in thumbs and fingers injected twice during the first 2 months (Table 7). In multivariable analysis, injection with triamcinolone, index, long, and ring fingers, orally treated NIDDM, but not treatment strategy were identified as independent predictors of apparent recurrent triggering (Table 5).
Late return with triggering of total 564 resolved trigger fingers

n number of injected fingers with real triggering
Bivariate analysis of apparent recurrence after documented or presumed resolution after documented or presumed solution
DM diabetes mellitus, IDDM insulin-dependent diabetes mellitus, NIDDM non-insulin-dependent diabetes mellitus, n number of injected fingers with real triggering
Late return of triggering (apparent recurrence) in case of (1) definite recurrence after documented resolution and (2) presumed resolution and recurrence (but possibly just persistent), no documented resolution
Final Result in the Medical Record
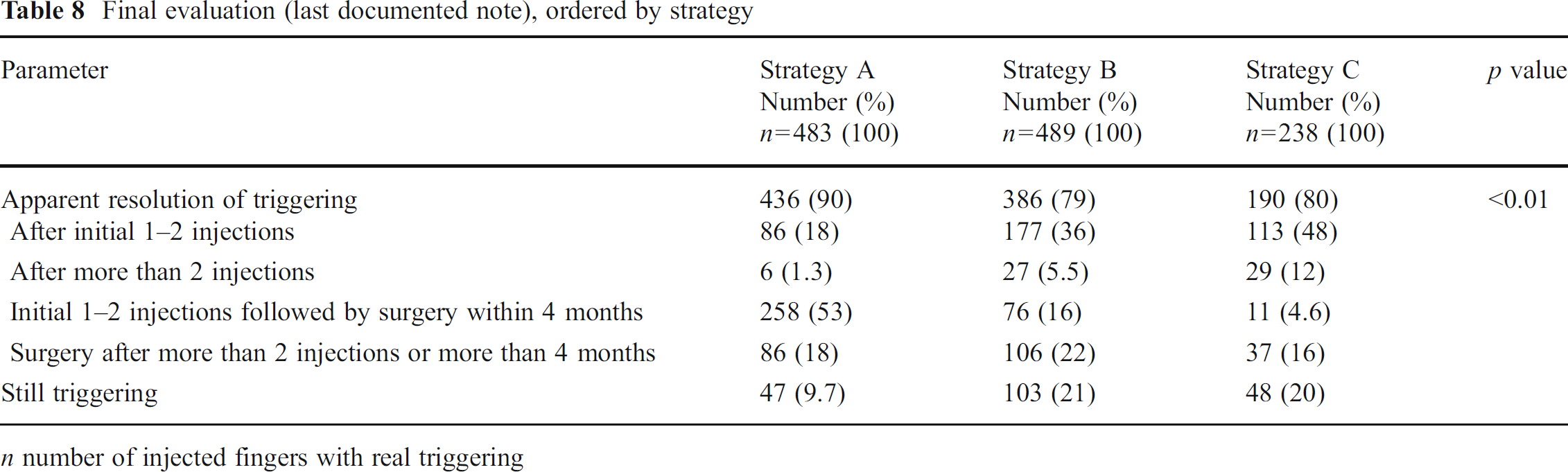
Operative treatment was performed within 4 months in a total of 345 fingers (29 % of all analyzed trigger fingers), whereas in 229 fingers (19 %) a surgical treatment was done later or after more than two injections (Tables 3 and 8). One hundred and fourteen patients (14 %) were still triggering at the last recorded visit in the medical record in the dexamethasone group, compared to 84 (22 %) in the triamcinolone group (p<0.01).
Final evaluation (last documented note), ordered by strategy
n number of injected fingers with real triggering
Strategy A (dexamethasone, 1-month scheduled return), representing 37 % of all the fingers, had the lowest initial resolution rate (18 %) and the highest proportion of patients having surgery within 4 months (53 %). Surgery was done significantly (p<0.01) more often and sooner than in the other strategies, but this strategy had the lowest final triggering rate of 10 %. Strategies B and C resulted in a similar triggering rate of nearly 20 % at the final visit.
Discussion
This study demonstrates that the effectiveness of corticosteroid injection for idiopathic trigger finger is highly dependent on treatment strategy. An early surgery strategy resulted in more surgeries and fewer patients with apparent recurrence or persistent triggering in the final record. Consistent with prior data, triamcinolone was associated with greater initial apparent resolution and greater apparent recurrence [17].
It is possible that the high rate of apparent resolution (83 %) and apparent recurrence (50 %) in the triamcinolone group is due at least in part to inaccurate presumed resolution on the part of the patient or surgeon, which may be an artifact of the treatment strategy. We have observed many patients that perceive resolution when they have simply learned to avoid triggering. With a forceful grip in the office, the triggering can still be elicited. It is likely that doctors vary in the degree that they attempt to elicit triggering when patients report resolution of symptoms. Conversely, the relatively low rate of apparent resolution (30 %) and apparent recurrence (13 %) with dexamethasone may be a result of the fact that one surgeon recommended surgery within 1 month (perhaps before the steroid could have adequate effect) and surgery is very successful in permanently resolving triggering. On the other hand, a recurrence rate of around 50 % has been observed before in studies of betamethasone [3, 7, 23] and triamcinolone [9, 18] injection for idiopathic trigger finger. More studies are needed to determine the relative influence of treatment strategy and type of corticosteroid.
Another important consideration is the retrospective nature of this study. Fleisch and colleagues pointed out that non-randomized studies indicate that steroid injections may be successful in up to 87 %, whereas randomized controlled trials demonstrate a much lower resolution rate of 57 % [4]. Our apparent resolution rate is more consistent with that observed in randomized trials, perhaps because of early surgery with one strategy as well as the inclusion of only Quinnell grade 2 or greater triggering. Another possibility is that retrospective case series tend to overestimate the response of trigger fingers to corticosteroids by excluding patients that do not return within a short time interval and by counting symptom resolution as success when there may be persistent undetected triggering. That trigger thumbs respond significantly better to corticosteroid injections than other digits is consistent with prior work [5, 12].
Rozental et al. identified insulin-dependent diabetes mellitus as an independent predictor of recurrence of symptoms [18]. Only orally treated non-insulin-dependent diabetes mellitus was a predictor of recurrence in our study, perhaps because we only counted Quinnell grade 2 or greater triggering as a true recurrence, whereas Rozental and colleagues diagnosed recurrence based on pain alone. Many surgeons would make this diagnosis in the absence of frank triggering and would therefore disagree with our strict definition of recurrence.
This study should be interpreted in light of the fact that the definitions of apparent resolution and apparent recurrence of trigger finger are imprecise and dependent upon the limited data available in the medical record as well as the interpretations of both the patient and the provider. In rare cases, it was not possible to clearly distinguish Quinnell grade 1 from grade 2. As mentioned, imprecision may be introduced by the fact that triggering can take some effort to elicit, particularly when a patient is in pain. Therefore, persistent trigger fingers may have been mistakenly labeled as resolved. For the substantial percentage of patients that never had documented resolution of triggering, we do not know if the triggering eventually resolved or if they had treatment elsewhere.
The time thresholds were chosen arbitrarily according to the current literature and our clinical experience. The minimum follow-up duration of 3 months is possibly insufficient to identify recurrence of triggering, since recurrence may first become apparent after 6 to 12 months [18]. In addition, the trigger fingers of the patients that had multiple trigger fingers injected were analyzed statistically as if they were separate entities. However, the outcome of these fingers after injection is not independent of the outcome of other injected fingers in the same patient. Finally, a small but unknown number of fingers may have had a prior, undocumented injection elsewhere. Occupation, obesity, carpal tunnel syndrome, and other important factors may play a role in resolution and recurrence of triggering; however, these points were not adequately recorded and therefore not analyzed.
Our data suggest that if corticosteroid injection is elected, greater success is achieved by waiting at least 2 months before deeming the injection ineffective. It also confirms that surgery was a more successful and definitive treatment strategy than corticosteroid injection. A prior analysis suggested that two corticosteroid injections followed by operative A1-pulley release is the most cost-effective approach to resolve an idiopathic trigger finger [8], but patient satisfaction was not addressed. We plan to offer patients surgery or steroid injection on initial diagnosis and study patient satisfaction with their elected treatment strategy. We also plan to study the role of decision aids in decreasing decision conflict and improving patient satisfaction.
Footnotes
All named authors hereby declare that they have no conflicts of interest to disclose related to this study.
The authors adhere to the ethical standards described by the Committee on Publication Ethics and the International Committee of Medical Journal Editors. The study was completed under an IRB-approved protocol.