
Abstract
Background
Osteoarthritis of the radiocarpal joints is commonly encountered by hand surgeons. To date, there is no well-defined method of radiographically grading osteoarthritis of the wrist.
Methods
Preoperative radiographs of 48 patients undergoing wrist arthroscopy were evaluated retrospectively. Images were graded subjectively by five surgeons based on overall severity of arthritis, osteophytes, subchondral cysts, and subchondral sclerosis. The joint space height (JSH) ratio was calculated by measuring the space of the mid-radioscaphoid and mid-radiolunate joints and dividing each by the height of the capitate. Arthroscopic grading of arthritis was obtained from operative records and compared to subjective and objective grades. ANOVA testing evaluated for statistical significance with p<0.05. Inter-rater and intra-rater reliability was determined using Pearson's correlation analysis and Cohen's kappa coefficient.
Results
Objective measurement using the JSH ratio demonstrated a significant decrease as arthroscopic arthritis grade increased for both radioscaphoid and radiolunate joints. Subjective grading of radioscaphoid and radiolunate joints was able to detect moderate/severe, but not mild arthritis. Subjective grading underestimated the degree of arthritis, particularly in the radiolunate joint. Inter-rater reliability was better for objective compared to subjective grading.
Conclusions
Subjective grading of wrist arthritis can detect moderate/severe radiocarpal arthritis but poorly evaluates early arthritis and underestimates severity. Objective grading using the JSH ratio accurately grades radioscaphoid arthritis and detects early radiolunate arthritis. The JSH ratio more accurately assesses radiocarpal arthritis compared with subjective grading. As there currently is no accepted method to radiographically grade wrist arthritis, the JSH ratio represents a promising option.
Introduction
Osteoarthritis of the wrist is a common condition treated by hand surgeons, which can result from a variety of causes [17]. Common etiologies include posttraumatic [7], scapholunate advanced collapse (SLAC) [15], scaphoid nonunion advanced collapse (SNAC) [14], and late effects of avascular necrosis [1]. Arthritis of the radiocarpal joints results in pain, abnormal wrist biomechanics, and functional limitation for patients.
The progression of wrist arthritis has been best delineated with studies evaluating the stages of the development of a SLAC wrist, which can develop after a scapholunate ligament injury [12]. The radial styloid–scaphoid junction is affected early (stage I), followed by progression to the entire radioscaphoid joint (stage II). Stage III also includes the capitolunate junction. Stage IV disease affects the entire radiocarpal joint, including the radiolunate articulation, as well as the intercarpal joints [15–17]. Only in advanced SLAC wrist is the radiolunate joint thought to be affected.
Arthroscopic evaluation is often considered to be the gold standard for evaluating articular cartilage integrity. Multiple studies have demonstrated that arthroscopic evaluation of articular cartilage is reproducible between surgeons, especially in surgeons with greater than 5 years of experience [3, 10]. While arthroscopic evaluation is reliable, this method is invasive and therefore is not a clinically useful method to screen patients presenting to clinic for wrist arthritis severity.
Despite the prevalence of wrist arthritis, there are limited systems described to grade arthritis based on radiographs, and few have been validated. In evaluating patients following distal radius fracture, Knirk and Jupiter [7] subjectively graded wrist arthritis on a scale of 0 to 3. Zero was described as no evidence of arthritis, 1 with slight joint space narrowing, 2 with marked joint space narrowing and osteophyte formation, and 3 with bone on bone joint space narrowing, osteophyte formation, and cyst formation. White et al. [18] proposed a method of scoring scaphotrapeziotrapezoidal arthritis based on objective joint space narrowing, sclerosis, and irregularity of the joint space. Another recent study of patterns of radiocarpal arthritis uses only subjective joint space narrowing agreed upon by three surgeons as the defining feature of arthritis [9]. Trapeziometacarpal arthritis has been graded based on subjective joint space narrowing and size and presence of osteophytes as well as number of joints involved [4]. Overall, there is little consistency or objectivity in the grading of wrist arthritis.
There are better defined and more commonly utilized systems for radiographically grading osteoarthritis of the knee, including the commonly used Kellgren–Lawrence method, which subjectively grades images based on joint space narrowing, osteophytes, subchondral sclerosis, and deformity [15]. Takahashi et al. [13] found a significant inverse relationship between objective measurement of radiographic joint space height of the tibiofemoral joint and Kellgren–Lawrence grade. However, Kijowski et al. [6] found at best a moderate correlation between subjective radiographic grading of knee osteoarthritis and arthroscopic findings of osteoarthritis. In combination, these data suggest that more sensitive methods are needed to evaluate osteoarthritis radiographically, even in the well-studied tibiofemoral joint.
The purpose of this study was to determine an optimal method to radiographically grade wrist arthritis. Both objective and subjective grading systems were used, and these were compared to arthroscopic grading, which was used as a gold standard for evaluation of articular cartilage integrity. We hypothesized that objective radiographic grading of wrist arthritis severity, using joint space height (JSH), would correlate better with actual degree of arthritis than subjective grading.
Methods
Forty-eight patients (25 females, 23 males) who underwent diagnostic wrist arthroscopy were retrospectively evaluated. The average patient age was 47.6 ± 2.0 years. Degree of radioscaphoid and radiolunate cartilage degeneration was carefully assessed intraoperatively by a single surgeon using the modified Outerbridge classification [11]. Grade 0 cartilage was considered normal. Grade 1 and 2 cartilage was considered mild arthritis, while grade 3 and 4 cartilage was considered moderate/severe arthritis. Due to the limited number of patients in the more severe groups, as well as the surgeon occasionally describing “grade 1 to 2” or “grade 3 to 4” changes in a given joint, groups were combined for statistical analysis.
Preoperative posteroanterior (PA) and lateral wrist radiographs were evaluated for each patient. Subjective grading was performed by five hand surgeons who were blinded to arthroscopic grade. Surgeons graded the overall severity of radioscaphoid and radiolunate arthritis (0=normal, 1=mild, 2=moderate, 3=severe). In addition, osteophyte size (0=none, 1=small, 2=large), presence of subchondral cysts (0=none, 1=small, 2=large), and sclerosis (0=none, 1=mild, 2=severe) were each graded. Those three scores were then combined to generate a combined subjective score (range, 0–6). The five surgeon's scores for each category were averaged and the resultant mean score was used for comparison. Inter-rater reliability between the subjective scores was determined using kappa statistic testing.
Objective grading was determined by measuring the length of the mid-radioscaphoid and mid-radiolunate joints on standard PA wrist radiographs (Fig. 1). Measurements were obtained using the digital measurement system on the ImageJ software program. The mid-radioscaphoid length was determined by measuring the length of a line which was perpendicular to the volar surface of the scaphoid facet and connected the scaphoid to the volar surface of the radius. Similarly, the mid-radiolunate length was determined by measuring the length of a line which was perpendicular to the volar surface of the lunate facet and connected the lunate to the volar surface of the radius. In order to have an internal standardization for lengths between different X-ray systems, JSH ratios were determined by dividing the radioscaphoid and radiolunate joint lengths by the height of the capitate and multiplying this value by 100. JSH ratio measurements were repeated three times by a single surgeon who was blinded to the arthroscopic grades. Intra-rater reliability was determined with a correlation analysis and Pearson's correlation coefficient. JSH ratios were then determined by a second independent surgeon in order to obtain an inter-rater reliability assessment using correlation analysis with Pearson's correlation coefficient. Average subjective and objective grades were then compared to the arthroscopic findings. Statistical significance was determined using one-way ANOVA and the Tukey's post hoc test with p<0.05 being significant.
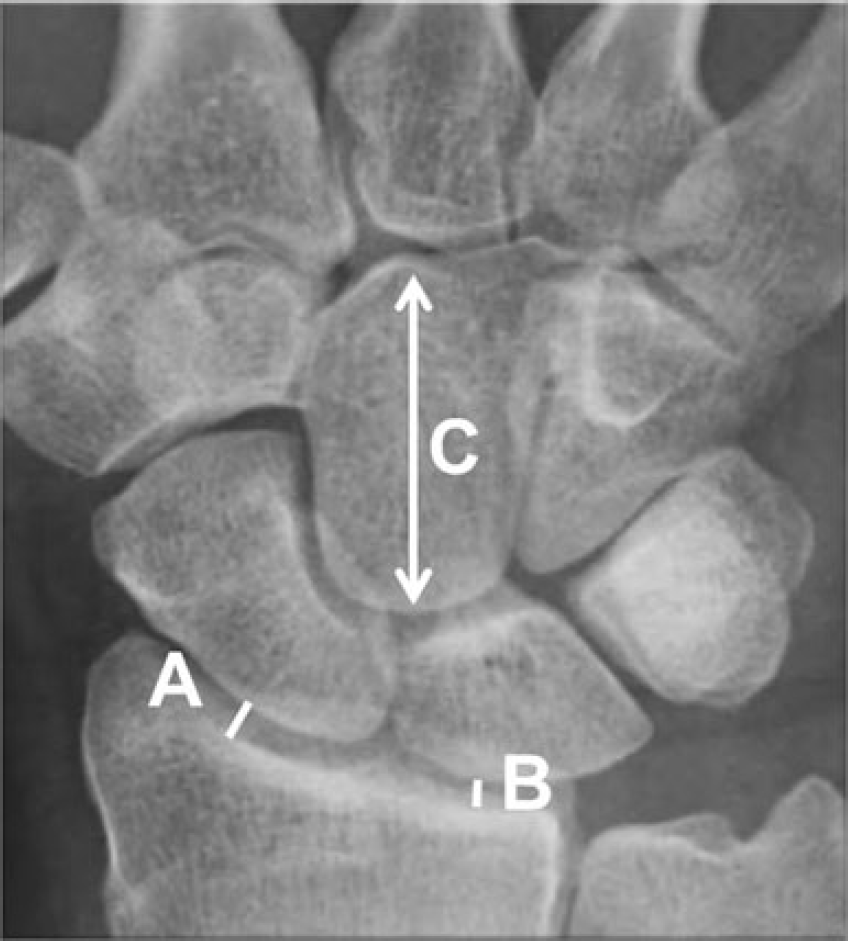
The length of the mid-radioscaphoid (A) and the mid-radiolunate (B) joints were each divided by the length of the capitate (C), in order to determine the joint space height (JSH) ratio for the radioscaphoid (A/C) and radiolunate (B/C) joints
Results
Subjective Grade vs Arthroscopic Findings
In the radioscaphoid joint, arthroscopically normal wrists (n=21) received the following subjective scores (mean±SD): overall arthritis 0.39 ± 2.39, osteophytes 0.24 ± 2.37, sclerosis 0.19 ± 2.25, cysts 0.06 ± 2.2, and combined score 0.37 ± 2.45. Joints with mild arthritis during arthroscopy (n=18) were scored: overall arthritis 0.69 ± 2.43, osteophytes 0.5 ± 2.49, sclerosis 0.37 ± 2.28, cysts 0.26 ± 2.39, and combined score 0.85 ± 2.63. Joints with moderate/severe arthritis during arthroscopy (n=8) received scores of: overall arthritis 1.8 ± 2.7, osteophytes 1.04 ± 2.49, sclerosis 1.08 ± 2.71, cysts 0.71 ± 2.65, and combined score 2.1 ±1.1. There were no statistically significant differences between arthroscopically normal and mild wrists with regard to subjective grading of the radioscaphoid joint. When comparing arthroscopically severe radioscaphoid joints to normal joints, subchondral cysts (p<0.01), overall grade, sclerosis, and combined subjective score all showed a statistically significant (p<0.05) relationship with arthroscopic evaluation (Fig. 2).
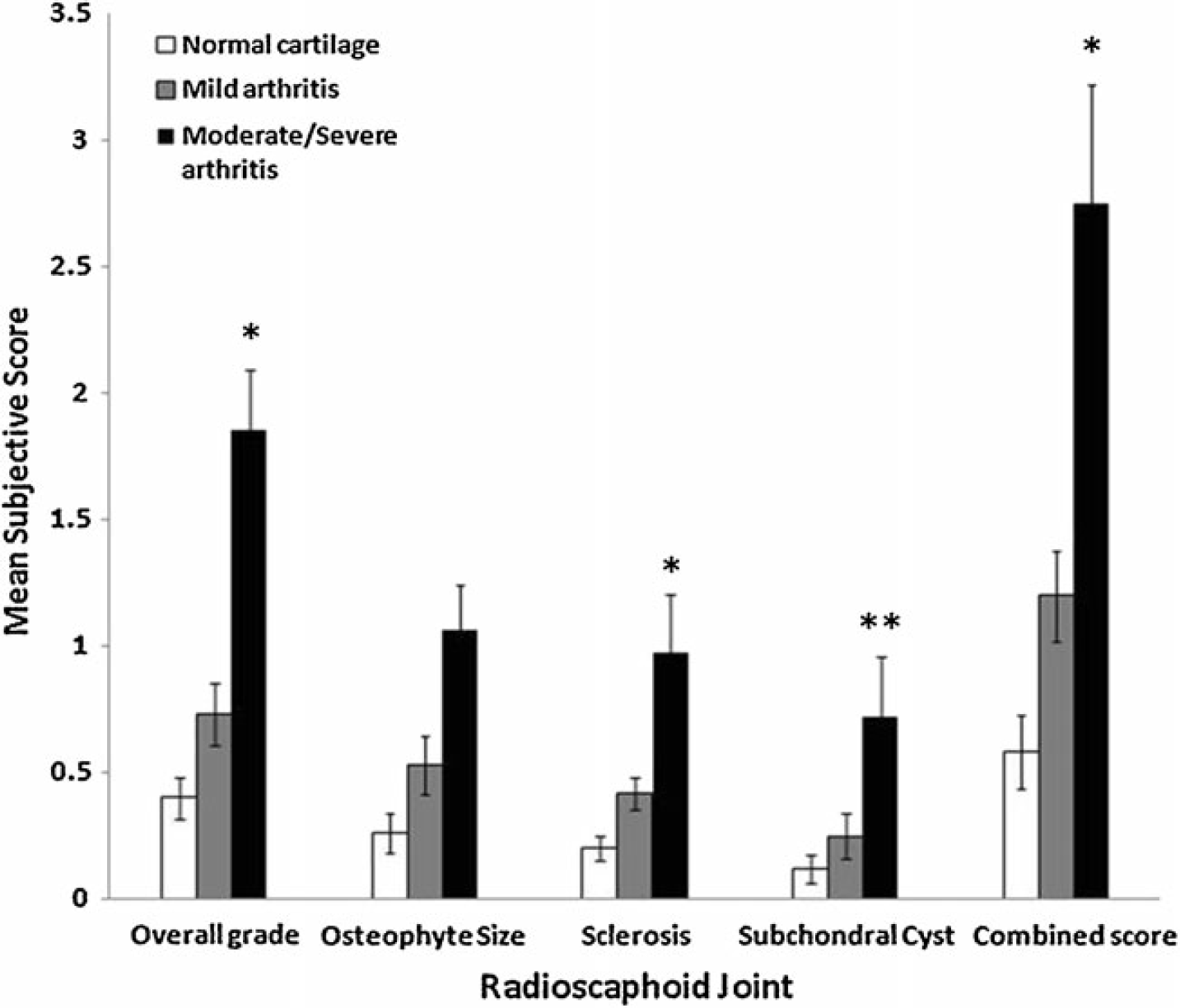
Subjective grading of the radioscaphoid joint was unable to detect mild arthritis, but was able to distinguish between mild and moderate/severe arthritis using overall grade (*p<0.01), sclerosis (*p)<0.01), subchondral cysts (**p<0.05), and combined score (*p<0.01)
In the radiolunate joint, arthroscopically normal wrists (n=26) received the following subjective scores (mean±SD): overall arthritis 0.19 ± 2.22, osteophytes 0.06 ± 2.16, sclerosis 0.19 ± 2.25, cysts 0.06 ± 2.2, and combined score 0.24 ± 2.34. Joints with mild arthritis during arthroscopy (n=15) were scored: overall arthritis 0.28 ± 2.36, osteophytes 0.11 ± 2.21, sclerosis 0.31 ± 0.34, cysts 0 ± 2, and combined score 0.32 ± 2.36. Joints with moderate/severe arthritis during arthroscopy (n=4) received scores of: overall arthritis 1.3 ± 1.1, osteophytes 0.67 ± 2.72, sclerosis 0.67 ± 2.94, cysts 0.67 ± 2.61, and combined score 1.5 ± 2.46. Again, there were no statistically significant differences between arthroscopically normal and mild wrists with regard to subjective grading of the radiolunate joint. When comparing arthroscopically severe radiolunate joints to normal joints, overall grade, osteophyte size, subchondral cysts, and combined subjective score all showed a statistically significant (p<0.01) relationship with arthroscopic evaluation (Fig. 3).
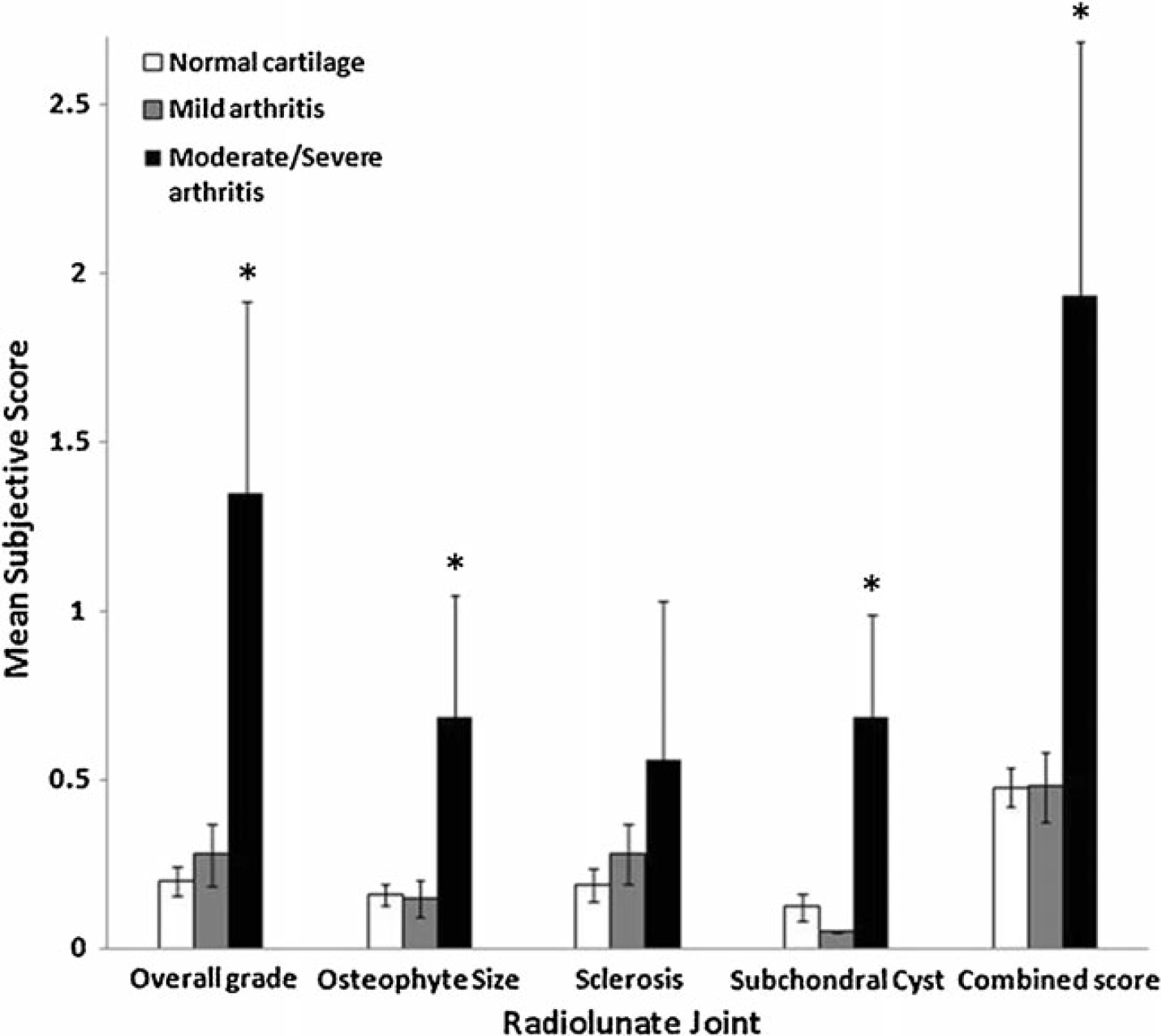
Subjective grading of the radiolunate joint was unable to detect mild arthritis, but was able to distinguish between mild and moderate/severe arthritis using overall grade (*p<0.01), osteophyte size (*p<0.01), subchondral cysts (*p<0.01), and combined score (*p<0.01). Subjective grading of overall arthritis severity grossly underestimated the severity of arthritis present
Objective Grade vs Arthroscopic Findings
The JSH ratio in the radioscaphoid joint measured (mean±SD) 9.8 ± 2.5 in arthroscopically normal joints, 8.3 ± 2.9 in mild arthritis, and 5.9 ± 2.2 in moderate/severe arthritis. In the radiolunate, the JSH measured 10 ± 2.6 in normal joints, 8.4 ± 2.3 in mild arthritis, and 7.0 ± 2.1 in moderate/severe arthritis. For both the radioscaphoid and radiolunate joints, the mean JSH ratio demonstrated a significant decrease as arthritis grade increased (Fig. 4, p<0.01). Post hoc analysis demonstrated a significant difference in the radioscaphoid JSH ratio between the arthroscopically normal and mild arthritis groups (p<0.05), as well as between the mild and moderate/severe groups (p<0.01). There was also a significant difference between the normal and mild arthritis groups in the radiolunate joint (p<0.01), but no difference was found between the mild and moderate/severe groups (p=0.2).
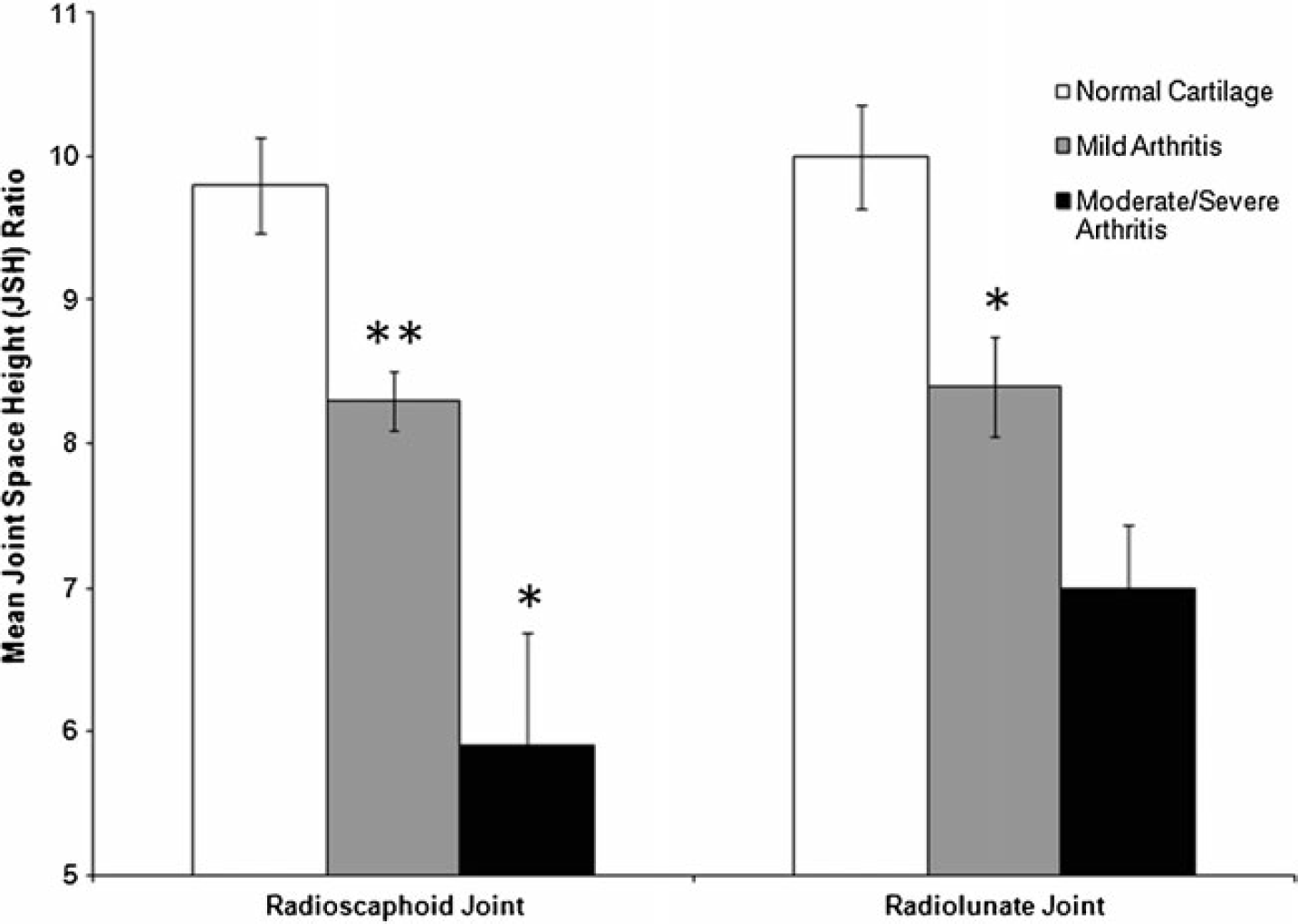
In the radioscaphoid joint, there was a significant decrease in the JSH ratio between the normal and mild arthritis groups (**p<0.05), as well as between the mild and moderate/severe groups (*p<0.01). There was a significant decrease in the radiolunate JSH ratio between the normal and mild arthritis groups (*p<0.01), but no difference was found between the mild and moderate/severe groups
Inter-rater and Intra-rater Reliability Assessments
Inter-rater reliability among the five observers evaluating subjective grade of radiographic wrist arthritis was calculated using Cohen's kappa coefficient. In the radioscaphoid joint, kappa values ranged from 0.21 to 0.46, with 0.46 for osteophyte size 0.40 for overall grade, 0.36 for cysts, and 0.21 for sclerosis. In the radiolunate joint, values ranged from 0.14 to 0.27, with 0.27 for overall grade, 0.24 for sclerosis, 0.18 for osteophyte size, and 0.14 for cysts.
For the objective grading, inter-rater reliability between the surgeons who determined the JSH ratios yielded a Pearson's correlation coefficient of 0.66 for the radioscaphoid joint and 0.67 for the radiolunate joint. Intra-rater reliability between the three different JSH ratio measurements obtained by a single surgeon yielded kappa coefficients of 0.95 and 0.94 for the radioscaphoid and radiolunate joints, respectively.
Discussion
As there is currently no well-accepted, noninvasive, objective measure of wrist arthritis, clinicians are forced to rely on subjective evaluation of imaging to assess arthritis. This investigation has shown that subjective grading by orthopedic hand surgeons may be capable of identifying moderate/severe arthritis of both the radioscaphoid and radiolunate joints; however, it is unable to detect mild arthritis. Overall grade, subchondral cysts, and the combined score could detect moderate/severe arthritis in both joints, while evaluation of osteophyte size and amount of sclerosis was only able to identify moderate/severe changes in one of the two joints.
None of the subjective methods, however, were able to detect mild arthritis changes.
Furthermore, subjective evaluation by trained clinicians was found to grossly underestimate the severity of arthritis present. This was particularly evident in the radiolunate joint. The “overall grade” of osteoarthritis in the radiolunate joint (0=normal, 1=mild, 2=moderate, 3=severe) averaged only 0.28 in the mild arthritis group, and only 1.31 in the moderate/severe arthritis group, demonstrating the underappreciation for the degree of arthritis severity in this joint. This underappreciation of radiolunate arthritis severity may be due, in part, to the current understanding of wrist arthritis progression patterns in which the radiolunate joint is often thought to be spared [5].
Perhaps even more clinically important for the subjective grading was the outcome of the inter-rater reliability analysis. The best kappa value in the radioscaphoid analysis was 0.47, compared to only 0.27 in the radiolunate joint. In general, kappa values of less than 0.2 are considered slight, 0.2 to 0.4 are considered fair, and 0.4 to 0.6 are considered moderate [8]. Based on this, subjective review of radiographs in this series showed no better than fair-to-moderate agreement between raters.
In comparison to subjective grading, objective grading using the JSH ratio was able to more accurately assess the severity of radiocarpal arthritis. The JSH ratio was most accurate in the radioscaphoid joint where it could distinguish between normal, mild, and moderate/severe arthritis. The JSH ratio in the radiolunate joint was able to detect early arthritic changes, but could not distinguish between mild and moderate/severe arthritis. The JSH ratio, therefore, may be used to detect early radiolunate arthritis, which, as this study demonstrated, may go unnoticed by subjective evaluation of radiographs. As treatment algorithms for SLAC and SNAC wrist consider involvement of the radiolunate joint as a factor in surgical decision making, alerting surgeons to the presence of radiolunate arthritis may help to guide treatment.
Inter-rater reliability analysis for the JSH measurements using Pearson's correlation coefficient yielded values between 0.6 and 0.65. Guidelines for Pearson correlation interpretation suggest that the correlation of a coefficient between 0.1 and 0.3 is small, between 0.3 and 0.5 is medium, and between 0.5 and 1.0 is strong [2]. Based on this, the JSH inter-rater reliability correlation is moderately strong. Although these numbers could be stronger, they are likely superior to the inter-rater reliability for the subjective scoring which was previously discussed. Furthermore, the strong Pearson coefficients of 0.95 and 0.94 for the intra-rater reliability of the objective testing suggest that these measurements are highly reproducible for a given surgeon doing the evaluation.
Although we cannot state whether or not there is a clinically significant difference in the ability to detect mild arthritis on radiographs based on this study, the ability to detect early arthritis, even before it is clinically obvious, may be quite valuable. As increasing research is aimed at prevention and reversal of early arthritis, the ability to detect arthritis prior to significant cartilage destruction is becoming increasingly important. As such, we believe the JSH ratio is a valuable diagnostic tool in the clinical setting.
A potential drawback of this study is the limited number of patients in the moderate/severe arthritis group for comparison. This is due, in part, to the nature of which patients underwent arthroscopy at our institution. Few patients with severe arthritis undergo arthroscopic exam due to the fact that these patients undergo carpectomy or fusion procedures and do not necessarily benefit from arthroscopic examination. For this reason, there are more patients in the normal and mild arthritis groups. It is possible that with a higher number of patients in the severe arthritis group, a significant difference may have been found between the mild and moderate/severe groups using the joint space height ratio in the radiolunate joint.
The JSH ratio is a novel, simple, objective method of quantifying wrist arthritis in the radioscaphoid and radiolunate joints. Compared to subjective grading, which tends to underestimate the degree of arthritis present, the JSH ratio more accurately assesses radiocarpal arthritis. While there currently lacks a standard method to radiographically grade radiocarpal arthritis, the JSH ratio represents a promising option. Future directions should focus on clinical evaluation as it correlates to objective radiographic findings as well as the implication of these findings on surgical decision making.
Footnotes
None