
Abstract
A clinical case of a 12-year-old boy who presented with multidigit, nonsyndromal, progressive camptodactyly is discussed. While bilateral little finger camptodactyly is well described, there is no documentation of camptodactyly involving all fingers and many toes as well as both proximal (PIP) and distal interphalangeal (DIP) joints. This patient responded well to surgery, which was performed on four toes and seven fingers, despite having established radiographic changes of camptodactyly in the PIP joints as well as two DIP joints. This case illustrates that in the skeletally immature patient, successful surgical outcomes can occur even in patients with radiographic bone changes, which themselves may be reversible following PIP contracture release. This patient's separate fingers presented with deformity at different stages. A single patient with multiple digit involvement is illustrative of the range of clinical presentations and treatment options for camptodactyly. This article serves to inform hand surgeons about the potential consequences of avoiding surgical treatment, the need for a severity staging system, and the breadth of presentations in camptodactyly.
Keywords
Introduction
Simply stated, camptodactyly means bent finger, which has come to imply flexion at the proximal interphalangeal (PIP) joint [11]. Most commonly, camptodactyly involves the little finger and may be bilateral. Multidigit involvement is infrequently described and typically associated with syndromal conditions [1, 5]. Prior publications abound with controversy regarding pathogenesis, anatomic structures involved, and treatment. Many advocate avoidance of surgery [1, 6, 8, 10]. Others recommend surgery for more severe contractures (over 60° flexion at the little finger PIP joints) and have reported varying success [2, 4, 7, 9, 12].
We describe a patient with nonsyndromal camptodactyly involving every finger and also toe involvement. Each digit displayed varying severity of both clinical and radiologic changes. Even the distal interphalangeal (DIP) joints of bilateral index fingers were involved, indicating that the PIP joint is not the only joint to be affected. Although this patient showed some atypical features of camptodactyly, the varying degrees of finger severity enable a suggested unifying theory (at least in this patient) for development of camptodactyly, much as that proposed by Smith and Grobbelaar [11]. This case study not only serves as an interesting report, but also reviews the differential diagnosis and illustrates that surgery to both hands and feet can be successful. It has taught us the importance of both a clinical and a radiographic severity score, and it shows in our young patient who still had open phalangeal epiphyses that these radiographic changes may be reversed. Indeed, there may be an urgency to perform surgery in the preadolescent in select cases before skeletal maturity is attained and the skeletal and clinical changes become permanent.
Case Report
This young boy first presented to us at age 12 years. He had multiple finger and even toe involvement with camptodactyly. He was completely healthy, of normal appearance and stature, and highly intelligent with a good class ranking in school. Family history was negative for camptodactyly, and he had nothing to suggest any associated syndromes.
His parents noted that the right little finger first started to flex at age 7 years, followed by the ring finger. The contractures steadily progressed, and by age 11 he had deformity to the left little and ring fingers. In the 6 months preceding our first consultation, other fingers and even the toes had started to flex. In that time, he consulted with another hand surgeon, who subsequently referred him to us, as the patient had undergone several months of splinting and serial casting that failed to halt the contractures' progression. The deformities actually continued to worsen during this treatment.
At the first consultation with us, the patient's worst affected digits were the right little and ring fingers. He had boutonniere deformities affecting bilateral little, ring and middle fingers, and swan neck deformities at the bilateral index fingers. The PIP flexion contractures at the right, little and ring fingers were fixed and independent of wrist and metacarpophalangeal (MP) joint flexion positioning. Compensatory hyperextension was present at the MP joints of the right middle, ring and little fingers, and at the left little finger. With fingers held in active extension, joint measurements are shown in Table 1. The clinical presentation is shown in Fig. 1. He was able to make a fully clenched fist. Thumbs appeared uninvolved.
Clinical assessment of digits affected by camptodactyly before and after surgery
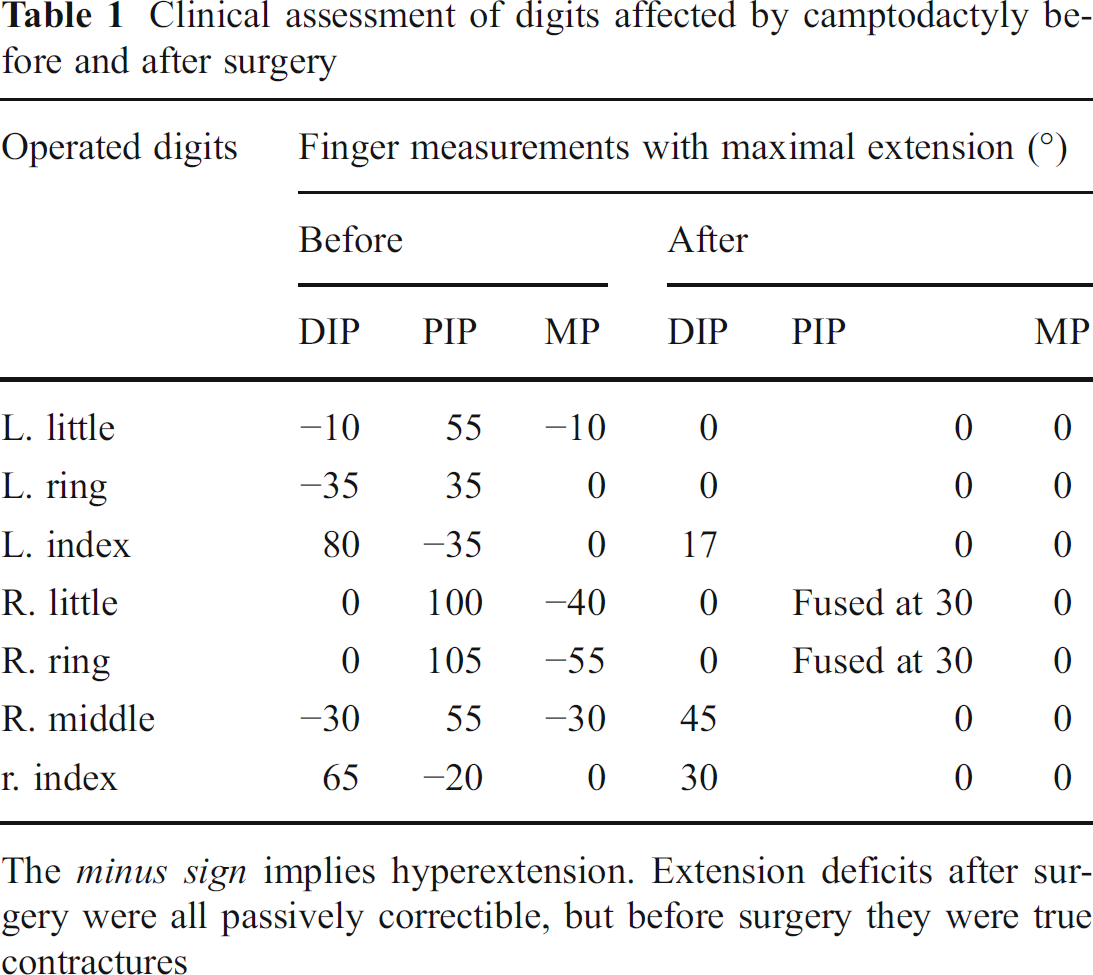
The minus sign implies hyperextension. Extension deficits after surgery were all passively correctible, but before surgery they were true contractures
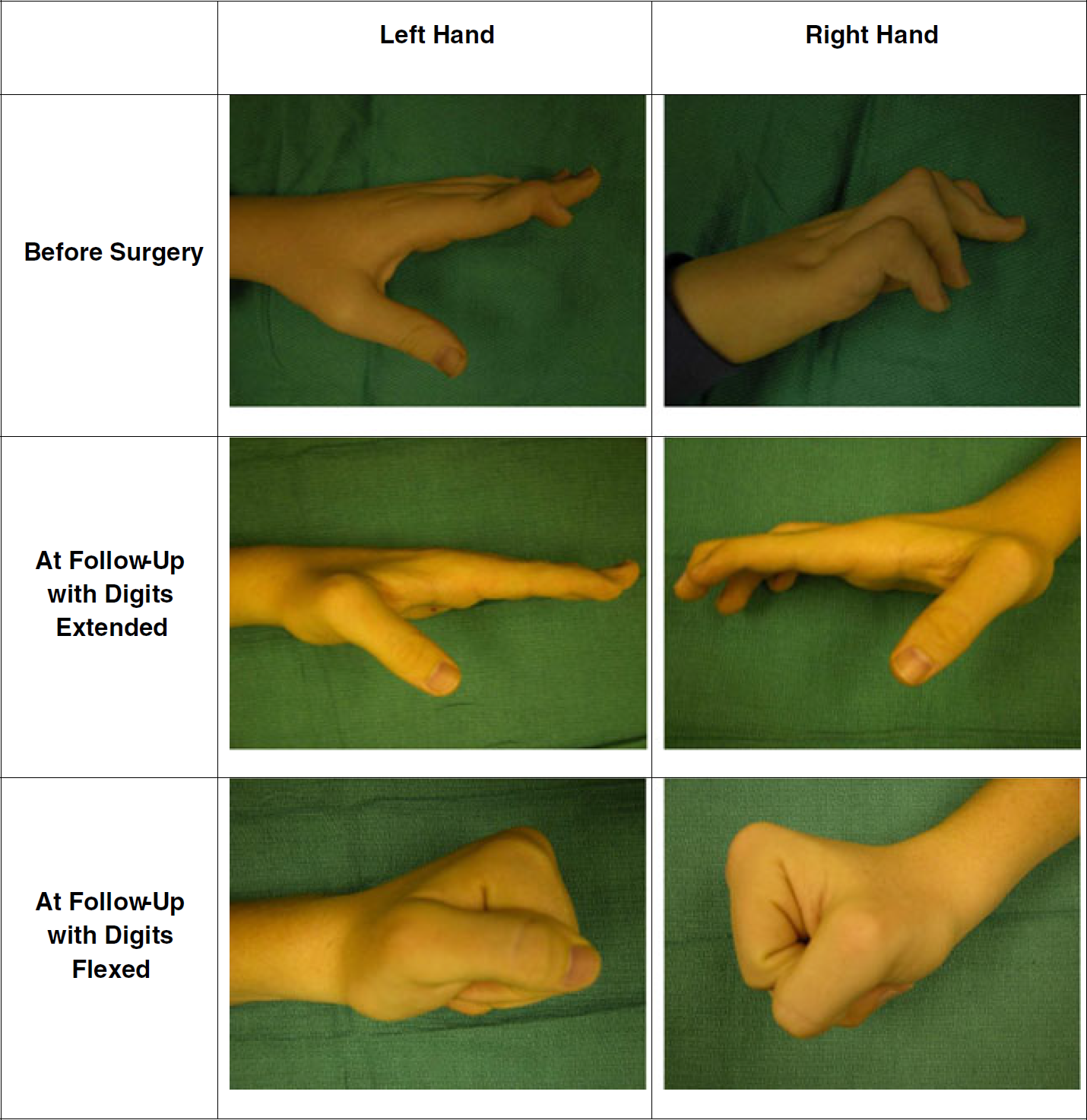
Left and right hands before and after surgery. Clinical photographs of the patient's left and right hands before surgery and at follow-up after surgery had been performed. Both hands can make a full fist
He was also developing flexion contractures at the PIP joints of some of the toes that caused pain on walking as the toes dug into the ground, and he was developing toe DIP joint compensatory hyperextension. The patient was talented musically and enjoyed being in the marching band, but this activity had become increasingly difficult due to his forefoot pain.
Hand radiographs showed varying severity of joint involvement that paralleled the clinical presentation of each finger (Fig. 2). The right little and ring fingers showed total dislocation of the PIP joint with articular destruction. The left middle finger was the least severely affected clinically, and the PIP joint was near-normal in lateral radiographic profile. However, the PIP joints of the other fingers showed “beaking” of the distal end of the proximal phalanx with loss of the rounded convexity, and flattening of the articular surface at the base of the middle phalanx with the proximal phalangeal articulation riding dorsally on the middle phalanx and volar subluxation. Interestingly, DIP joints of the index fingers showed similar radiographic articular changes to the PIP joints.

Pre-operative radiographs of the left and right digits: left hand top row, right hand bottom row. Left hand: the head of the middle phalanx of the left index finger developed a high-riding articular defect presenting as a mallet deformity
Clinical assessment showed longitudinal webbing of soft tissues (pterygium) across the volar aspects of the PIP joints of bilateral ring and little fingers, and also of the right middle finger. The right little and ring finger PIP joint contractures persisted independently of more proximal MP joint flexed positioning. Although the PIP joints were dislocated both clinically and radiographically, they could still flex into the palm, albeit with a very narrow flexion arc. Right middle and contralateral left little and ring finger PIP joint flexion contractures improved but did not fully correct with passive MP joint flexion. The mild flexion deformity of the PIP joint of the left middle finger that was noted with active finger extension was fully passively correctable. The DIP joint flexed positions at the index fingers could correct when the PIP joint was flexed. Even with active attempted PIP joint extension and with the MP joints blocked in flexion, a PIP joint extension lag (Bouvier maneuver) remained at the right middle finger and left little and ring fingers.
The patient had a series of four surgeries over the ensuing year to systematically treat the second, third and fourth toes of the right foot and every finger (except the left middle finger). The left middle finger's deformity remained sufficiently minimal to not require surgery. The left little and ring finger progressed to PIP contractures of 55° and 35°, respectively, requiring correction. Chondrodeses (arthrodeses with preservation of epiphysis) were done at the right ring and little fingers as the PIP joints were too damaged to be salvaged. At the right middle finger, he underwent Fowler distal extensor tenotomy, local flap and full thickness skin grafting to address the pterygium and flexor digitorum superficialis (FDS) transection through an A3 pulley window in the flexor sheath. Bilateral index finger deformities were treated by soft tissue releases and full-thickness skin grafting at the volar DIP joint, along with spiral oblique retinacular ligament (SORL) tenodesis using a palmaris longus tendon autograft. The left ring and little fingers underwent distal Fowler tenotomy for DIP joint hyperextension deformities, combined with local soft tissue extensor tendon repair for the boutonniere problems, a volar soft tissue release with local transposition flap and ***full-thickness skin grafting, and FDS transection with volar plate release. In these two fingers, the transected FDS was in turn used for intrinsic transfers, having previously established that there was independent FDS function to both little and ring fingers by clinical testing. The lumbricals were uninvolved throughout. The toes were treated by open flexor tenotomy and volar z-plasties with excellent resolution of the flexion deformities.
At the culmination of these staged procedures, both the patient and his parents were pleased with the clinical outcome. Three years following his last procedure, the patient's hands have now reached radiographic skeletal maturity. Interestingly, the radiographic articular deformities at the affected PIP and DIP joints have completely resolved (Fig. 3). The PIP joints of the right little and ring fingers are fused. He can make bilateral clenched fists and extend his fingers (making an allowance for the two fingers with PIP joint fusions) and has a slight residual extension lag at some DIP joints but no contractures (Fig. 1). His right toes remain contracture-free. The left toes have worsening contractures but are not yet painful. He may require future surgery (Fig. 4).

Post-operative radiographs of the left and right digits: left hand top row, right hand bottom row. Left hand: the mallet deformity of the left index finger is no longer apparent, and the joint appears radiographically normal

An operated and unoperated foot. The patient's left, unoperated toes
His foot pain with walking has resolved, and he has rejoined his marching band. He can play the trumpet efficiently and has resumed playing guitar, which he had previously given up because of his dysfunctional finger deformities.
Discussion
Camptodactyly is defined simply as a flexion contracture of the PIP joint of the finger. It is said not to affect the DIP joint primarily, although compensatory DIP joint deformities may occur in a reciprocal direction to the more proximal PIP joint flexion [3]. Camptodactyly may have progressive deformity, and surgical treatment has been advised when there is a dysfunctional flexion contracture that has been unresponsive to nonoperative measures. Although camptodactyly has been classified into three types based on age of onset and presence of associated syndromes, there is no classification based on severity of joint changes, especially in the growing immature skeleton. The DIP and MP joints are unaffected, except in a compensatory manner for the PIP joint flexion deformity. Multidigit, aggressively progressive deformities occur, especially in syndromal types. Involvement of the toes has not been described.
The differential diagnosis of camptodactyly includes distal arthrogryposis. However, the thumb is frequently affected in that condition and is often associated with extensor deficiency and stiff joints. He had no other clinical features to suggest Freeman–Sheldon syndrome. Primary absence of extensor tendons is another possible differential diagnosis, and can affect multiple digits, but this patient had excellent extrinsic extensor function. Pediatric trigger finger is a different condition from the adult variety and more typically has tightness at the FDS decussation and chiasma. This may lead to flexion contracture, but more typically produces snapping of the finger. Generalized syndromal conditions may be associated with multiple digit camptodactyly, and one should assess for these. They include associated craniofacial disorders, chromosomal trisomy disorders, and those associated with short stature, such as mucopolysaccharidoses and camptomelic dysplasia.
We discuss a clinical case of a now 16-year-old male who presented with multidigit bilateral camptodactyly. We have learned not to be too dogmatic about classifications of camptodactyly, and our past clinical experience has identified patients that presented at a young age (so-called Type I) with multidigit camptodactyly that was progressive and severe in the absence of associated syndromes. Likewise, we have seen older pre-adolescent children (so-called Type II) with mild single digit (little finger) camptodactyly that did not progress to worsening flexion contracture. This is in contradistinction to what is most frequently reported with these two types.
This patient emphasizes that one cannot be too dogmatic about generalizations because he was atypical in many ways. However, his management also helps provide some unifying guidelines about camptodactyly that help in the treatment algorithm.
Atypical features in his presentation are as follows:
He had multidigit nonsyndromal progressive camptodactyly.
All fingers and all toes (except the great toes) were affected.
Seven of eight fingers and four toes required surgical intervention. Toe affliction has not been previously reported. Three of his toes have been operated on, and the remaining ones may necessitate future surgery as they continue to worsen.
The DIP joints of both index fingers had the classical radiographic changes of camptodactyly (without PIP joint involvement of the index fingers). All other fingers had PIP involvement.
PIP joints showed a range of severity from total dislocation and articular surface destruction to the classical misshapen convexity of the proximal phalangeal head that rides dorsally on the base of the middle phalanx and with the flexed middle phalanx creating an indentation in the palmar neck of the proximal phalanx to a near-normal articulation in other digits. Our patient showed the full spectrum of these radiographic changes in different fingers.
It has been said that once skeletal changes occur, these bone changes further downgrade expectations after surgeries. However, this case illustrates that in the growing skeleton, these radiographic bone changes do not necessarily preclude successful surgical outcome and may actually be reversible following PIP contracture release.
All PIP periarticular structures have been implicated as causative. However, it is difficult to identify which are primary versus secondary changes. Our patient seems to support the unifying hypothesis proposed by Smith and Grobbelaar [11]. The primary deformity appeared to involve the flexor tendon with secondary changes resulting in skin tethering (pterygium) and formation of abnormal fascial bands beneath the skin, and then PIP joint soft tissue and skeletal changes. The lumbricals were uninvolved. Due to PIP joint flexion, the dorsal central slip extensor mechanism may become attenuated and even result in compensatory hyperextension boutonniere deformity at the DIP joint. There also may be compensatory MP joint hyperextension. All these changes were seen to varying degrees in the fingers affected to different severities.
This patient highlights, through multiple affected digits, that there may be indeed a unifying theory of evolution of PIP joint camptodactyly and may help in developing a treatment algorithm. The surgical incision needs to be preplanned to allow for z-plasties, local flap or skin grafting to address the skin deficiency. The FDS is divided through an A3 pulley tendon sheath window. PIP joint release may be required, dependent on the contracture's severity. We performed an FDS intrinsic tendon transfer to two fingers that we thought were affected particularly severely. However, in other digits, according to the advice of Smith and co-workers, the central slip and intrinsic function will rebalance with judicial postoperative splinting in those digits less severely affected. Compensatory MP joint deformities correct with resolution of the PIP joint problem.
An interesting phenomenon was that both PIP and DIP joint radiographic changes appear to return to normal (except in the two fused fingers) after successful soft tissue correction. This phenomenon is previously unreported. Furthermore, these radiographic joint changes did not seem to preclude successful surgical treatment of the flexion contracture. This may potentially make a case for surgical intervention once radiographic skeletal changes are noted and not based on severity of clinical contracture alone. This may be even more important in preadolescent patients, who are rapidly approaching skeletal maturity. One can only assume that by the time maturity is attained, skeletal changes (and hence contracture) would remain fixed.
Unusual features of our patient were severe multidigit nonsyndromal camptodactyly, toe involvement severe enough to warrant surgery, two fingers that involved DIP joint camptodactyly, and two PIP joints that were so severely affected that chondrodesis was required.
This patient's uniqueness is the multidigit involvement with the full spectrum of severity in different fingers. The pathogenesis of camptodactyly is controversial. Essentially, all structures surrounding the affected joints have been implicated in its pathogenesis [2, 6, 10, 11]. Our clinical impression is that camptodactyly is caused by a soft tissue deficit involving many components. In our patient, the FDS was tethered too tightly, soft tissue around the joint was too tense, the extensor mechanism was stretched in a compensatory manner, and the skin and subcutaneous tissues were foreshortened. With these unnatural forces acting on the joint, articular changes result as seen radiographically. As we believe multiple soft tissue structures are involved in camptodactyly, our surgical approach is stepwise that systematically releases the restraining structures until the digits are passively extendable. The extensor attenuation most frequently accommodates with judicious postoperative splinting. Occasionally, FDS intrinsic transfer and central slip reconstruction may be required. This approach, however, does risk the potential loss of full PIP joint flexion postoperatively.
Footnotes
The authors declare that they have no conflict of interest.