
Abstract
OBJECTIVE: The study goal was to evaluate the effects of hyperbaric therapy on the auditory and vestibular function of guinea pigs compromised by perilymph fistula (PLF).
METHODS: Twenty-four pigmented guinea pigs underwent induction of bilateral eustachian tube dysfunction before the creation of a unilateral PLF. Half of the animals were randomly assigned to receive immediate hyperbaric compression treatment of 4 “dives” each. Hearing was tested electrocochleographically, and signs of vestibulopathy were recorded before and after compression.
RESULTS: After accounting for the effects of PLF, compression was not associated with significant hearing loss (P = 0.5411). Vestibulopathy was seen only in ears with PLF, and its incidence was similar for compression and noncompression groups.
CONCLUSION: Hyperbaric compression does not compromise auditory or vestibular function in guinea pig ears with experimental PLF.
SIGNIFICANCE: Our observations support the relative safety of recompression in patients with PLF.
To date, there have been no published reports linking recompression therapy in the presence of a perilymph fistula to adverse sequelae. Anecdotal reports have described patients with PLF who have sustained no worsening of their cochlear or vestibular function with recompression. 2,6,7 Only one abstract, for which the article has not been published, has described the safety of recompression after creation of PLF in an animal model. 8 The purpose of this study was to evaluate the effects of compression therapy on the auditory and vestibular function of ears compromised by eustachian tube dysfunction and PLF in the guinea pig model.
MATERIALS AND METHODS
Experimental Design
The experimental protocol was approved by the University of Florida Animal Care and Use Committee (Protocol No. B197). This study was performed in accordance with the Public Health Service Policy on Human Care and Use of Laboratory Animals, the National Institutes of Health Guide for the Care and Use of Laboratory Animals, and the Animal Welfare Act. Twenty-four adult pigmented guinea pigs (weight, 500 to 1000 g) were used. All animals underwent induction of bilateral eustachian tube dysfunction to predispose barotrauma, followed by electrocochleography to assess hearing, before a unilateral surgical fenestration of the round window. The opposite ear served as an internal control in each animal. Half (n = 12) of the animals were randomly assigned to receive immediate hyperbaric compression, and the other 12 served as noncompressed controls. Electrocochleography was repeated along with observation for signs of vestibulopathy after fenestration and compression and 1 week after surgery to evaluate the effects of compression on ears with PLF. All animals were then deeply anesthetized and killed.
Surgical Technique
Anesthesia was achieved with an intramuscular injection of ketamine (100 mg/kg) and xylazine (5 mg/kg). Lidocaine 1% was injected subcutaneously for local anesthesia. A prophylactic antibiotic (enrofloxacin 10 mg/kg) was administered preoperatively. Thermal support was provided during all interventions.
Eustachian tube dysfunction was induced by gently scraping the mucosa around the tube orifice with a right angle probe, introduced across the soft palate. The bullae and skull were exposed via a postauricular approach. 9 Indwelling electrodes were implanted in the anterior epitympanic recesses bilaterally and over the snout for serial electrocochleography. A nylon electrode receptacle was secured to an anchoring screw on the skull dorsum with dental acrylic. Under microscopic visualization, the round window membrane was fenestrated with a 30-gauge needle. If there was more than 5 dB difference in baseline click-evoked auditory thresholds, the ear with the better thresholds was fenestrated, to allow more dynamic range for assessing change in thresholds. The wound was closed before compression.
Auditory Testing
Hearing was tested using click and tone pip-evoked electrocochleography. Auditory signals were generated, and the responses were averaged using an auditory electrophysiology workstation with SigGen and AeP software and hardware (Tucker-Davis Technologies, Gainesville, FL). Sound was produced by a standard transducer (model ER-2; Etymotic Research, Elk Grove Village, IL) and introduced via an earphone tube carefully placed in the external auditory canal. Thresholds to clicks, 4 kHz, 8 kHz, and 16 kHz were determined by decreasing sound intensities by 5-dB increments from a maximum stimulus of 100 dB until the waveform was lost and then raising the stimulus by 5 dB until a reproducible waveform was restored. The investigator was blinded to the animals' treatment group and prior auditory data at the time of the 1-week postoperative testing.
Diving Profile
Immediately after surgery and electrocochleography, anesthetized animals underwent 4 hyperbaric compression “dives” in a thermally controlled certified chamber. Carbon dioxide levels were maintained using lime crystals. The dive profile consisted of descent to 3 atmospheres of absolute pressure (66 feet of seawater) over a 2-minute period, maintenance at 3 atmospheres for 2 minutes, ascent to ambient pressure over 2 minutes, and then maintenance at ambient pressure for 2 minutes. This sequence was repeated 3 times for a total of 4 “dives” within 30 minutes. The value of 3 atmospheres was chosen because that is the depth used in the treatment of decompression sickness. 10
Vestibular Assessment
During the postoperative period, all animals were monitored for signs of vestibular disorder, including spontaneous and positional nystagmus, ataxia, and head tilt or abnormal posture. Vestibular signs were recorded as present or absent. The investigator was blinded to the animals' treatment group.
Barotrauma Assessment
Otomicroscopy was performed on all animals before the final electrocochleography. Presence of barotrauma was indicated by middle ear inflammation, effusion, or tympanic membrane perforation.
Statistical Analysis
To determine whether barotrauma had a significant effect on hearing, a 2-way multivariate analysis of variance (MANOVA) was used to test for differences in the thresholds measured at each frequency immediately after creation of the PLF and those measured 7 days postoperatively among the 4 groups of ears (+PLF, +compression). A second MANOVA was performed on the 2 groups of ears receiving compression (+PLF), comparing the thresholds measured immediately after creation of a PLF with those measured immediately after compression. Wilke's lambda test determined whether there was a statistically significant change in the distribution between groups that are multivariate.
Evidence of middle ear barotrauma in ears with and without compression
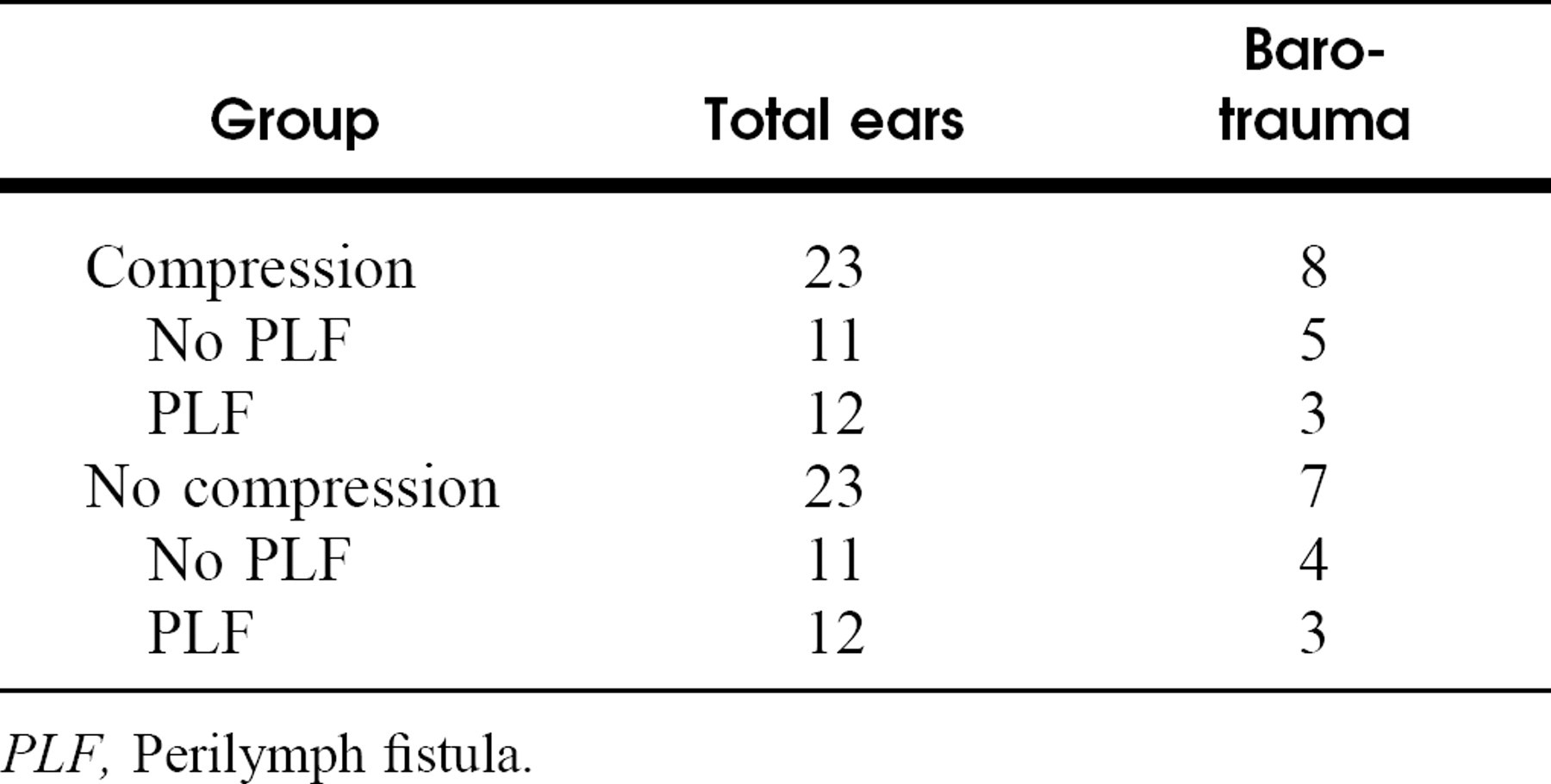
PLF, Perilymph fistula.
RESULTS
All animals tolerated electrocochleography, PLF, and diving conditions well. Two animals, one in the compression group and one control, developed severe unilateral postoperative otitis externa in their nonfenestrated (control) ears that occluded the external auditory canal and resulted in a profound conductive deficit. The affected ears were excluded from analysis, leaving 11 nonfenestrated ears in both the control and test groups.
Postoperative middle ear pathology was recorded in all ears and did not differ significantly among groups. Animals in the control group (no compression) incurred as many middle ear complications as did those in the compression group (Table 1). PLF ears experienced similar middle ear complications to nonfenestrated ears, regardless of compression status. Tympanic membrane perforation was found in only one ear, with PLF, that was subjected to compression.
Auditory-evoked thresholds were significantly higher in PLF ears than in non-PLF ears for clicks and all frequencies of tone pips (Figs 1 to 4). Presence of middle ear pathology did not correlate with auditory thresholds. Of the 8 PLF ears with the most pronounced auditory decline (ie, 7-day click thresholds ≥100 dB), only 2 had concurrent middle ear effusions. The differences between thresholds measured immediately after induction of PLF and those measured 7 days postoperatively among the 4 groups of ears (+PLF, + compression) were found to be insignificant at each frequency (P = 0.0551) (Figs 1 to 4). Within the compressed ear groups, thresholds measured immediately after PLF and immediately after compression were also found to be similar (P = 0.5411). All ears, even controls (no compression, no PLF), had worse thresholds at 1 week than at the initial evaluation.
The rate of vestibulopathy was equal between compression and noncompression groups, with most cases of vestibulopathy resolving by day 7 (Table 2). Of the 4 animals experiencing late vestibulopathy, only one had microscopically visible middle ear pathology (effusion). Of the 8 ears with the most pronounced auditory decompensation (7-day click thresholds ≥100 dB), only 1 demonstrated late vestibulopathy. Of the 4 animals that had late vestibulopathy, 2 animals also displayed severe hearing loss with 7-day postoperative click thresholds ≥85 dB in the ear with PLF.
DISCUSSION
IEBT and IEDCS have remarkably similar symptoms and may be difficult to distinguish clinically. 1–7 Some authors believe PLF to be a contraindication to recompression and reserve compression therapy for cases with the strongest suspicion for IEDCS, in an attempt to prevent repeat barotrauma. 1,3,11 To our knowledge, there have been no published, prospective, controlled, experimental studies to validate this treatment dogma. Our observations suggest that there is no significant compromise of cochlear or vestibular function in ears with PLF subjected to compression versus no compression. These results concur with those reported in an abstract presented by Stevens and colleagues. 8 In the latter study, animals were exposed to a single dive to 6 atmospheres, but the dive profile was not reported. In a previous study, 12 we found that rapid compression of guinea pigs 3 weeks after stapedectomy was not complicated by significant hearing loss. Rapid compression after recent stapedectomy may be considered analogous to oval window PLF.
Both auditory and vestibular dysfunction was found more often and to a greater degree in the ears with PLF. The impact of experimental PLF on inner ear dysfunction is well established. 13-15 In other words, hearing loss and dizziness encountered with IEBT are more likely a result of the initial injury, rather than the use of compression therapy.
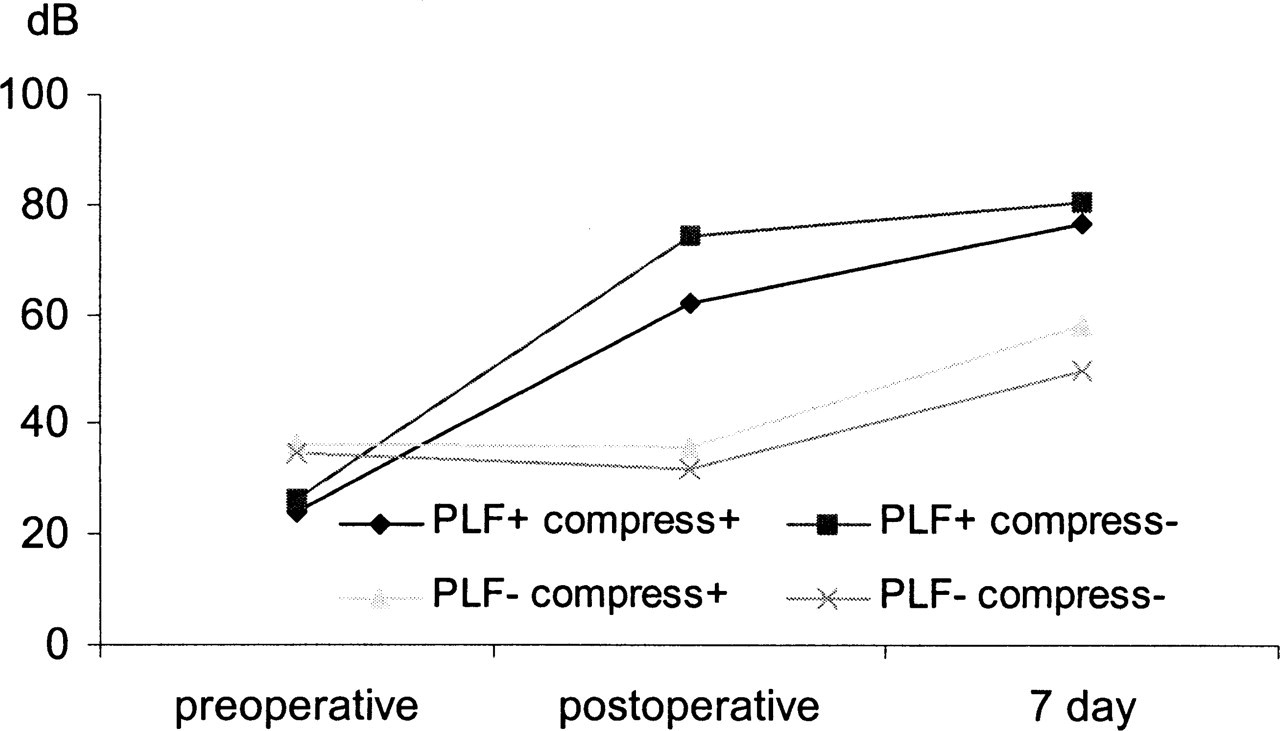
Shown are click-evoked electrocochleographic thresholds over time, with or without (+ or −) compression (compress) in animals with or without (+ or −) PLF.
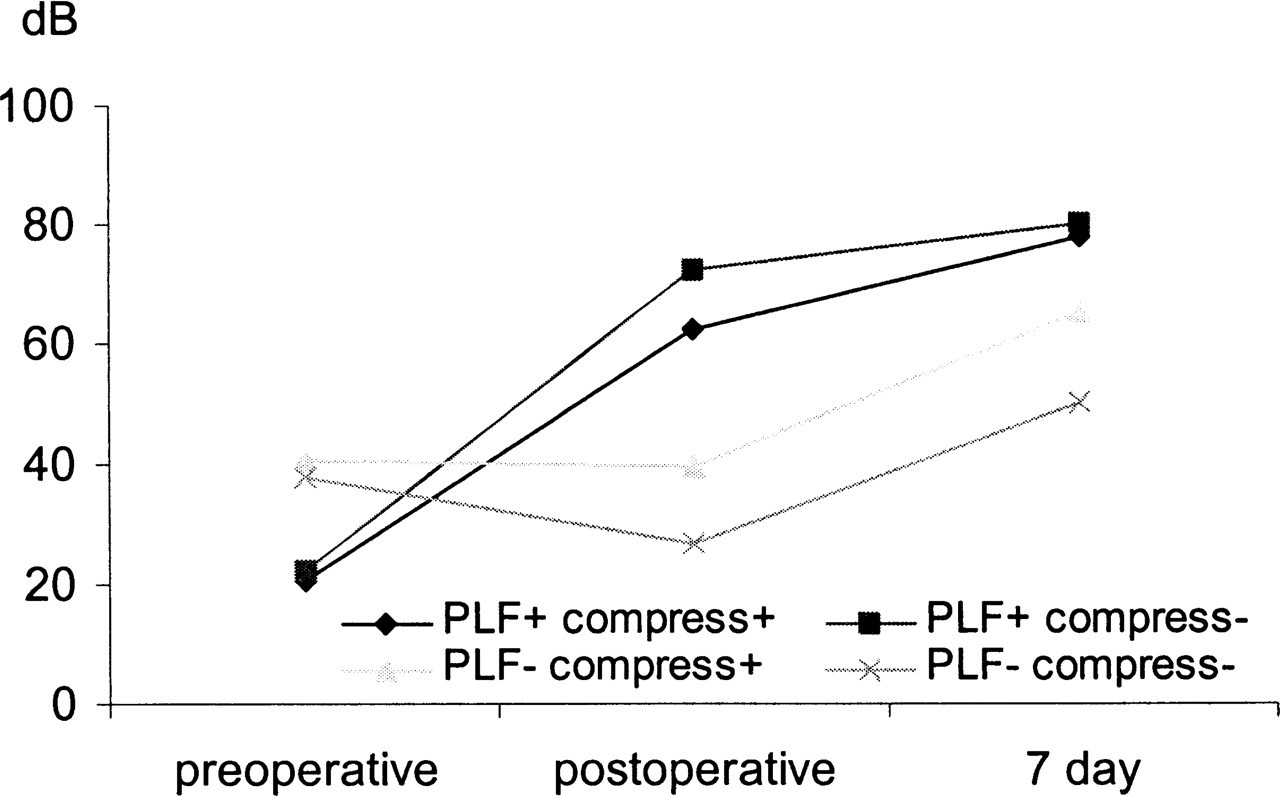
Shown are 4-kHz tone pip-evoked electrocochleographic thresholds over time, with or without (+ or −) compression (compress) in animals with or without (+ or −) PLF.
Middle ear pathology, ranging from effusion to perforation, was observed in many ears, independent of PLF or compression status. These observations suggest that the middle ear pathology was the (expected) result of eustachian tube obstruction and middle ear manipulation that was performed on all ears. As middle ear status did not correlate with either treatment group or auditory dysfunction, it is unlikely that the hearing results were biased by middle ear status.
As with any experimental study, extrapolation to the human condition must be done cautiously. PLF encountered in scuba diving accidents may be accompanied by more severe inner ear pathology. 7,16 Unfortunately, no animal models are known to more closely replicate human IEBT.
It is also possible that our attempt to predispose to IEBT with compression in the animal model—by anesthetizing the animal and reducing its spontaneous jaw movements—may have actually reduced the risk for IEBT. It has been suggested that IEBT may result from forceful equilibration of middle ear pressure by autoinflation. 1
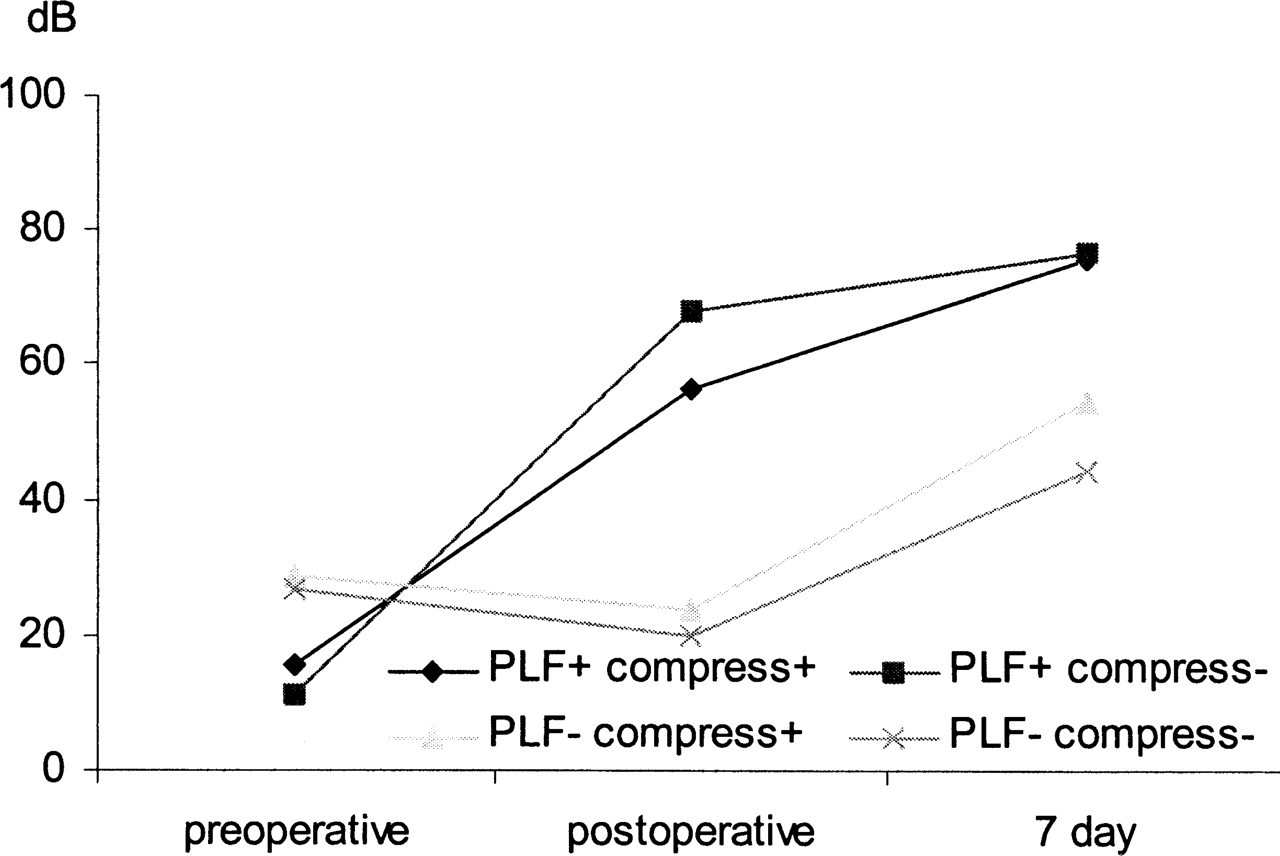
Shown are 8-kHz tone pip-evoked electrocochleographic thresholds over time, with or without (+ or −) compression (compress) in animals with or without (+ or −) PLF.

Shown are 16-kHz tone pip-evoked electrocochleographic thresholds over time, with or without (+ or −) compression (compress) in animals with or without (+ or −) PLF.
Evidence of vestibulopathy in animals with and without compression

CONCLUSION
Observations in the guinea pig suggest that the cochlear and vestibular sequelae of PLF are unlikely to be aggravated by hyperbaric compression. Such observations should be cautiously extrapolated to the humans. The rarity of diving-related PLF does not allow for large-scale controlled studies to corroborate these findings in humans. However, in situations where it is difficult to distinguish IEBT, with possible PLF, from IEDCS or where both may coexist, it may not be as risky as has been previously thought to treat the patient with recompression therapy.