
Abstract
OBJECTIVES: We sought to determine the thromboprophylactic effects of low-molecular-weight heparin (LMWH) and pentoxifylline.
DESIGN: Randomized blinded study.
MATERIALS AND METHODS: Sixty Sprague-Dawley rats were assigned to 1 of 4 treatment groups: (1) control group (n = 15), (2) pentoxifylline group (n = 15), (3) LMWH group (n = 15), and (4) combined therapy group (n = 15). A groin/abdominal free flap was elevated in each, with division of the artery and microvascular repair The animals received therapy for 4 days preoperatively and 6 days postoperatively. Flaps were monitored visually, and on the seventh postoperative day, the flap was elevated, and the microvascular anastomosis was assessed for patency.
RESULTS: There was a statistically significant improvement in arterial patency in both pentoxifylline and LMWH groups compared with controls (P < 0.01) but no significant improvement with combined therapy (P > 0.05).
CONCLUSIONS: In this animal model, LMWH and pentoxifylline have significant thrombroprophylactic effects when used individually but not in combination.
Several studies have addressed the benefit of perioperative antithrombotic agents in optimizing blood flow through microvascular pedicles. Of the numerous pharmacological agents used, one that has met with universal acceptance is topical heparin due to its proven efficacy in preventing thrombosis and improving microvascular patency in rat models. 4,5 However, the optimal systemic agent, dosing schedule, and duration of treatment have yet to be established. The 2 agents selected for our study were low-molecular-weight heparin (LMWH) and pentoxifylline. These drugs have been previously evaluated and used within the fields of microvascular surgery and orthopedic surgery for their effects in reducing thrombosis and maintaining vascular patency. 6-11
LMWH was attractive to us for study because it is a relatively new alternative to heparin that is thought to prevent intravascular thrombosis without the same degree of prolongation of the activated partial thromboplastin time and risk of bleeding. LMWHs have a different mechanism of action to standard heparin, acting primarily by inhibiting factor Xa. They have a longer half-life and much higher bioavailability. It has been shown that topical administration of LMWH prevents the occurrence of thrombosis at the traumatic anastomotic site in animal models to a similar degree as heparin. 6,7 In a randomized, double-blinded clinical study on 136 patients who underwent elective total hip replacement where the drugs were given by subcutaneous injection, the efficacy of LMWH was superior to that of standard heparin in the prevention of femoral thrombosis and pulmonary embolism. 8 In the same study, the total loss of blood and the total amount of blood that was transfused were significantly reduced in the patients who received LMWH compared with those who received standard heparin.
Pentoxyphylline was also an attractive pharmacologic agent for study in this setting because its mechanism of action was completely different than that of other antithrombotic agents. In searching for the best combination of antithrombotic agents therefore, it seemed a logical choice. Pentoxifylline, a xanthine derivative, increases erythrocyte flexibility and enhances the prostaglandin2 release from the vascular wall and causes increasing platelet sensitivity to antiaggregating prostaglandins. 9 In a double-blinded study using Sprague-Dawley rats, pentoxifylline given intraperitoneally resulted in a statistically significant improvement in microvascular patency when compared with controls. 10 The drug reduced the number of intramural vascular channels and prevented formation of endovascular thrombus following microanastomosis in the rat inferior vena cava. 11
The purpose of this study was, therefore, to study the individual antithrombotic effects of LMWH and pentoxifylline, to determine whether a combination of these drugs resulted in increased efficacy, and to assess the correlation of anastomotic patency with survival of the flap in control and test animals.
MATERIALS AND METHODS
Subjects
Sixty Sprague-Dawley rats, weighing 300 to 400 g, were included in the study. The animals were randomized by a technician to 1 of 4 treatment groups: (1) control (no treatment) group, (2) LMWH group, (3) pentoxifylline group, and (4) combined therapy (LMWH + pentoxifylline) group. Fifteen animals were placed in each group. Four additional flaps were raised and the artery was ligated, without anastomosis to confirm flap necrosis. The principal investigators and pathologist were blinded as to group assignment or the selected therapeutic regimen. LMWH was given in a dosage of 1.5 mg/kg/day via subcutaneous injection and pentoxifylline 24 mg/kg/day via gastric gavage tube. Both regimens were given for 4 days preoperatively and 6 days postoperatively. The study had been approved by the University of Miami Animal Care and Use Committee, and its guidelines were followed throughout the study.
Operative Procedure
The animals were anesthetized with intraperitoneal sodium pentobarbital (Nembutal; 50 mg/kg body weight) and positioned supine. A groin/abdominal free flap, based on the inferior epigastric artery and vein, was used in the study. The flap, measuring approximately 5 cm × 3 cm, was marked out, and an incision was made down to the external oblique muscle medially and thigh muscle laterally. The skin paddle was elevated and left based solely on its pedicle. The femoral vessels were dissected from the inguinal ligament to approximately 5 mm distal to the branching of the inferior epigastric vessels. All minor branches were cauterized with bipolar diathermy or ligated and divided. The artery proximal to the branching was dissected free from the adjacent vein, placed within the double microvascular arterial clamp, and divided. A standard end-to-end anastomosis was carried out using interrupted 10–0 nylon (Ethicon, Inc) sutures. The anastomosis was checked for patency by flow studies, including the empty and refill test, immediately afterwards. A controlled injury of the vessel wall was then created by applying a hemostat for 10 seconds at 5 mm proximal to the anastomosis, clamping one fourth of the vessel diameter. The femoral vessels distal to the branching of the inferior epigastric artery were ligated to ensure that the flap was perfused exclusively by the proximal femoral artery via the inferior epigastric artery. The skin flap was laid back in place, 4–0 nylon sutures were applied, and the animal was allowed to emerge from anesthesia.
Anastomotic patency and skin flap status in the 4 treatment groups
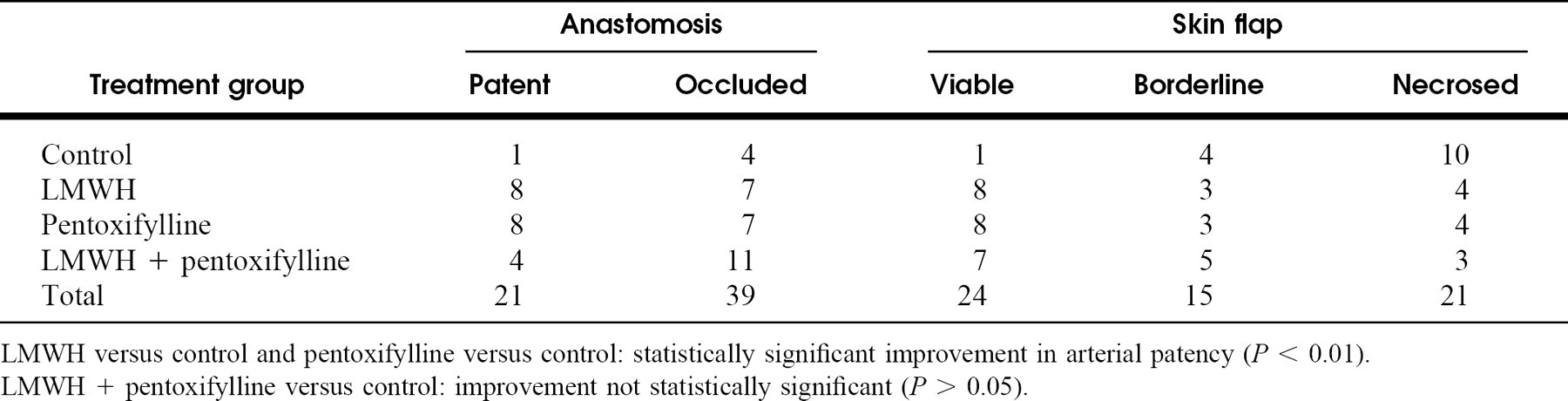
LMWH versus control and pentoxifylline versus control: statistically significant improvement in arterial patency (P < 0.01).
LMWH + pentoxifylline versus control: improvement not statistically significant (P > 0.05).
On the seventh postoperative day, the animal was reanesthetized and the gross appearance of the skin flap was recorded. It was noted to be viable if it retained its pink colour, soft consistency, and capillary refill; necrosed if it appeared black, crusted, and dessicated; or borderline if the features fit between the 2 categories. The flap was elevated, and the anastomosis was examined for patency by flow studies. Selected skin paddles and vascular pedicles including the area of anastomosis were harvested en bloc and submitted for histopathologic evaluation. The animal was then killed with a lethal dose of sodium pentobarbital intraperitoneally.
Pathology
The specimen was immersed in formaldehyde, and each jar was labeled with the previously assigned code. Sections of the vascular anastomosis were prepared for light microscopy using hematoxylin and eosin stains.
Statistical Analysis
Recording and analysis of data for the 4 treatment groups were carried out. Surgical findings were correlated with histopathologic examination, and the relationship of skin flap viability with anastomotic patency was noted. Statistical significance was evaluated in accordance with Fisher-Yates test.
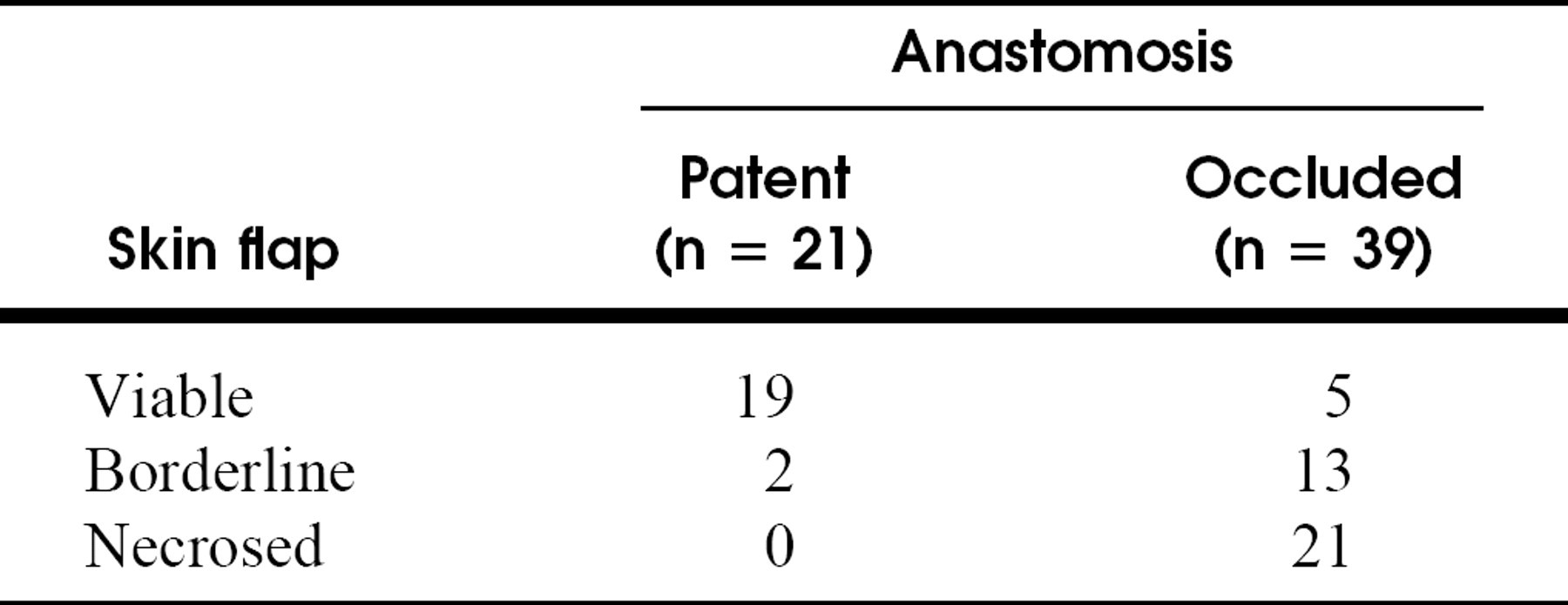
Correlation of skin flap viability and anastomotic patency
RESULTS
The distribution of anastomotic patency and skin flap status within the 4 treatment groups is shown in Table 1. The numbers of subjects with patent/occluded anastomoses and viable/borderline/necrosed skin flaps were identical in the pentoxifylline and LMWH groups. On comparison of the pentoxifylline and LMWH groups individually with the control group, there was a statistically significant improvement in arterial patency with both drug groups (P < 0.01). However, the combined group did not show a statistically significant improvement over the control group (P > 0.05).
The correlation of skin flap viability and anastomotic patency is shown in Table 2. As shown in the 2 tables, the vast majority of patent anastomoses (90%) were associated with a healthy skin flap and the majority of occluded anastomoses (54%) with a necrosed skin flap. However, of the 39 occluded anastomoses, 33% were associated with borderline viability flap and 13% with a completely healthy flap. Four additional rats done without arterial anastomosis experienced, as expected, complete flap necrosis.
Histopathologic assessment was carried out in 9 randomly selected specimens. These comprised 4 patent and 5 occluded anastomotic segments as assessed by clinical criteria. These anastomotic segments as assessed by clinical criteria. There was histopathologic correlation with the clinical findings in 8 cases (88%). The 1 remaining specimen, assessed to be a patent anastomosis clinically, was found to be partially occluded by a thrombus on histopathologic evaluation. Figures 1 and 2 demonstrate the histopathologic appearances of a patent and occluded anastomosis respectively.
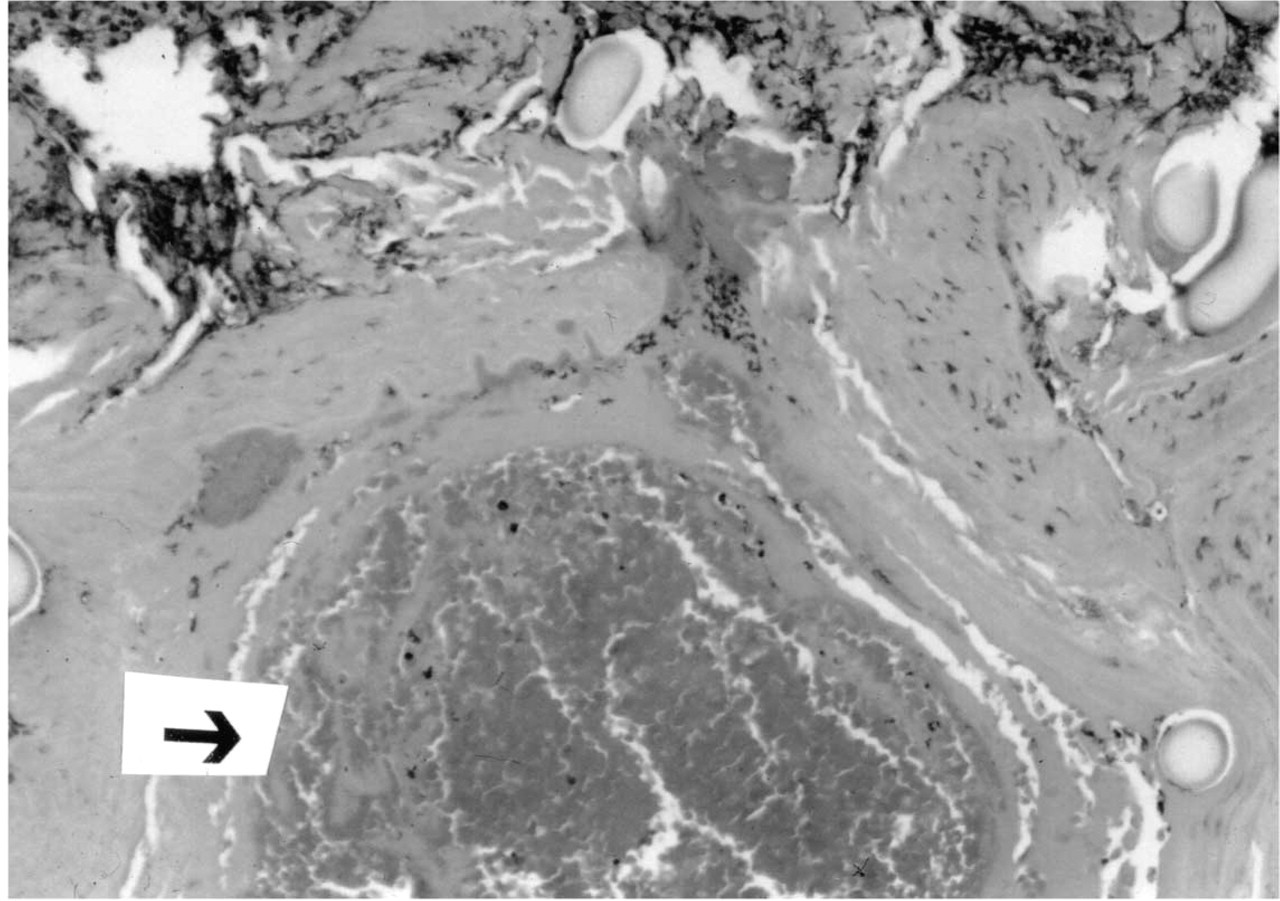
Photomicrograph of section of patent anastomosis (H&&E; original magnification, ×100).
DISCUSSION
The use of medications to reduce thrombosis has been advocated due to the risk of thrombosis in microvascular surgery. Despite numerous animal studies and clinical reports, there remains a lack of standardization of the optimal agent, regimen, and dosing schedule in clinical practice. Although standard heparin has been widely acclaimed as the drug of choice in preventing microvascular thrombosis, heparin-induced platelet activation, limits its effects in preventing arterial thrombosis, 12 and prolongation of APTT results in increased risk of bleeding. 4
The above study, carried out in blinded fashion to eliminate observer bias, is the first of its kind to compare the effects of 2 thromboprophylactic pharmacologic agents, used singularly and in combination, in the maintenance of patency of vascular microanastomoses after crush injury and survival of microvascular free flaps. Although the 2 drugs, LMWH and pentoxifylline, have been used widely in clinical practice and in animal experiments via topical application on microvascular anastomoses, there are very few reports of the effects of these drugs given enterally or parenterally. Similarly, there are fewer studies on the effects on free flaps supplied by the microvascular anastomoses as most assessments are centered around the patency of the anastomoses themselves. The simple rat groin flap model was chosen because it closely approximates the human composite flaps used in free flap reconstruction. To study the thromboprophylactic and antithrombotic potential of the 2 drugs, predisposition to thrombosis at the anastomotic site was enhanced by a controlled injury to the vessel wall just proximal to the anastomosis. Both LMWH and pentoxifylline, when used singularly, were found to have a significant effect in the prevention of thrombosis and maintenance of patency across the microvascular anastomosis. However, the combination of the 2 drugs was surprisingly less effective in achieving this state of events. Because the mechanisms of action of the 2 drugs are quite different, there is no obvious explanation based on the pharmacologic properties of the agents. It is possible that an undetermined antagonistic reaction may be responsible for this phenomenon. Alternatively, whereas some degree of anticoagulant and/or antiplatelet activity may be beneficial, the combination of an anticoagulant with an agent that interferes with platelet function may be detrimental by simply reducing coagulatory function excessively, thereby preventing sealing of the vascular anastomosis, leading to surrounding hematoma. Interestingly, one could easily envision a clinical situation where a patient might be place on both drugs. At the very least this finding reminds us that unexpected results can be obtained when various medications are used in combination and that nothing can be assumed regarding unproven but theoretically beneficial pharmacologic combinations.
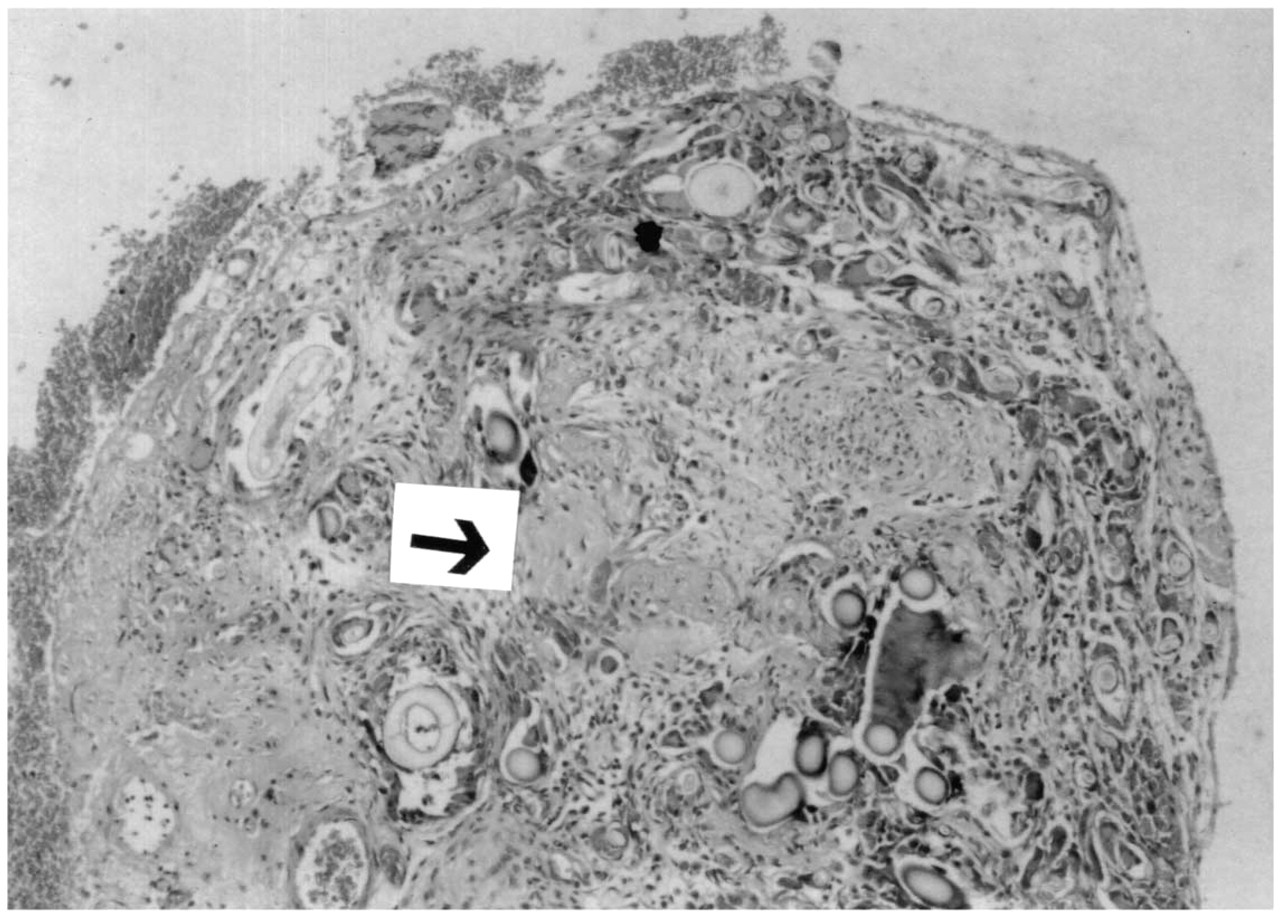
Photomicrograph of section of anastomosis occluded with thrombus (H&&E; original magnification, ×100).
It is widely assumed that the health of the free flap is strictly dependent on the status of the microvascular anastomosis, at least during the initial few weeks. It was, however, demonstrated that where, as expected, the vast majority (90%) of patent anastomoses were associated with a healthy skin flap, just over half of the occluded anastomoses were associated with a completely nonviable flap. One third of the occluded anastomoses were compatible with a flap that still survived, and 13% with a completely healthy flap. It is possible that in this situation, the flap may take as a free graft, particularly in the borderline cases, or there could be a delayed failure of the anastomosis, thereby still allowing the skin flap to survive after it had achieved its own circulation. Although vascular patency did not necessarily correlate with flap viability, the flap portion was important to understand the animal model. All pedicles were assessed by the empty and refill test to confirm patency, and this was the true indication that reflected whether thrombosis occurred in the immediate postoperative period. The maintenance of a patent venous circulation may have assisted the survival of flaps after thrombosis of the arterial circulation. In any case, although advantageous because of its simplicity, necrosis in 4 cases where no arterial anastomosis was performed supports the latter theory. This animal model must be considered imperfect as a model for a free flap transfer. Nonetheless, it is probably still preferable to seek an animal model for microvascular anastomosis in the environment of an elevated flap. Despite the occasional tissue survival after anastomotic failure, our model still represents an inexpensive means of simulating the clinical situation of a free tissue transfer.
A study of the antithrombotic properties of LMWH carried out on microvascular anastomoses after arteriotomies of the central arteries of rabbit ears showed a patency rate of 73% with parenteral administration of the drug. 13 In the same study, the mean weight of the thrombotic material in each artery was also significantly lower in the LMWH group than in the control group. The beneficial antithrombotic effects of LMWH were also demonstrated in a recent study carried out on a group of Sprague-Dawley rats. 14 After administration of the drug to the animals after microvascular anastomosis of the femoral artery and vein, a patency rate of 15/15 (100%) was noted with the drug compared with controls (10/15, 66.6%). However, a controlled injury to promote thrombosis was not performed in this study. Another study on Sprague-Dawley rats involving a controlled crush injury to the femoral vessels followed by anastomosis showed a significantly higher patency rate (P < 0.001) after the use of both topical LMWH at higher concentrations (12/ 20, 60%) and a combination of topical and systemic administration of the drug (10/16, 62.5%) at day 7. 15 These results correlate well with the findings in our own study.
A study of the effects of pentoxifylline administration on microvascular anastomotic patency rates of femoral arteries and veins in streptozotocin-induced diabetic rats showed that the drug improved microvenous patency at all levels of hyperglycemia studied. 16 This was statistically significant in uncontrolled diabetic animals, where the patency was increased from 0% to 36% (P = 0.05). A study to investigate the effects of pentoxifylline on the healing of intestinal anastomoses in rats with experimentally induced obstructive jaundice demonstrated that the administration of the drug resulted in better anastomotic wound healing. 17 This was attributed to its inhibitor effect on the endotoxin-induced tumor necrosis factor-α release from macrophages and monocytes and the stabilizing effect on neutrophils.
The value of antithrombotic therapy for free tissue transfer has been well established in the literature. An international survey of microvascular practices in free flap transfer showed that some form of prophylactic antithrombotic treatment was routinely given in 91% (75/83) of the centers. 18 The incidence of thrombosis in the category not using antithrombotic drugs was more than that in the category using such therapy (15.2% versus 7.1%). These results, however, need to be interpreted with caution due to the large discrepancy in the number of cases between the 2 groups (184 versus 3527). Following reoperations, the overall success was almost identical in the 2 groups (95.1% vs 95.7%). The routine use of antithrombotic agents therefore may decrease the frequency of thrombosis and thus the need for reoperation.
Based on the above study, both LMWH and pentoxifylline have significant thromboprophylactic activity when utilized singularly in the perioperative period following microvascular anastomosis. For the case where anastomotic patency was not maintained despite drug administration, it is possible that the degree of thrombogenesis stimulated by the injury may have outweighed the antithrombotic potential of these drugs. Although the number of subjects is too small to draw effective conclusions, the results suggest that there is a trend for the combination of the 2 drugs to have a deleterious effect in maintaining anastomotic patency. However, one must be cautious in extrapolating these findings to the clinical situation. Differences in the vessel wall, blood, and circulation between humans and rats are considerable. Both agents studied, however, have been found suitable for use in patients. Preoperative administration of LMWH was found to be safe in head and neck cancer surgery, 19 although further studies are required to evaluate its efficacy in preventing thromboembolism.
The cost of these medications represents an additional issue. It is difficult to perform a clinical cost-benefit analysis in a situation where there is no standard regimen, and the true clinical benefits of treatment have not been quantified in a randomized trial. However, some form of antithrombotic therapy is in widespread clinical use, and there is a financial cost involved in these medications. The cost for the medications studied here is quite disparate. The average wholesale price for a 3-day course of pentoxifylline is approximately $7, whereas that for LMWH is about $300. By comparison, a 325 mg aspirin suppository for 3 days costs less than $1, and Dextran 40 intravenous infusion at 25 mL/h for 3 days costs $600. 20 The goal of animal studies such as this is to provide information that would ultimately allow for the planning of a clinical trial to compare treatment regimens. Such a study would allow for an accurate cost-benefit analysis of pharmacologic intervention in the prevention of vascular thrombosis after free tissue transfer.
CONCLUSION
The present study indicates that the use of perioperative antithrombotic agents given systemically is beneficial in maintaining arterial patency following microvascular anastomosis and stimulation of thrombogenesis in rats. Both LMWH and pentoxifylline showed identical significant antithrombotic effects when used in isolation and compared with controls. However, when using the combination of the 2 drugs, these effects were significantly reduced. Our flap model was limited by some degree of flap survival after vascular thrombosis, presumably related to temporary patency followed by delayed thrombosis.