
Abstract
Background
Scholars have found that as a multi-facet phenomenon, religion has a complicated relationship with people's health well-being. However, current research on health and religion has left a vacuum in understanding why we observe widespread health disparities between the majority and minority religious groups.
Purpose
The present study is aimed at two purposes. First, we conduct a cross-national comprehensive examination of the relationship between religious minority/majority status and self-rated health. Second, we investigate the moderating potential of political contexts on the relationship in question.
Methods
Drawing from the 2010–2014 wave of World Values Survey, we construct an analytic sample containing about 70,000 individual cases nested within 51 countries, and apply multilevel modeling to account for the hierarchical data structure.
Results
We first find that religious minorities are less likely to report good/very good health status relative to members of majority group. However, we note that the religious minority health disadvantage is driven by a few country outliers. After exclusion of any of these country outliers from the analysis, there is no significant health difference between majority and minority groups. Moreover, we find that political contexts moderate the health effect of being a religious minority. In countries with low levels of democracy or heavy religious restriction on minority groups, people of minority groups are less likely to report good/very good health compared with those belonging to majority group. By contrast, in societies with high levels of democracy or low levels of religious restriction, the health dispartities between religious majority and minority groups become non-significant. A series of sensitivity analysis, including using multiple-imputation sample and different ways of coding key variables, provides credibility to the results.
Conclusions and Implications
This study's findings suggest that religious minorities experience health disadvantage, only when minority groups are denied of political and religious freedom. Compared with past works that mostly focused on a single or a few societies, this study provides large-scale, cross-national evidence for the issue of religious minority health. This study also adds to our understanding of how political context shapes the health impacts of religion.
Introduction
As a multi-facet phenomenon, religion has a complicated relationship with people's health well-being. When discussing multiple aspects of personal religiosity, past works tend to focus on the effects of the “Three Bs”, that is religious behavior, belief, and belonging. Studies on religious behavior have found that participation in religious activities is positively related to health status as frequent participants can obtain health benefits such as social support and coping methods (e.g., Hummer et al. 1999; Ellison and George 1994; Ellison et al. 2001; Idler and Benyamini 1997; Schieman et al. 2001; Schnittker 2001; Upenieks et al. 2018). Religious beliefs have mixed effects on individuals’ well-being. While comforting beliefs can improve mental and physical health (e.g., Ellison and Burdette 2012; Flannelly et al. 2012), some others may drive believers to experience spiritual struggle, doubt, and depression (e.g., Ellison and Burdette 2012; Ellison et al. 2009, 2013; Exline et al. 2000; Krause and Wulff 2004; Nie and Olson 2016). In addition, some studies have explored how belonging to a particular denomination such as Protestantism and Catholicism affects followers’ well-being (e.g., Ellison 1991; Ford and Kadushin 2002; Huijts and Kraaykamp 2011). The academic inquiry summarized above has demonstrated the importance of teasing out religion's multiple impacts on health.
To extend the current discussion, the present study is aimed to examine the relationship between individuals’ health and religious minority/majority status, an understudied aspect of personal religiosity. In the contemporary world, religious minority groups constitute a significant component in the ecosystem of religious landscapes in most countries, and many minority groups are faced with severe discrimination or repression (Fox 2000). Minority groups’ disadvantaged status suggests that these groups may experience high levels of stress or have limited access to health resources. Given the large size of minority groups and their disadvantaged status in many societies, our understanding of religion-health link is incomplete without exploring health disparities between religious majority and minority and the formative mechanisms behind such disparities.
The present study is aimed at two purposes. First, we conduct a cross-national comprehensive examination of the relationship between religious minority/majority status and self-rated health. A few studies have explored the health status of people who affiliate with a minority religion (Hu et al. 2017; Huijts and Kraaykamp 2011; Jasperse et al. 2012; May and Smilde 2016; Stroope and Baker 2018; Yang et al. 2019), but the research scope of these works may restrict the generalizability of their conclusions. As case studies, most of them focus on a single society such as the U.S. and China or select a single group such as Muslims and Protestants. The distinctive national context of these studied countries, along with the theological and organizational features of the selected groups, may confound the impact of religious minority/majority status. For example, we do not know if the health disadvantage of Christian minorities in China (Hu et al. 2017) is due to the majority group's hostility, government regulation, or their religious practice. To address such shortcoming, we conduct a more generic test of the relationship in question by using the 2010–2014 wave of World Values Survey data, which include societies that vary in political institutions and religious traditions.
Second, we investigate the moderating potential of political contexts on the relationship in question. In societies where the authorities respect political and religious freedom, minority groups can use legal or political means to mitigate the negative health influences conferred by their marginal status. However, minority groups in adverse political settings are more vulnerable to various forms of societal or governmental sanction, so that they may suffer greater health disadvantages. In the following sections, drawing on prior theories and research, we elaborate on potential mechanisms and set out a series of empirical expectations for religious minority/majority status and its interplay with national political contexts. Finally, we discuss our findings in light of theories of religious regulation, cultural dissonance, and religion-health link.
Literature Review
Health Disparities between Religious Majority and Minority Groups
Existing studies have suggested several mechanisms for the health disparities between religious majority and minority groups. First, minority groups may experience interreligious hostility in daily life. The worldviews and codes of behavior of religious minorities are possibly at odds with the social norms at large. Scholars argue that such cultural dissonance may force minority people to experience various forms of social sanctions such as contempt, criticism, exclusion and stigmatization (Hu et al. 2017; Yang et al. 2019; Stavrova et al. 2013; Stroope and Baker 2018). These negative social experiences likely function as chronic stressors that are adversarial to physical and mental health.
Moreover, the hostility against religious minorities may restrict the economic opportunities of minority individuals (Link and Phelan 2001). Intergroup relation studies find that people belonging to a majority group may view minority groups as competitors of economic resources such as jobs and housing (Blumer 1958; Stephan and Stephan 2000). Majority groups may take measures to limit minority individuals’ economic opportunities. These socio-economic disadvantages often translate into higher rates of illness and impairment and less access to health resources.
Built upon these theories, a limited number of empirical studies have examined the health disparities between religious majority and minority groups. Some research has found that in China, minority groups such as Christians and Muslims reported worse health than the majority group (Hu et al. 2017; Yang et al. 2019). Research focusing on Europe has shown that the health status of Protestants declines in countries dominated by Catholics (Huijts and Kraaykamp 2011). Another group of studies has found that Muslims in Western societies are subject to more stressful situations and report worse mental health than non-Muslims (Jasperse et al. 2012). In Catholic-dominated nations, participation in religious communities may lead to poor health among non-Catholics (May and Smilde 2016). In the United States, scholars have examined the health disadvantage of religious nones—people not affiliating with any religious group—relative to religious individuals (Stroope and Baker 2018).
These case studies are restricted to a single country or a single religious group, a limitation raising doubt on the generalizability of the studies’ findings. In this study, we use a cross-national dataset with major world religions included and model the health inequality between majority and minority groups, adjusting for potential confounding variables such as belonging to a particular religion. According to the mechanisms suggested in previous research, we hypothesize that:
Hypothesis 1
Religious minority status is negatively associated with individual health.
Moderation by Political Contexts
The theories we have reviewed do not suggest that being a minority by itself leads to inherent health disadvantages. Instead, whether it is intergroup hostility, marginalization and segregation, or cultural dissonance, these notions point to the underlying social context that generate minority-health disparities. Minority status is a prescribed identity and its impact on the possessors of such identity depends closely on the context that generates the definition of such identity and delineates the experiences associated with it (Yang et al. 2019; Stroope and Baker 2018). Without the institutional context that produces discrimination and cultural dissonance for minority members, it is possible that a minority health disadvantage does not exist.
Among different types of contexts, political context may induce the most salient structure-level forces on minority health. Political repression may escalate the levels of criticism, discrimination, or other forms of social sanctions against minority groups (Fox 2000). However, when political systems bestow minority groups with political and religious freedom, these groups may suffer fewer hostilities and be more capable of protecting their interests. Understanding the context that leads to potential health disparities between religious majorities and minorities is an urgent question. Therefore, the current study aims to investigate how political contexts moderate the extent of minority-health disparities.
This study focuses on two aspects of political contexts, the levels of democracy and of state restriction on religious minorities. Although democracy and restriction measures are correlated (r = − 0.59 in our study), democracy and restriction on religious minorities are conceptually distinctive. Democracy refers to the institutional arrangements that channel citizens’ opinions, regardless of their religious affiliation, into the political process (Lipset 1994), while minority restriction means the policies or laws that limit religious gathering, proselytization, and organization of minority groups (Fox 2000). Therefore, we decided to analyze the moderating effects of democracy and minority restriction respectively.
While the shaping effect of democratic institutions on health has been well documented (Barnish et al. 2018; Lu and Yang 2020; Mackenbach et al. 2013; Muntaner et al. 2011), such institutions’ meaning for religious minorities’ well-being is under-studied. In this research, we argue that democratic institutions may alleviate the cultural, economic and health disadvantages of minority individuals. According to theories on democracy (Dahl 1971; Lipset 1994; Seabright 1996), first, the political arena is open for citizens to articulate interests and voice grievances. Minority groups may exert influence on politicians to advance their interests or seek relief. Moreover, the legal system of democratic regimes protects minority groups’ rights to express and follow their distinctive values and code of behavior. This is because consolidated democracies guarantee citizens—regardless of their religious faiths—the freedom of association and speech. In other words, through empowering minority groups to pursue their own ways of life, democratic institutions may narrow the health gap between majority and minority people. By contrast, in societies with weak democratic institutions, the lack of political rights makes minority groups particularly vulnerable (Magaloni and Kricheli, 2010; O'Donnell and Schmitter, 2013). Minority groups may find it difficult to resort to the legal system when facing discrimination or persecution from the religious majority. Also, the mechanisms of inputting concerns and opinions into the political process are ineffective or blocked in these societies. There are few avenues for minority groups to express interests or grievances. Thus, nondemocratic regimes may exacerbate the extent of daily hostility, social disorganization, and cultural dissonance, with worse health status among minority groups as a result.
State restriction on minority religions exists widely in the contemporary world (Finke et al. 2017; Schleutker 2019) and can generate varying levels of inter-religion tensions, from daily bias to civil war (Fox 2000). Past works have noted that high levels of religious regulation impair the life satisfaction of people who participate in religious activity (Elliott and Hayward 2009; Hayward and Elliott 2014). Moving beyond these studies, we argue that state restriction on the religious minority is another political factor that may shape minority groups’ social environment, religious identity, and health. First, according to Beckfield's institutional theory (2018), a polity may generate health disparities through transferring health resources for a majority group at the expense of religious minorities. Thus, political regimes that are hostile to minority religions may limit the amount of health care resources for certain minority groups, deepening the divide between minority and majority groups. Second, state restriction may escalate majority groups’ discrimination against a religious minority. In countries with higher levels of government restriction, cross-religion tensions are more likely to happen (Grim and Finke 2007). According to Grim and Finke's research, the state may rely on religious majority-related social forces to implement restriction measures, or the state may embolden the discriminatory action of other religious groups, which exploit the vulnerability of minority groups. Third, state restriction likely interrupts religious activities that are health-promoting (Fox and Tabory 2008). Participation in religious activities is found to be closely related to better health outcomes. People who regularly participate in religious activities can obtain social support from religious communities, reduce sedentary time, subscribe to pro-health religious norms and learn religious coping methods for uncertainty and illness, all of which may promote their overall health (Eliassen et al. 2005; Krause et al. 1999; Lim and Putnam 2010; McCree et al 2003; Yang et al. 2017; Seybold 2007; Schjoedt 2009). Minority individuals will hardly reap the health benefits of religious participation if the state restricts access to religious services and punishes those who disobey the rule. By tracing back to these conceptual frameworks in relation to minority status and political contexts, the current study proposes two hypotheses about the moderation effect of political contexts:
Hypothesis 2
The negative health effects of religious minority status are weaker in more democratic countries. This is the palliative role of democracy.
Hypothesis 3
The negative health effects of religious minority status are stronger in countries with more severe minority restriction. We consider political restriction an aggravating force for minority-health disparity.
Methods
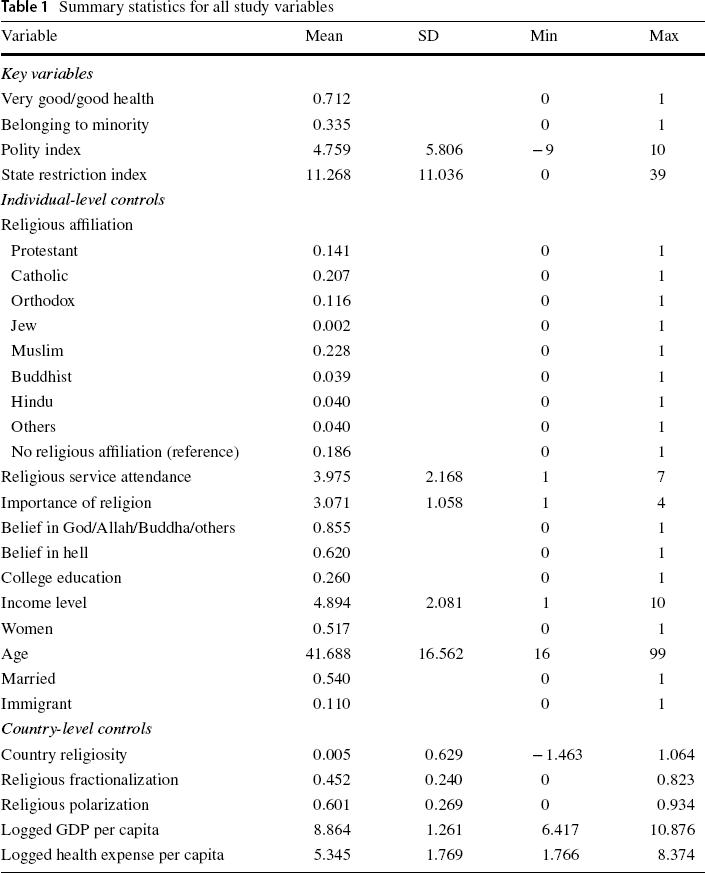
Summary statistics for all study variables
Outcome Variable
Self-rated health has been demonstrated to be a valid and reliable assessment of individuals’ overall health status and has been widely used in previous research focusing on individuals’ health (e.g., Boardman 2004; Ferraro and Farmer 1999; Frankenberg and Jones 2004; Idler and Benyamini 1997; Jylhä 2009). In a review of self-reported health measures, self-reports are found to exceed the predictability of physician assessment (Ferraro and Farmer 1999). The self-rated health question in the sixth wave of WVS is asked as, “How would you describe your state of health these days?” Reversed coded responses are (1) “poor,” (2) “fair,” (3) “good,” (4) “very good.” The majority of existing studies have classified the responses into a binary variable with “good” and “very good” coded as 1 and “poor” and “fair” coded as 0 (e.g., Idler and Benyamini 1997; Stroope and Baker 2018). Following this approach, we report logistic model results as the main findings. As part of sensitivity analysis, we estimated linear models which treated self-rated health as a continuous variable. The linear models produced substantively identical results as the logistic ones. In addition, we estimated ordered logistic models with an ordinal health variable, which yielded similar results to the logistic models. However, we noted that the proportional odds assumption was violated. We thus chose to focus on the findings of logistic and linear regressions. Appendix Tables 3 and 4 show the shares of respondents who reported good/very good health for each religious group per country.
Key Predictors
Religious minority status is the key individual-level independent variable. According to the religious composition of each country, we classified respondents into two groups, religious majority and religious minority. There were nine categories of religious identity in the WVS from which respondents were allowed to choose: Protestant, Catholic, Orthodox, Muslim, Buddhist, Jew, Hindu, other religions, and religious none. Using the original nine categories, we calculated the sizes of each religious group per country based on the proportion of respondents. The religious group that was the largest in its country was labeled as the majority religion, while the others were treated as minority religions. We coded respondents belonging to minority religions as 1, and those belonging to majority religion as 0.
The level of democracy of each state is measured by the polity index, drawn from the Polity IV project. We then compiled the Polity IV project data with WVS at the state-level. The Polity IV project describes and summarizes the political characteristics of all regimes that have ever existed since the eighteenth century. Researchers of the project focus on multiple dimensions of a regime, the competitiveness of executive recruitment, the openness of executive recruitment, the constraints on the chief executive, and the competitiveness of political participation. Quantitative comparative political studies have heavily relied on the information provided by the project (e.g., Muntaner et al. 2011; Schofer and Fourcade-Gourinchas 2001). The index is between − 10 (strongly autocratic) to 10 (strongly democratic). This study used the index of the year 2010.
State restriction on minority religions is constructed according to the information drawn from the Religion and State project (2014), which provides data about government involvement in religion for 175 countries (Fox 2008). From this data, we selected 27 variables that capture specific measures restricting minority religions, particularly the measures that have implications on the health status of minority groups. The full list of 27 variables is provided in Appendix Table 7. Each of the variables ranges from 0 (no such restriction) to 3 (severe restriction). We combined these variables to create an index. After integration with the WVS data, the state restriction index in the analytic sample ranges from 0 to 39, with a larger score indicating a higher restriction level.
Control Variables
We controlled for several religious variables that may confound the association between religious minority/majority status and health. Religious affiliation was included in the models (Protestant, Catholic, Orthodox, Muslim, Buddhist, Jew, Hindu, other religions, and religious none as the reference group). As an indicator of participation in religious activities, religious service attendance ([1] “never” to [7] “more than one a week”) is controlled for. We included beliefs in God/Allah/Buddha/other divinities (believing = 1, not believing = 0) and in hell (believing = 1, not believing = 0) in the models. Also, we controlled for the self-reported importance of religion (from [1] “not important at all” to [4] “very important”).
In addition, we controlled for common socio-demographical variables that were found to be associated with health (Deaton 2013; Elo 2009): Age (coded in year), sex (women = 1, men = 0), marital status (married = 1, else = 0), college education (having college education = 1, not having college education = 0), income level (ranging from 10, highest income, to 1, lowest income), and immigrant status (respondent's father, mother, or self is an immigrant = 1, otherwise = 0).
In terms of country-level control variables, we (1) included 2010-year Gross Domestic Product (in US dollar and natural log form) from World Bank data, as the associations between the economic development and health indicators are well documented in the literature (Cole 2018). (2) The quality of the health care system matters for people's health. We measured the quality of the health care system by using 2010-year health expenditure per capita (in US dollar and natural log form), which is provided by World Bank. (3) Country-level religiosity has been found to be influential on the religion-health link (Stavrova 2015; Stavrova et al. 2013). To measure country-level religiosity, we created a principle-component factor of religious service attendance and religious importance and then calculated the country mean of this factor. (4) Religious composition of an area not only has consequences on religion and politics relationship (Grim and Finke 2007), but also shapes the well-being of people living in that area (Upenieks et al. 2018). Following previous research, we controlled for religious fractionalization and polarization, two types of religious diversity which are found to influence people's health differently (Lu and Yang 2020).
Plan of Analysis
We used multilevel modeling to incorporate both individual- and country-level variables as well as cross-level interaction. In this study, individual respondents were nested within different countries. Using ordinary regression violates an assumption of ordinary logistic regression in which cases should be independent of each other and therefore miscalculates the errors. Multilevel modeling is thus appropriate for this study because it allows for simultaneous consideration of multiple-level variables. In the models, the intercept is set to vary across countries, meaning that country-mean probabilities of reporting good/very good health are different. We also allow the slope of religious minority variable to vary, so the health effects of religious minority would change across countries.
Two of our hypotheses are aimed at revealing the moderation effect through multiplicative interaction terms. When the dependent variable is binary and logit regression is used to estimate the model, the (in)equality of the regression coefficients between two groups (e.g., minority vs. majority) does not imply the (in)equality of marginal effects on the probability. Therefore, beyond estimating the coefficients of interactive terms, we also show the comparison of the predicted probability between groups, as suggested by the recent methodology works (Long and Mustillo 2021; Mize 2019).
A major source of missing data originates from the state-level information of nine countries or regions (Kuwait, Tunisia, Morocco, Qatar, Egypt, Hong Kong, Taiwan, Palestine, and Yemen).1 Thus, the inclusion of these variables in models will delete 10,529 respondents from the countries or regions, around 11.8% of the whole sample. Besides, there are 9,866 more missing cases in the remaining sample, 11.5% of the whole data. We addressed the missing values in two ways. The first method is listwise deletion of all the missing values. This is a common strategy adopted by most researchers who use the WVS data (e.g., Huijts and Kraaykamp 2011; Lu and Yang 2018; Olson and Li 2015; Ruiter and De Graaf 2006; Stavrova 2015), which resulted in an analytic sample of 65,605 individual cases. The second method is a combination of listwise deletion and multiple imputation. We dropped the cases from the above nine societies. The missingness of the data from these societies may not depend on the observed cases, so it is not appropriate to imputate for the missing data. For the missing values in the remaining sample, we used multiple imputation. Following the widely practiced procedure, we excluded those observations with missing data on the dependent variable in estimating the models. The multiple-imputation sample contained 73,145 cases. We find that the results based on the listwise-deletion sample are substantially similar to the those with the multiple-imputation sample. We present the listwise-deletion results in the main table and the multiple-imputation results in the Appendix Table 8.
Results
Main Findings
We first run an unconditional model on the dichotomous health variable without any covariates (Model 1). The intraclass correlation (ICC)2 is about 0.133. This means that around 13% of the total variance in health can be attributed to between-country differences. Because there is substantial variation in individual health status across countries, it is appropriate to use multilevel regression models to account for the between-country variance along with the within-country variance.
Model 2 is a multilevel logistic model of the health variable regressed on all study variables. Model 2 explains 54.3% of country-level variance.3 It shows that religious minority status is negatively associated with having good health (β = − 0.101, SE = 0.041). The finding suggests that minority individuals are less likely to report good health relative to those belonging to the majority religion. In terms of the effect size, religious minorities are 10% less likely to report good or very good health, relative to the religious majority. We compare the effect size of religious minority status with that of an important control variable, marriage status. Married people are 22% more likely to report good or very good health (β = 0.199, SE = 0.021), relative to those unmarried. Compared with the marriage variable, religious minority status's effect size looks modest. This finding is line with Hypothesis 1 that expects negative health effects of religious minority status.
Model 3 estimated an interaction between belonging to minority religions and democratic level, adjusting for the individual- and country-level confounding variables. This interaction coefficient is significantly positive, indicating that the negative effects of belonging to minority religions are mitigated in more democratic societies. We calculate the effect size of religious minority in different political contexts. In countries with low polity scores (one standard deviation below the mean), religious minorities are 21% less likely to report good or very good health. This is a substantial gap when considering the effect size of marriage. By contrast, religious minorities are only 2% less likely to report good or very good health in countries with high polity scores (one standard deviation above the mean). Figure 1 displays the predicted marginal effects of religious minority across polity scores. The y-axis is the estimated marginal effects of religious minority status and the x-axis is the the polity score. As moving from low polity scores (less democratic) to high polity scores (more democratic), the negative effects of religious minority become smaller. The finding provides support to Hypothesis 2 on the moderating effect of democracy on the association between religious minority status and health outcome.
The predicted marginal effects of religious minority status on self-reported health across polity score with 95% confidential intervals (Model 3 of Table 2)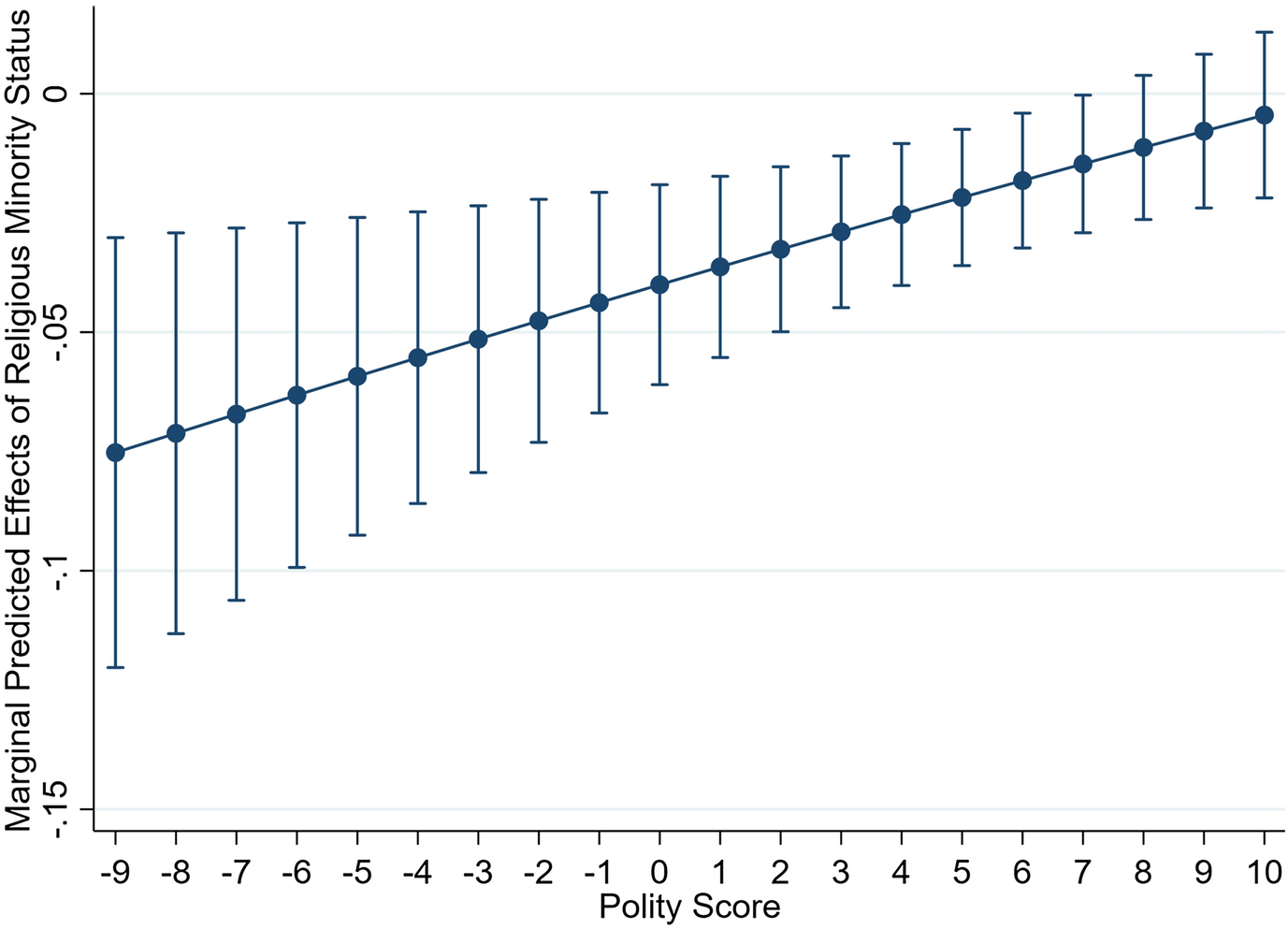
Model 4 shows that religious minority status significantly interacts with state restriction index. The effect size of religious minority status changes substantially across different levels of state restriction. In societies characterized by high government restriction (one standard deviation above the mean), religious minorities are about 19% less likely to report good or very good health. In societies with low restriction scores (one standard deviation below the mean), religious minorities are 2% less likely to report good or very good health. Figure 2 plots such interplay with all control variables set at their respective means. The y-axis is the estimated marginal effects and the x-axis is the the religious restriction score. The graph shows that the predicted marginal effects of religious minority increase as the religious restriction becomes more severe. Thus, in societies with high levels of restriction, there are substantial health disparities between majority and minority people. We find evidence for Hypothesis 3, which expects state restriction leading to health disadvantages among religious minorities.
The predicted marginal effects of religious minority status on self-reported health across religious restriction score with 95% confidential intervals (Model 4 of Table 2)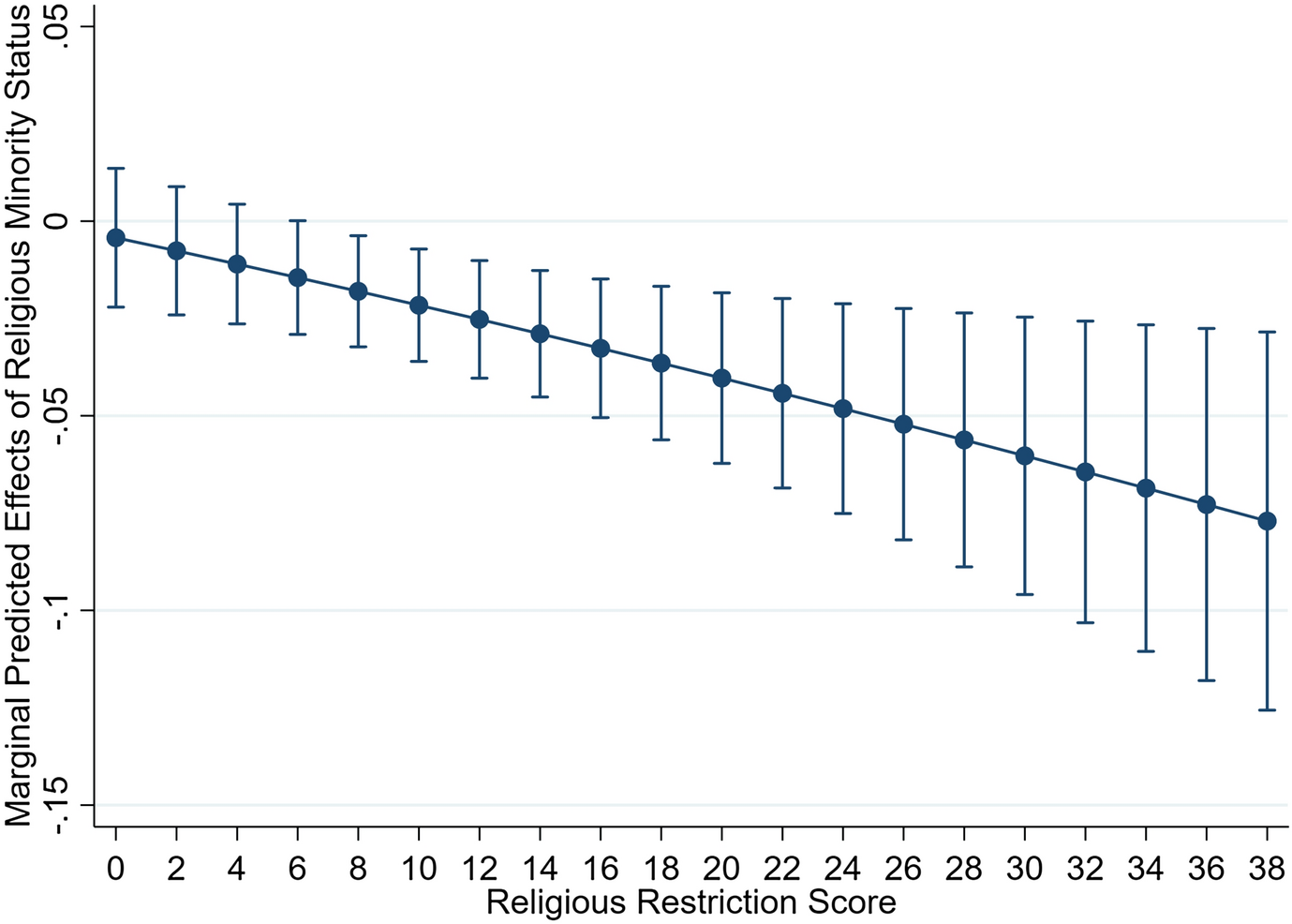
Robustness Test
The limited sample size at the country-wave level, around 50 cases, makes the analysis vulnerable to the influence of potential outliers. To check this possibility that some country cases are too influential, we did a drop-one-at-a-time analysis in which we repeated the models with each country-wave case being dropped at a time. If excluding any particular country case substantially alters the findings, it would mean that this influential outlier drives the findings. If not, it would provide evidence of the robustness of the results.
We focused on investigating whether the statistical significance changed with the exclusion of one country case at a time. For the effect of belonging to minority religions on self-rated health, we found that after excluding any one of 12 countries,4 such effect became non-significant. As this finding suggests, the negative effect of belonging to minority religions was driven by some country-level cases and after we removed any one of these countries from analysis, there was no significant difference between the majority and minority people in the remaining sample. The finding from the drop-one check cautions against Hypothesis 1. However, for the interaction effects of democracy and state restriction on minority religions, we found no evidence that such exclusion leads any interaction coefficient to become non-significant. Thus, the drop-one check provides credibility to Hypothesis 2 and 3 that expect the moderating effects of political context variables.
Multilevel logistic regression modeling on self-rated health (Individual N = 65,605; Country N = 51)
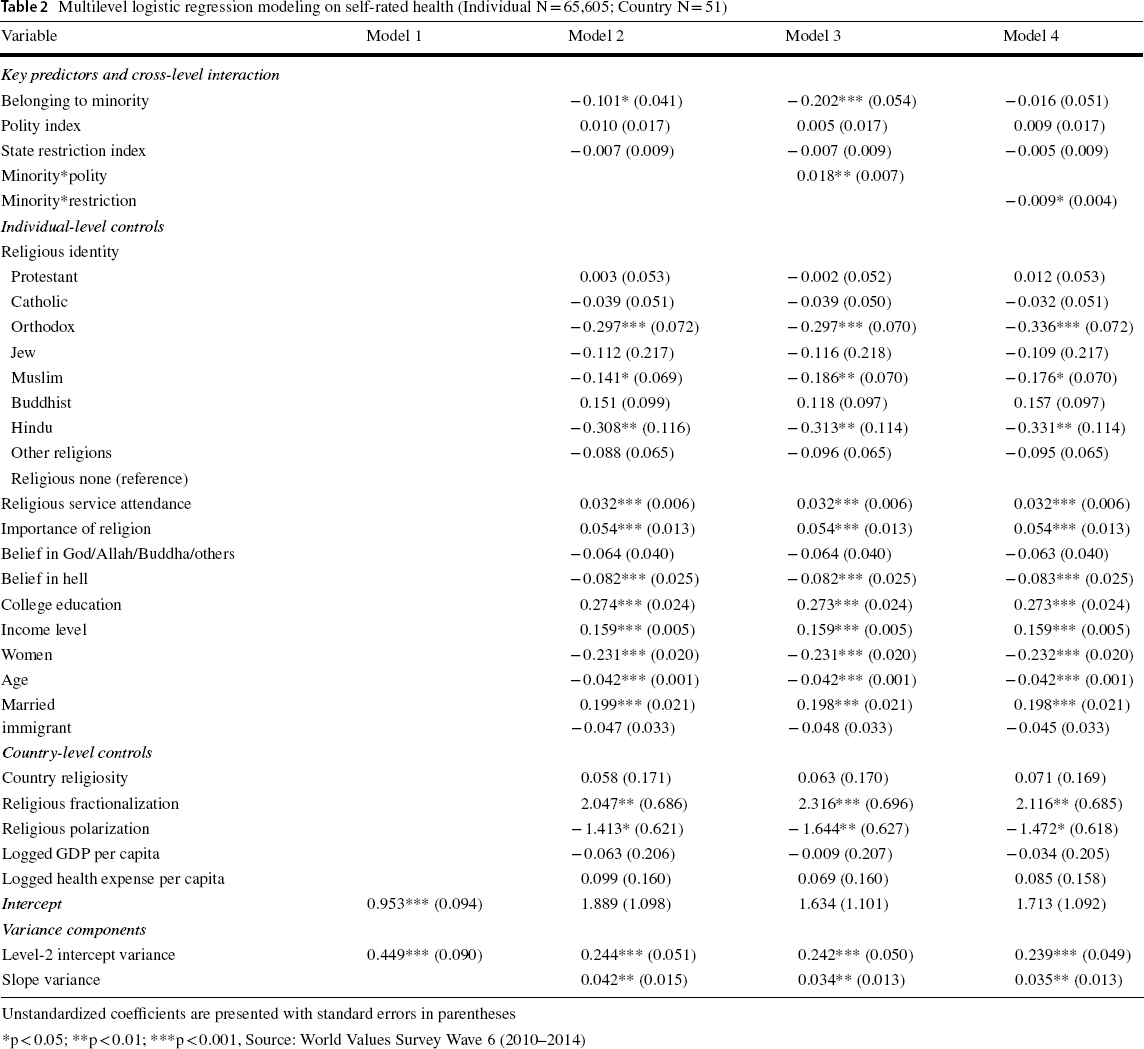
Unstandardized coefficients are presented with standard errors in parentheses
*p < 0.05; **p < 0.01; ***p < 0.001, Source: World Values Survey Wave 6 (2010–2014)
We re-estimated the models by modifying the operationalization of majority religion. As discussed in the methodology section, we coded the religious group with the largest size as majority religion for each society. However, in some societies the largest group does not have an overwhelming size and the population share difference between the largest group and the second largest one is small. In Singapore, for example, the largest group is Buddhism with 27% of respondents from the country, while the second-largest is religious nones with 19%. In a context like Singapore, it may be difficult for the largest religious group to generalize its own values as social norms from which deviation will incur discrimination and stigmatization. To address this problem, we reckon that the majority religion should have a considerable size to shape social norms and cause cultural dissonance among other groups. Therefore, we re-defined majority religion as the religious group which has more than 50% of respondents for each society. We then dropped from the analysis the countries without any such religious group.5 As shown in Model 3 and 4 of Appendix Table 6, the changes do not substantially alter the core findings.
When coding the religious minority status variable, we chose to combine Sunni and Shiite Muslims (two major subgroups of Islam) into one group. One may argue that in a Sunni-majority country, a combination of Sunni and Shiite Muslims masks the marginal status of the Shiite group, leading to miscalculation of the health gaps between religious majority and minority. The decision to combine all Muslim respondents is based on the fact that most Muslim respondents in the WVS data did not indicate which specific branch of Islam they belonged to. We identified 15,290 respondents as being affiliated with Islam, among which 83.17% reported themselves as “Muslim”, 16.66% as “Sunni”, and 0.18% as “Shiite”. Using the WVS data for individual information, we need to classify all Muslim respondents into a single group.
Although we had to follow the WVS’ classification of religious identity, we conducted sensitivity analysis by dropping the countries with a mixture of Shiite and Sunni Muslims. Most Shiite Muslims (which is the smaller branch) are living in a few countries. In our analytical sample, there are only three countries (Iraq, Lebanon, and Pakistan) that have sizable shares of both Sunni and Shiite Muslims based on the official census. If the combination of Sunni and Shiite Muslims really distorts the model results, we should expect substantial changes in the findings after removing these countries from the analysis. As Model 5 and 6 of Appendix Table 6 show, the key findings persisted in the models without the countries where Shiite and Sunni Muslims coexist. This test suggests that grouping together Sunni and Shiite Muslims do not cause a severe problem for the purpose of our study.
There are a few minority respondents in some country samples. For instance, only 6 out of 1200 respondents from Algeria reported belonging to minority religions. The results may vary if the analysis is restricted to countries with a significant number of minority respondents. We first remove from the analysis the country samples in which minority respondents are less than 50. Eight country samples are excluded: Algeria, Azerbaijan, Iraq, Jordan, Libya, Pakistan, Thailand, and Turkey. Model results without the eight country samples are presented in Model 1 to 3 in Appendix Table 9. Second, we limit the analysis to the country samples with at least 100 minority respondents. Another four country samples are excluded: Armenia, Georgia, Poland, and Uzbekistan (Model 4 to 6 in Appendix Table 9). According to these models, religious minorities are less likely to report good/very good health than religious majorities. The health gap between religious majorities and minorities depends on the Polity index and religious regulation index. Therefore, the results are similar to that based on the full sample.
As part of a robustness check, we combine the WVS 2005, 2010, and 2017 waves to examine the link between religious minority status and self-report health. The three-wave models (Appendix Table 10) yield substantially similar results. The minority status is negatively associated with good/very good health. The effect of minority status is conditioned on the Polity index and religious regulation. The three-wave model findings provide credibility to this study's core argument.
Discussion
Summary of Results
We have two goals in this study. First, moving beyond existing case studies, we attempt to comprehensively test the relationship between individuals’ religious majority/minority status and self-reported health. We integrate the 2010–2014 wave of World Values Survey with other national datasets, creating a cross-national representative sample containing 51 societies. A series of analysis provides mixed findings: the full-sample models find that minority individuals are less likely to report good health, but the robustness check shows that such result is influenced by outlier societies. After dropping outliers that are too influential, we find that there is no significant difference between the majority and minority individuals regarding their health status. The results does not fully support Hypothesis 1, which expects a negative association between religious minority status and self-rated health.
The second goal of this study is to explore if the health gap between religious groups depends on political contexts. We take into consideration two aspects of political contexts, democratic level and state restriction on religious minorities. The model results show that in countries that are democratic or have few restrictions on minority groups, minority respondents have similar probabilities of reporting good health as majority ones. However, adverse political settings, which are characterized by weak democratic institutions or harsh restriction measures, are found associated with greater health disparities between minority and majority individuals. These findings lend support to Hypothesis 2 and 3, which argue that democracy and religious regulation respectively moderate the association between religious minority status and self-rated health.
We argue that the extent of health gap between religious groups is politically bounded. Democratic institutions enable people to use legal or political means to offset the harmful influence, or to prevent discrimination or any other social sanctions against minority groups. Minority groups living under nondemocratic regimes lack an institutionalized mechanism to express grievances and protect interests. Moreover, state restriction may reduce health resources available to minority groups, make them more vulnerable to other social forces, or interrupt health-benefiting services of minority communities, all of which escalate the degree of culture dissonance perceived by minority people.
Case Discussion
We select Brazil and China to discuss how this cross-national comparative research corresponds to previous cases studies. A brief discussion of religion and health in the two countries helps illustrate how political institutions influence the health gap between majority and minority groups. In China, most people do not affiliate with a religious organization, though they may conduct some religious or spiritual practices; Among people with a clear religious affiliation, Buddhists are the largest religious group, while Christians and Muslims are minorities (Yang 2006). The authoritarian party-state heavily monitors religious activities such as prohibiting religious organizations that are not registered, controlling personnel and financial affairs within official religious organizations, and limiting civic engagement of religious groups. Such political pressure exerted upon minority groups have health consequences. Compared to people without religious affiliation, minority groups are more likely to report depression (Hu et al. 2017) and have lower levels of self-rated health (Yang et al. 2019). This study's findings align with the literature. Appendix Table 4 summarizes the respective shares of respondents who reported good/very good health of minority and majority groups. The share of minority respondents who reported good/very good health (60.6%) is smaller than that of religious majority respondents (69.5%) in China. The health disadvantages of minority groups in China, as noted by previous research, may be due to the social and political environment influencing minority members’ daily lives.
By contrast, Brazil has a very different religious and political landscape. This country was once dominated by Catholicism, but recent decades have witnessed a fast growth of Pentecostal Protestantism (Miller 2007). The development of Protestantism in Brazil has not encountered the political limitations that Protestant churches have faced in China. Past works have noted the health benefits that Protestant churches bring to local followers (Wood et al. 2007). Thus, scholars have not found health disadvantages associated with religious minority status in Brazil, suggesting that minority and majority members might have similar health statuses without religious and political restrictions. As shown in Appendix Table 4, the share of minority respondents who reported good/very good health (71.0%) is very close to that of majority respondents (70.1%) in Brazil. This study's finding echoes previous research. Generally, The case studies of Brazil and China demonstrate that political context shapes the religion-health link. Political restriction may lead to the health disparities between religious majority and minority groups. However, when political restriction is absent, such health disparities may decline.
Limitations
There are some limitations in the study. One limition is the subjective nature of the self-rated health variable. Although past works have proven that self-rated health is a valid indicator, an objective measure of health should better reveal the relationship between religious minority status and health outcome. However, we lack cross-national data that contains both individual religiosity and objective health information. We encourage additional research into this issue when such data is available. In addition, we discussed several potential mechanisms for the relationship between religious minority status and health disadvantage. However, we cannot directly test these mechanisms based on the data. Future research should examine these mechanism when cross-national data provides needed information.
Conclusions and Implications
Our research contributes to the knowledge of health outcome of belonging to religious minority groups. We find evidence that minority religious groups report worse health status than majority groups, of which the interpretation needs caution due to the influence of a few country outliers. By using a large-scale, cross-national representative sample, this study provides nuance to the knowledge of this issue. Also, we find that greater health disparities between the groups are associated with higher levels of religious and political repression. When minority groups are denied of political and religious freedom, the health gap may widen.
As an important implication of this study, existing case studies’ findings on religious minority and health outcomes need cautious interpretation (Hu et al. 2017; Huijts and Kraaykamp 2011; Jasperse et al. 2012; May and Smilde 2016; Stroope and Baker 2018; Yang et al. 2019). Understandably, these case studies tend to focus on certain situations where the religious majority has noticeable health advantages relative to the religious minority. However, when examining this question at a larger scale with global data, our analysis suggests that some country cases are influential on the relationship between religious minorities and self-rated health.
This study also contributes to a broader literature on religion and health. Scholars have generally agreed that multiple aspects of personal religiosity affect health outcomes differently. Most of the health and religion literature have emphasized the health implications of religious behavior, belonging, and beliefs (e.g., Ellison et al. 2001; Ellison and Burdette 2012; Exline et al. 2000; Flannelly et al. 2012; Ford and Kadushin 2002; Huijts and Kraaykamp 2011; Krause and Wulff 2004; Nie and Olson 2016; Schieman et al. 2001; Schnittker 2001; Upenieks et al. 2018). This study's findings add to this academic inquiry by exploring whether and where belonging to minority religions adversely shapes one's overall health.
Another implication of this study is related to an emerging research area focusing on political determinants of individual health. Scholars have recently paid more attention to the health consequences of democracy, the welfare state, women's political representation, and other political factors (Barnish et al. 2018; Mackenbach et al. 2013; Muntaner et al. 2011; Lu and Yang 2020). The growing attention to macro context reflects an academic belief that a comprehensive understanding of micro-level physiological phenomena necessitates the analysis of the underlying fundamental social process (Beckfield 2018). Specifically, studies have pointed out that democratic institutions render government agencies to be responsive to citizens’ health and economic needs, thus improving population health. Our study adds to the literature by showing that democracy moderates the association between religious majority/minority status and individual health. Moreover, we also find that state restriction on the religious minority, a political factor rarely examined in health and politics literature, matters for the health outcome of minority groups.
Footnotes
Funding
This research is funded by the National Social Science Fund of China, grant number 22CSH005.
1
Specifically, there is no observation on religious service attendance in Kuwait, Qatar, and Morocco; religious affiliation is missing in Kuwait, Qatar, and Egypt; beliefs in God/Allah/Buddha/other and in hell are missing in Palestine, Kuwait, Qatar, Tunisia, Egypt, and Yemen. In addition, Polity IV project does not include Hong Kong and Palestine. World Bank data provides no information on Taiwan and Yemen.
2
0.449/(0.449 + π2/3) = 0.133. For a multilevel logistic regression model, the within-cluster variance (level-1 individual variance) is assumed to follow a standard logistic distribution, which is equal to π2/3, or approximately 3.29.
3
(0.449-0.244)/0.449 = 0.543.
4
These countries are Rwanda, China, Malaysia, Kazakhstan, Philippines, Uzbekistan, Georgia, Libya, Cyprus, Peru, Haiti, and Belarus.
5
In the analytic sample, there are eleven countries without any religious group reaching the 50% threshold, which are Australia, Cyprus, Germany, Haiti, South Korea, New Zealand, Nigeria, Singapore, United States, South Africa, and Trinidad and Tobago.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Springer Nature or its licensor (e.g. a society or other partner) holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.