
Abstract
Introduction
Rupture of the extensor pollicis longus (EPL) tendon is a disabling complication occurring with an estimated frequency of 0.07 to 0.88 % following fracture of the distal radius in adults [1, 5, 6, 9]. In this population, most tendon ruptures occurred 4 to 8 weeks after trauma [13], affecting people at an average age of 53 years [9]. The incidence of EPL tendon rupture is even lower in the pediatric population, and there is limited literature on this subject. The few pediatric case reports have described EPL tendon rupture following either severe injuries requiring intramedullary nailing and open reduction [1, 12, 16] or a markedly displaced fracture [3, 5, 11]. Herein we report a case of delayed EPL tendon rupture in a 15-year-old boy 9 weeks following a nondisplaced distal radius fracture.
Case Report
A 15-year-old boy sustained a nondisplaced Salter–Harris II right distal radius fracture after a fall onto his outstretched hand while playing soccer (Fig. 1). For treatment of the fracture, he was casted for 5 weeks and achieved full function of his right hand and wrist postinjury. Four weeks after cast removal, while the patient was texting on his mobile phone, he noticed a sudden inability to extend his right thumb. This incident was painless and was not associated with any trauma at the time. Rupture of the EPL tendon was confirmed clinically (Fig. 2), and a radiograph showed a well-healing distal radius fracture. Surgical exploration revealed that the proximal portion of EPL was significantly attenuated and frayed up to the musculotendinous junction (Fig. 3). A tendon transfer was therefore performed using extensor indicis proprius (EIP) to EPL using the Pulvertaft weave technique (Fig. 4). There was no bony irregularity, no bony spicule, and no prominent Lister's tubercle evident at the time of the tendon transfer. The patient was casted for 6 weeks and commenced hand therapy consisting of range of motion and strengthening exercises.

Plain radiographs taken at the time of injury show a nondisplaced distal radius fracture

Preoperative view of a clinical confirmation of right EPL tendon rupture based on the patient's inability to extend and elevate the right thumb

Intraoperative view of the frayed EPL tendon and the harvested EIP tendon for transfer

Intraoperative view of the EIP to EPL tendon transfer using Pulvertaft weaves
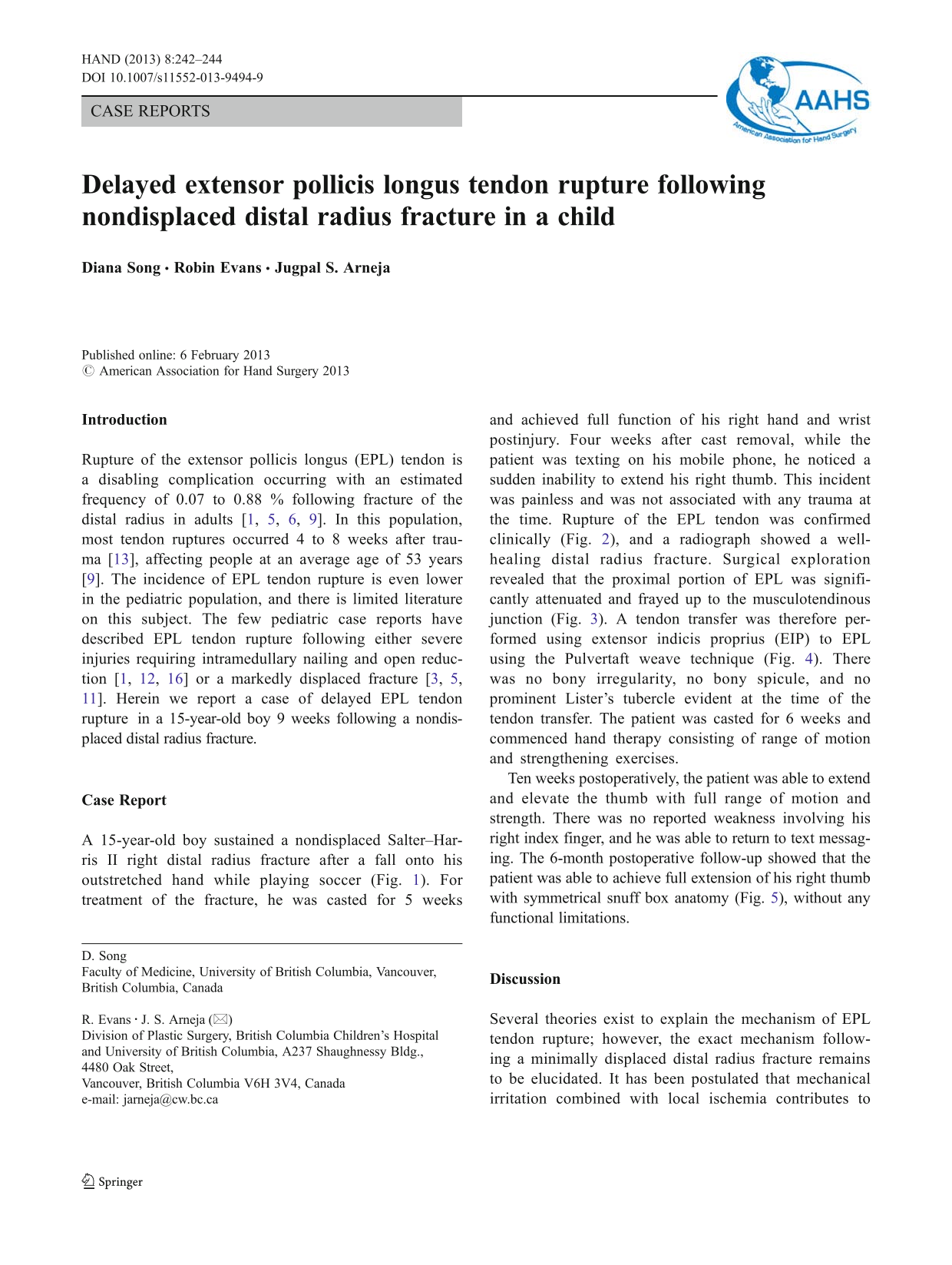
Ten weeks postoperatively, the patient was able to extend and elevate the thumb with full range of motion and strength. There was no reported weakness involving his right index finger, and he was able to return to text messaging. The 6-month postoperative follow-up showed that the patient was able to achieve full extension of his right thumb with symmetrical snuff box anatomy (Fig. 5), without any functional limitations.
Symmetrical snuff box anatomy with full right thumb extension and elevation 6 months postoperatively
Discussion
Several theories exist to explain the mechanism of EPL tendon rupture; however, the exact mechanism following a minimally displaced distal radius fracture remains to be elucidated. It has been postulated that mechanical irritation combined with local ischemia contributes to late rupture of the tendon [2]. This theory is supported by two pediatric cases involving intramedullary nailing of the radius [12, 16]; the rupture was attributed to physical abrasion of the tendon over the edge of a screw. It has also been suggested that the tendon can become injured on the fractured fragments during reduction [10]. However, in the setting of a nondisplaced and nonreduced fracture, these mechanisms seem unlikely. A more plausible theory proposed by Engkvist and Lundborg [4] suggested that increased pressure within the nonruptured tendon sheath after injury compromises the vascular supply of the tendon leading to ischemia, devitalization, or necrosis. A fracture without displacement may still be severe enough to cause effusion or bleeding inside the intact synovial sheath and adversely affect the microvasculature around the tendon [4, 7]. This event is especially problematic to areas of the tendon that already receive attenuated blood supply such as regions near the musculotendinous junction [4, 8]. We surmise that given the absence of a bony spicule postfracture or a prominent Lister's tubercle, rupture in this patient was due to vascular compromise creating ischemia and ultimate rupture at the musculotendinous junction.
Management of EPL tendon ruptures generally fall under three categories: primary repair, tendon graft, or tendon transfer. The EIP tendon transfer was selected because of the difficulty repairing the tendon at the level of the musculotendinous junction. Reported long-term complication with this procedure has been extensor lag or index weakness [14, 15, 17], neither of which was present in our patient 6 months postoperatively. Given the frequency of radius fractures, no preventative measure are suggested; however, despite the infrequent nature of EPL rupture postradius fracture in the pediatric population, a high clinical suspicion for this type of injury is warranted.
Footnotes
The authors declare that they have no conflict of interest.