
Abstract

Diagnosis of perilymphatic fistula after penetrating trauma to the middle ear is usually not difficult. Vertigo, nystagmus, combined or pure sensorineural hearing loss, and tinnitus, all signs of cochleo-vestibular damage, are usually present immediately after injury. With the development of microsurgery techniques, treatment has changed radically so that the treatment in cases of suspected perilymphatic fistula has evolved from a purely conservative therapy to exploratory tympanotomy and reconstruction. To decide when and how the surgery is to be performed, the type and extent of damage to the middle and inner ear must be determined, especially if the stapes is luxated into the vestibule. Moreover, when the stapes is luxated into the vestibule, it is important to determine how deeply and whether it is fractured. When such a case is encountered, thin-sliced, high-resolution computed tomography (HRCT) of the temporal bone can facilitate an accurate diagnosis of both the location and presence of fracture of the stapes.
CASE REPORT
A 13-year-old girl fell on the floor while scratching her right ear canal with an ear pick and the pick penetrated deeply into the ear canal. Immediately after this episode, she experienced otalgia, vertigo, tinnitus, and hearing loss in the right ear. On admission to our hospital, she had horizonto-rotatory gaze nystagmus, beating to the right. Otoscopic examination detected a perforation in the posterior half of the tympanic membrane. The malleus handle was intact, but the incudo-stapedial joint was not visible through the perforation. A needle otoscopic examination made through the perforation revealed that the long process of the incus was dislocated anteriorly, the incudo-stapedial joint was separated, and the stapes capitulum was leaning against the inferior edge of the oval window. The inferior aspects of the stapes were not visible. A pure-tone audiometric examination detected a mild hearing loss (pure tone average, 30 dB HL) with an increase in the bone conduction threshold on the right and normal hearing on the left. HRCT, in which joined 1-mm thick sections in the axial and coronal planes were obtained, showed that the incudo-mallear joint was slightly separated and the incus long process was dislocated anteriorly. The stapes was depressed deeply into the vestibule but was unfractured. Pneumolabyrinth, a sign of perilymph fistula, was evident (Figs 1 and 2).
After a full explanation of the procedure and its possible complications, surgical exploration of the middle ear was performed. After elevating the eardrum, the incus long process was found to be dislocated anteriorly. The stapes was depressed deeply into the vestibule, the capitulum was leaning against the inferior edge of the oval window. By inserting a hook into the obturator foramen, the stapes was gently removed from the vestibule. Perichondrium from the tragus was used to seal the oval window. Tragus perichondrium was also used to close the tympanic membrane perforation. The tragus cartilage was trimmed and placed as a columella between the oval window and the tympanic membrane.
Postoperatively, the patient's vestibular symptoms lessened markedly; spontaneous nystagmus disappeared 7 days after surgery. Caloric testing of the right ear did not elicit nystagmus 2 weeks after surgery, but only slight canal paresis was found 6 months later. Pure-tone audiometric examinations 2 weeks after surgery revealed moderate combined hearing loss (pure tone average, 45 dB HL) in the right ear. Her hearing had not changed during the 6 months postoperative follow-up period.
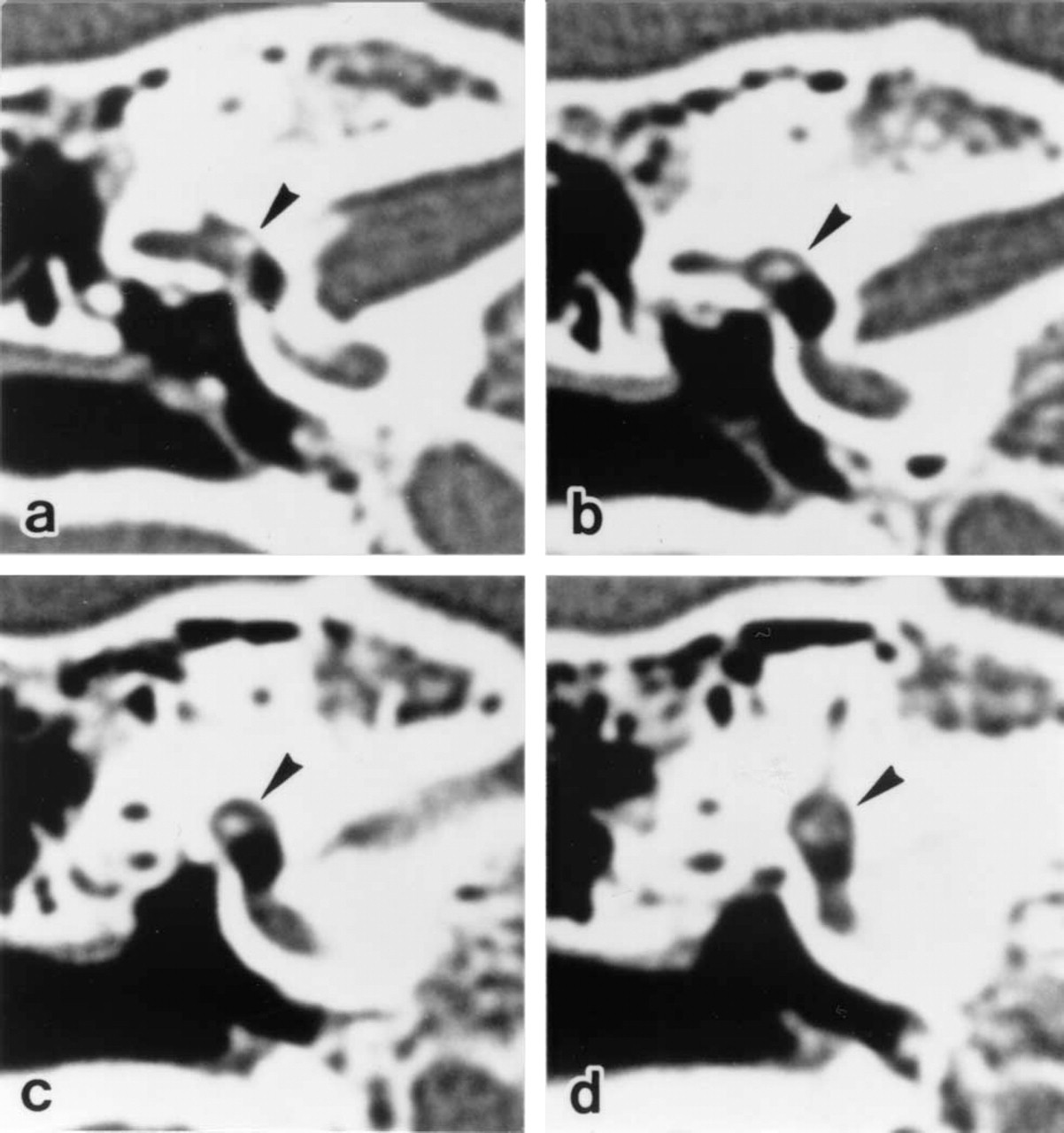
Coronal planes of thin-sliced, high-resolution computed tomography images show luxation of the unfractured stapes (arrowheads, a-d) deeply into the vestibule. Planes are moved posteriorly from a to d.
DISCUSSION
Traumatic luxation of the stapes into the vestibule is a rare complication in penetrating middle ear injury. Fracture of the stapes is not uncommon, but it is rarely accompanied by disruption of the annular ligament and depression of the footplate in the vestibule. 1 Very seldom is an intact stapes luxated out of the oval window or depressed into it. 1-5
Although rare, the possibility of stapes luxation into the vestibule must be kept in mind when perilymphatic fistula is suspected after penetrating middle ear injury because the treatment needed may differ in patients with stapes luxation into the vestibule. When the stapes is not depressed into the vestibule (ie, luxation out of the vestibule or rupture of the annular ligament without stapes dislocation), sealing of the perilymphatic fistula followed by ossicular chain reconstruction usually can be done without additional damage to the inner ear. However, when the stapes is depressed into the vestibule, several factors must be considered, eg, whether surgery should be performed at all, and if so, whether the stapes should be removed. This point is important because manipulation of the stapes may cause additional damage to the inner ear. Moreover, leaving the stapes in the vestibule may lead to late inner ear dysfunction because of vestibular space obstruction.
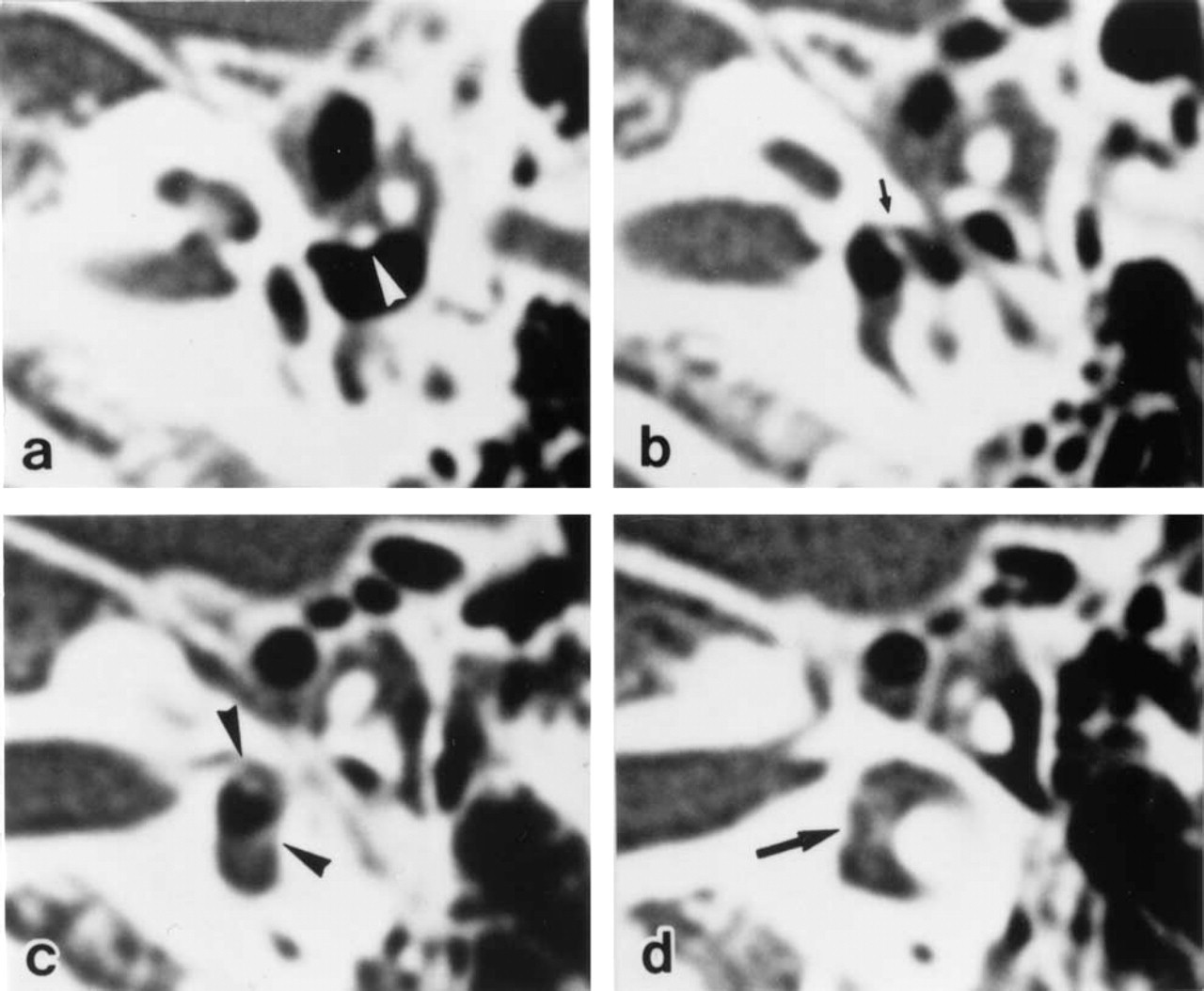
Axial planes of thin-sliced, high-resolution computed tomography images show anterior dislocation of the incus long process (white arrowhead) and luxation of the unfractured stapes deeply into the vestibule. Planes are moved superiorly from a to d. The small arrow (b) indicates the stapes capitulum; arrowheads (c), the anterior and posterior crus of the stapes; long arrow (d), the stapes footplate.
In deciding how surgery is to be performed when the stapes is depressed into the vestibule, it is important to determine the condition of the stapes (ie, how deeply is it depressed and whether it is fractured), as well as the extent of middle and inner ear damage. When the stapes is only slightly depressed into the vestibule, exploratory tympanotomy followed by reconstruction with or without removal of the stapes can provide a fairly good prognosis for recovery of hearing. 1,5 When the stapes is deeply depressed into the vestibule, however, the risk of causing additional inner ear damage on surgical intervention is increased. Ogawa et al 5 reported development of severe deafness in 3 of 4 patients whose stapes, deeply depressed into the vestibule, had been removed. Vanderstock et al 3 reported hearing recovery after reconstruction following removal of a deeply depressed stapes, but the bone conduction thresholds deteriorated slightly. Taking into account these reports, removal of a deeply depressed stapes from the vestibule may not always be a good choice. When, however, the stapes is left in the vestibule, scarring around it may occupy the vestibular spaces and cause late inner ear damage. For instance, Herman et al 4 reported on a 47-year-old woman with complete stapes luxation into the vestibule after a penetrating middle ear injury who had not undergone surgical treatment initially. She was completely deaf and had disabling vertigo 3 years later. We therefore consider it better to remove the deeply depressed stapes despite the potential risk of additional inner ear damage. After removing the stapes, it is necessary to seal the oval window with tissue and reconstruct the ossicular chain.
Another important factor to consider in the case of stapes luxation into the vestibule is whether the stapes is fractured. If the fractured stapes is slightly depressed into the vestibule, it is not difficult to remove all stapes fragments, whereas it is very difficult to remove all the fragments without causing severe inner ear damage when the fragments are deeply dislocated into the vestibule.
As stated above, the prognosis of inner ear function and, therefore, the treatment required are markedly influenced by the condition of the stapes when it is dislocated into the vestibule. Needle otoscopic observation may be useful for determining the extent of depression of the stapes, 2 but it does not provide information about whether the stapes is fractured. Our study shows that HRCT can facilitate making an accurate diagnosis, not only of the location but of whether the stapes is fractured. When the stapes is luxated into the vestibule, surgeons need to obtain sufficient information about the stapes condition in order to give a full explanation to the patients about the suggested surgical procedure and its possible outcome. We therefore strongly recommend performing an HRCT when patients are suspected of having luxation of the stapes into the vestibule.