
Abstract
OBJECTIVE: We sought to determine the effect of montelukast, a leukotriene receptor antagonist, on intradermal skin testing.
STUDY DESIGN AND SETTING: We conducted a prospective, randomized, double-blind, placebo-controlled study in a university setting.
METHODS: After a 1 -week washout of allergy pharmacotherapy, intradermal skin testing was performed on 23 atopic subjects. Whealing size was measured 20 minutes after injection. Subjects then began a 1 -week regimen of daily loratadine, montelukast, or placebo. At 1 week, subjects again underwent intradermal skin testing. The change in wheal size was then calculated from baseline.
RESULTS: A significant difference (P < 0.05) between the montelukast and loratadine groups in suppression of intradermal whealing at 1 week was observed. No significant difference was noted between the montelukast and placebo subjects.
CONCLUSIONS: Montelukast demonstrated no significant suppression of skin whealing after antigen challenge over placebo.
SIGNIFICANCE: Montelukast does not need to be discontinued before intradermal allergy testing.
Intradermal skin testing introduces an allergen into the dermis of the skin to provoke an immediate response. The presence and magnitude of the whealing response allow for the qualitative identification and quantification of an individual's allergic sensitivity. Many medications are known to have an effect on intradermal skin testing, including theophylline, β2-agonists, prochlorperazine, some sedatives, and antihistamines. 14–16 These agents must be stopped before skin testing to obtain reliable results.
Leukotriene receptor antagonists are a new class of medications that have been shown to be useful in the treatment of allergic diseases including asthma and allergic rhinitis. 17–21 Few studies, however, have evaluated the effect of 5-OH-lipoxygenase inhibitors or leukotriene receptor antagonists on the type I hypersensitivity reaction. 20,22–25 Recently, Simons, Johnston, and Gu 22 described the early and late cutaneous responses of 12 atopic patients after intradermal challenge of allergen, histamine, LTD4, and saline control. Re-testing was then performed after a 1-week course of fexofenadine, montelukast, fexofenadine, and montelukast concurrently, or placebo. All treatments in this study were found to affect cutaneous allergic responses compared with pretreatment baseline. The suppressive effect noted in the placebo group makes conclusions of significance somewhat difficult in this report. 23
The current study is designed to examine the effect of various agents in suppressing skin whealing after intradermal allergy testing. The specific aim of this study was to determine the effect of montelukast, a leukotriene receptor antagonist, on skin response during intradermal skin testing.
METHODS
Subjects
Adults between the ages of 18 to 70 years with suspected inhalant allergy were invited to participate in this study. Subjects were solicited from the Wayne State University School of Medicine community. They were advised of the study and the requirements for their participation and, if they wished to proceed, underwent a full informed consent procedure. Individuals with uncontrolled asthma or known sensitivities to the study medications were excluded. The study design was approved by the Human Investigation Committee of Wayne State University and was conducted according to its guidelines.
Procedure
This investigation was a prospective, double-blind, randomized, placebo-controlled experimental study. A pretest, posttest design was used with 3 treatment groups. Subjects were tested for allergy using a standard screening skin prick test (Multi-Test II; Lincoln Diagnostics, Decatur, IL). Those subjects who demonstrated a wheal of 3 mm or greater in diameter to 1 or more of 7 common inhalant antigens (Timothy grass, short ragweed, oak, cat dander [Fel D1], dust mite [D. pteronyssinus], Alternaria, or Aspergillus) were qualified to participate in the intervention phase of the study. All subjects underwent baseline intradermal testing performed with 1 specific allergen to which they reacted on the skin prick testing. They were then randomized into 1 of 3 groups: loratadine, montelukast, or placebo.
Each subject then underwent a 1-week washout, during which time they were advised to discontinue any oral or intranasal allergy medications, as well as any other medications known to interfere with skin testing. At the time of baseline allergy testing, a single 4-mm wheal of 0.01 to 0.02 mL of 1:500 weight-to-volume solution of histamine was placed as a positive control for skin response. Subjects were identified as adequately reactive if the histamine challenge grew to a diameter of 7 mm at 10 minutes. All subjects then underwent baseline intradermal injections of 1:2500 weight-to-volume dilutions of both a demonstrated allergen and Candida albicans. Intradermal 4-mm wheals were raised with 0.01 to 0.02 mL with a standard 26-gauge allergy syringe. The whealing responses were then measured 20 minutes after injection in both vertical and horizontal axes. The mean wheal diameter was recorded. Subjects were also given a standardized measuring device (Antigen Laboratories, Inc, Liberty, MO) and instructed on the measurement of the C albicans injection site to be performed 24 hours later to evaluate for any delayed allergic responses.
The 3 treatment medications to be used were loratadine 10 mg, montelukast 10 mg, and a lactose placebo. Loratadine was included as a positive control for assessing suppression of wheal and flare and placebo was included as the negative control. The treatment medications were prepared by a registered pharmacist in the Wayne State University College of Pharmacy and were dispensed in a double-blinded fashion to each subject. All 3 medications were encapsulated to prevent visual discrimination among the 3 agents. This encapsulation process was judged not to have significant effect on the absorption or bioavailability of test medications. Each dose was dispensed in a labeled container holding a 1-week course. Subjects were instructed to take 1 capsule orally once daily at a similar time.
After subjects had completed the 1-week course of test medication, steady-state levels of the drug were obtained as predicted by the pharmacokinetics of the medications. The patients were reevaluated by intradermal skin testing with a positive histamine control, and similar procedures were followed for administration of C albicans and the same antigen used for baseline assessment. Whealing was then measured after 20 minutes. Again, the change in wheal size was calculated. A repeat evaluation was again performed 1 day later by the patient to assess for any delayed skin reactions.
Wheal diameters for loratadine
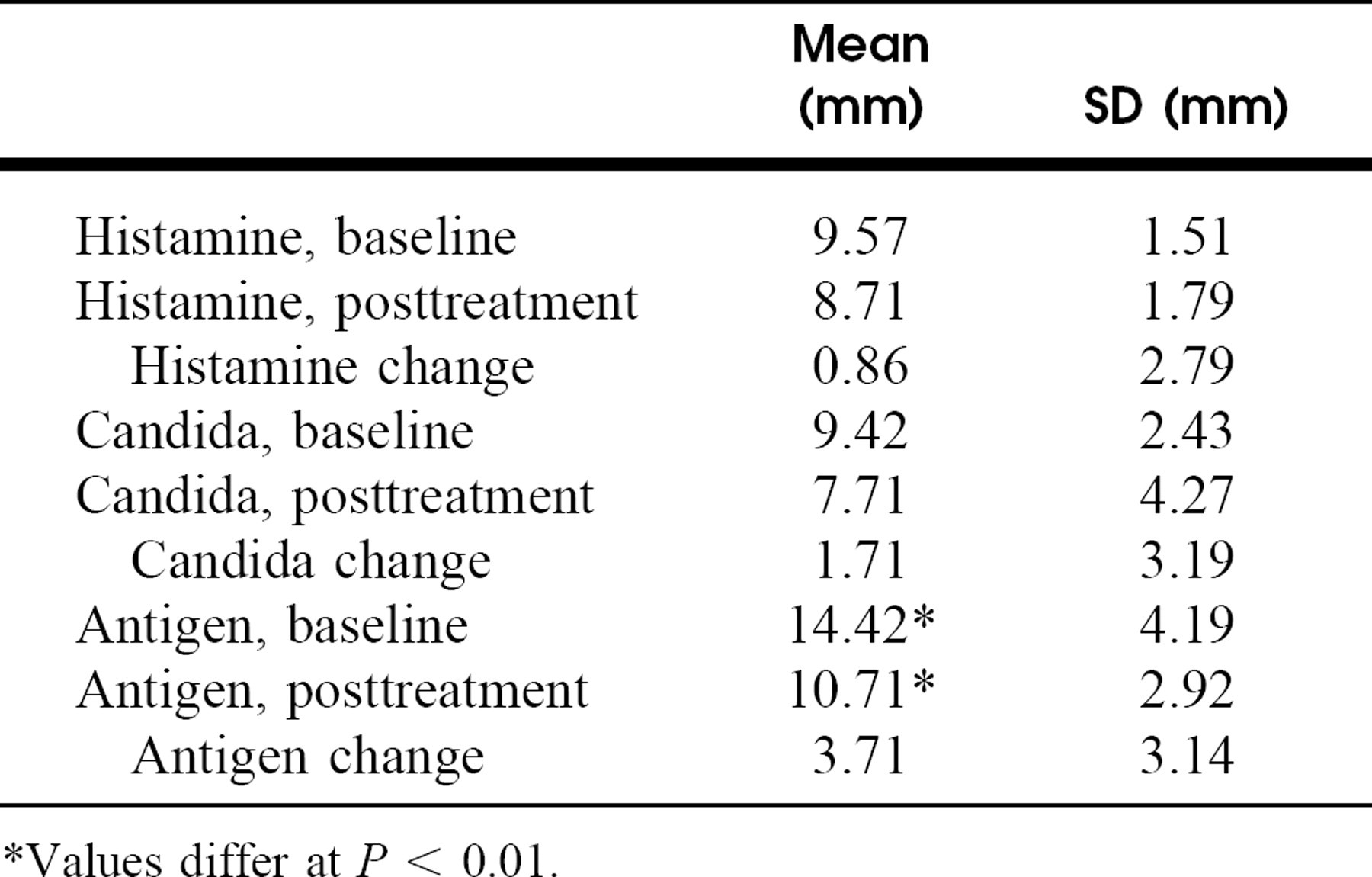
Values differ at P < 0.01.
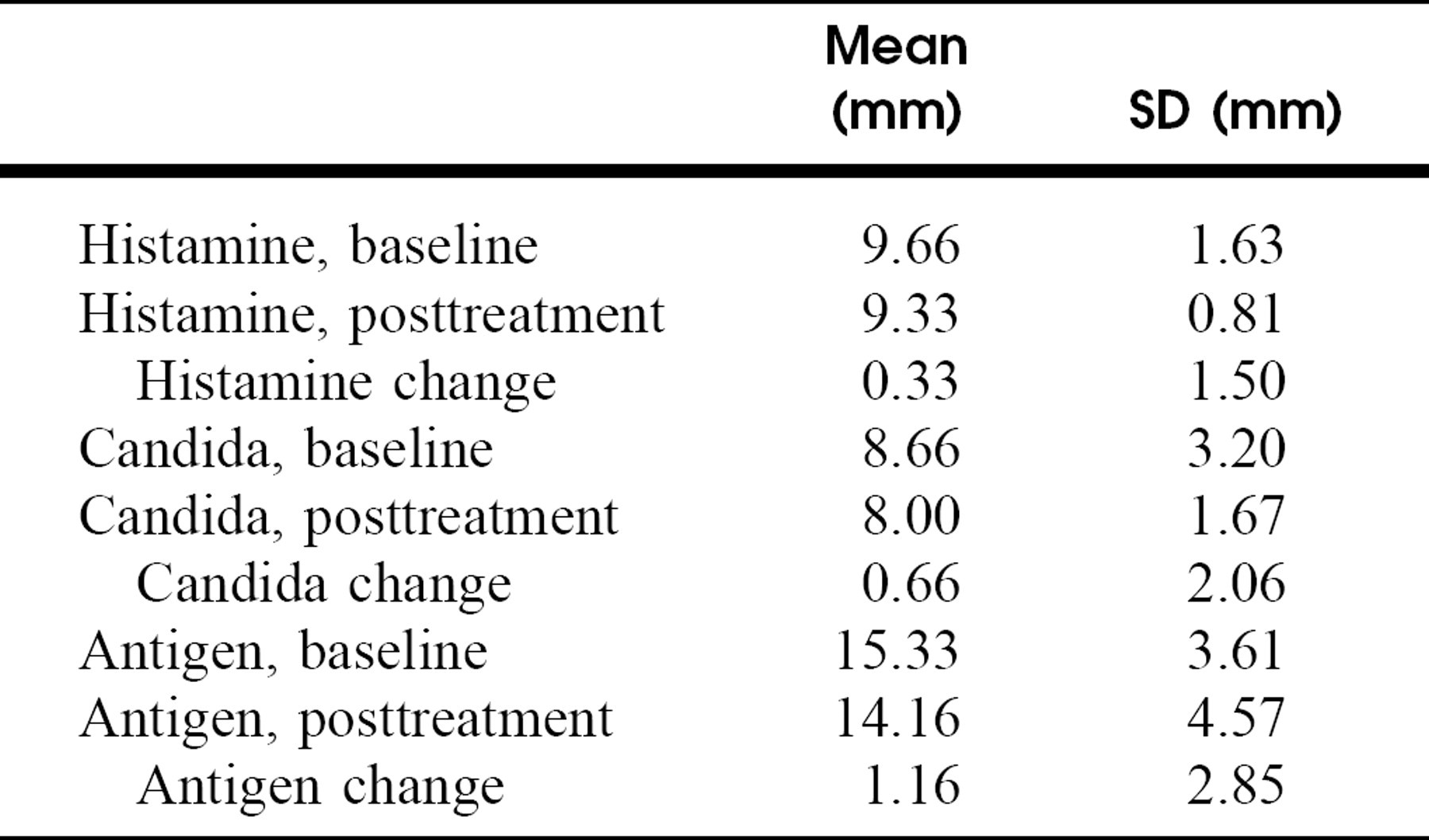
Wheal diameters for montelukast
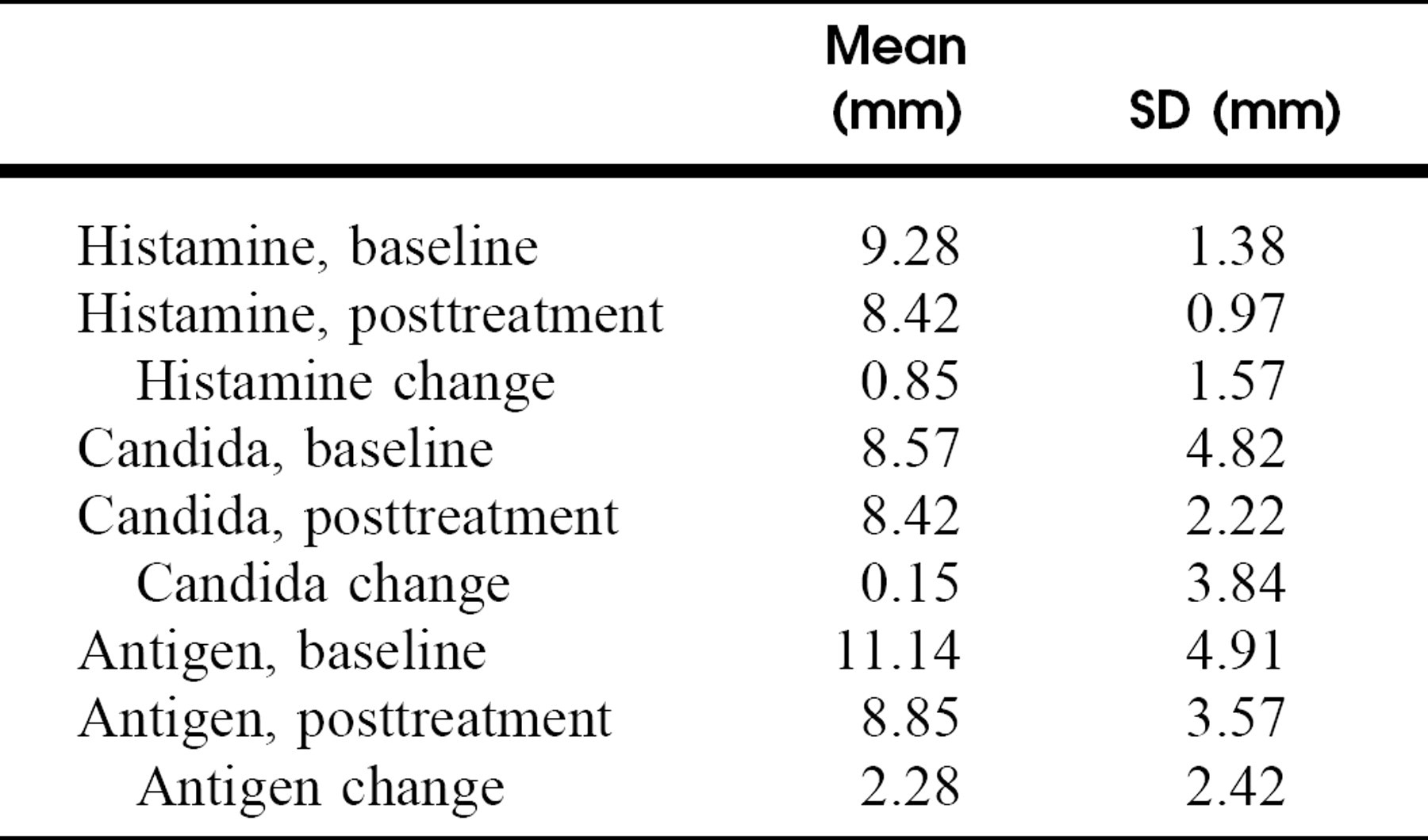
Wheal diameters for placebo
Wheal diameters for change scores
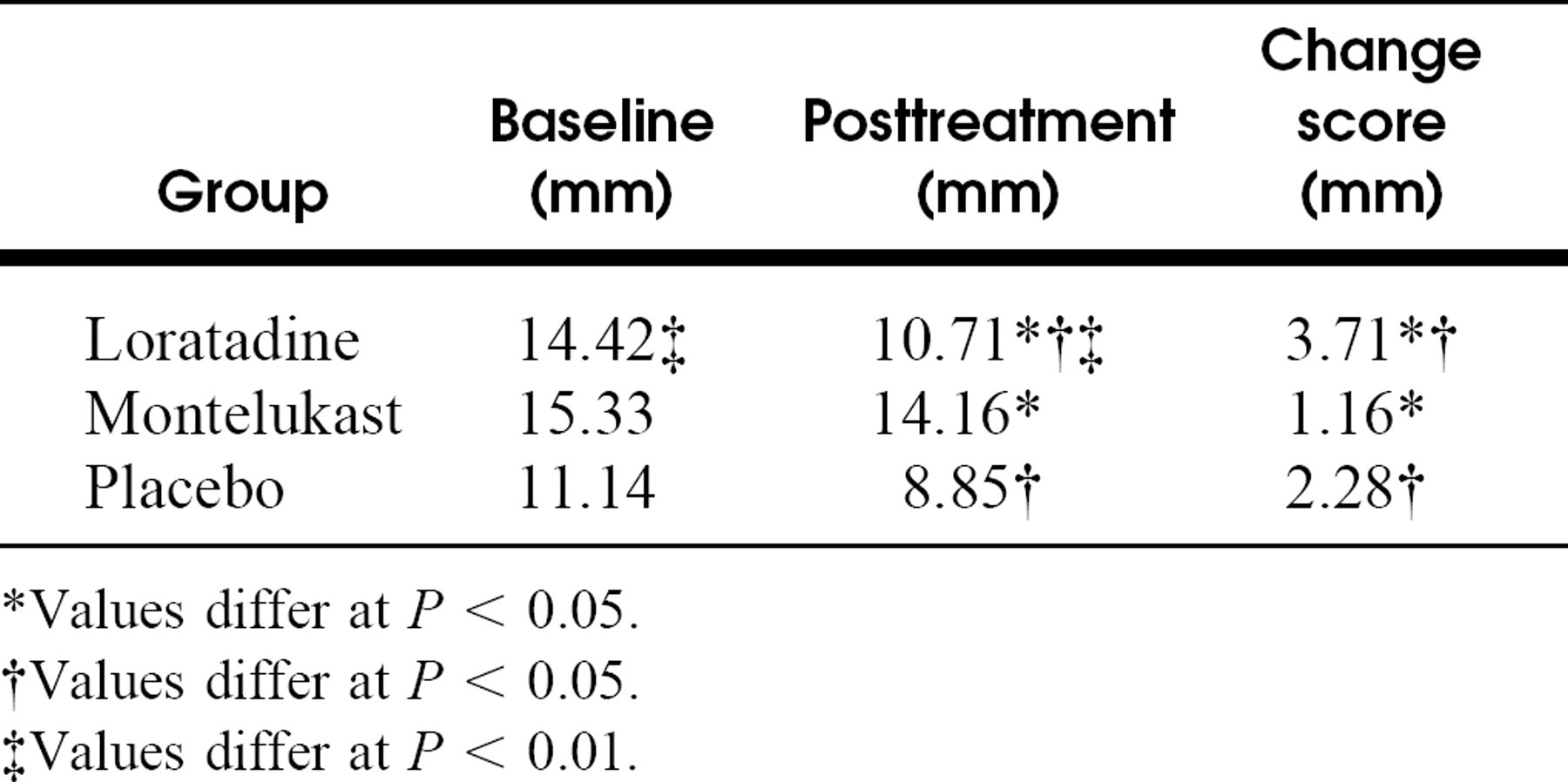
Values differ at P < 0.05.
Values differ at P < 0.05.
Values differ at P < 0.01.
Data Analysis
At the conclusion of the study, all data were tabulated. The difference in whealing from baseline to posttreatment was calculated for each treatment group. Statistical analysis by 2-way analysis of variance (group × time) and post-hoc testing of mean differences were performed to determine the level of significance of the collected data.
RESULTS
A total of 23 subjects were enrolled in the present study. Twenty patients completed the study protocol.
One patient developed a mild systemic allergic response after initial intradermal challenge, 1 patient was unable to tolerate cessation of antihistamine therapy during the course of the study, and 1 patient was lost to follow-up after initial testing.
Tables 1, 2, and 3 show the mean wheal sizes pre/post treatment, change in wheal sizes, and standard deviations (SDs) for the histamine, antigen and Candida intradermal challenges in the 3 treatment groups. An examination of these findings demonstrates that loratadine produced a significant suppression in whealing in response to antigen challenge (F = 14.22, P < 0.01), but not in suppressing the delayed response to Candida antigen. There were no significant reductions in skin whealing with the use of either montelukast or placebo.
Table 4 shows a direct comparison of mean values of antigen-induced wheal sizes at baseline and posttreatment in loratadine, montelukast, and placebo groups. As noted, the loratadine group demonstrated a significant change in wheal size following 1 week of treatment (F = 3.38, P < 0.05) compared with both the montelukast and placebo groups. No significant differences were observed between the montelukast and placebo groups in skin whealing.
DISCUSSION
The assessment of type I hypersensitivity reactions in the skin has been the mainstay of testing for inhalant allergy. Studies have demonstrated that numerous inflammatory mediators are released during these reactions. 2–5 It is well documented in the literature that both histamine and leukotrienes can be found at local reaction sites following skin testing. It is widely accepted that histamine plays a major role in this skin response. However, the potential role of leukotrienes is uncertain at this time and few studies to date have been conducted to further elucidate their function.
Several studies have localized leukotrienes along with other proinflammatory mediators to reaction sites in skin testing. 4–6,9 Research performed by Atkins notes the time course of leukotriene appearance in cutaneous inflammatory responses and suggests that the role of leukotrienes could be in the delayed- or late-phase response. 26 These authors conclude that leukotrienes are of limited importance in immediate allergic skin responses. Other authors have looked at the direct effect of leukotrienes by intradermal injection of these substances. 6–9 This work consistently demonstrates an immediate effect as measured by wheal and flare. However, when compared with responses classically observed with histamine injection or those noted during allergy skin testing, these leukotriene-mediated reactions appear somewhat more variable and tend to be more painful, less pruritic, and of longer duration.
Numerous medications are known to interfere with skin testing. The mechanisms for many of these responses are not known. The variability of these responses makes it difficult to predict the effects of new allergy medications on cutaneous inflammatory responses. The production and role of leukotrienes in allergic asthma and chronic urticaria have prompted great interest in the development of drugs aimed at inhibiting this pathway. Numerous drugs have been developed targeting different aspects of this metabolic cascade. The leukotriene receptor antagonists have recently received much attention due to their clinical efficacy in the treatment of allergic asthma and other allergic diseases. Because there is considerable overlap between the population of patients undergoing skin testing for inhalant allergies and those who may already be taking leukotriene receptor antagonists for other atopic diseases, it is of great importance that their effect on skin testing be established.
As discussed previously, Simons, Johnston, and Gu 22 described the early and late cutaneous responses of 12 atopic patients after intradermal challenge of allergen, histamine, LTD4, and saline control. When comparing montelukast with placebo, no significant effect was reported. 23 Another study recently reported by Cuhadaroglu et al 23 looked at the effects of zafirlukast, another leukotriene receptor antagonist, on skin prick testing in 9 atopic and 8 nonatopic patients. The study concluded that there was no significant effect of zafirlukast on skin prick testing after a 5-day course. However, this study only looked at the effects on skin prick testing, not intradermal testing, and proper controls were not established.
The present study showed that montelukast did not affect the intradermal whealing response in skin after 1 week of use. As would be expected, the greatest antigen-induced wheal suppression was noted in the loratadine group. The montelukast group demonstrated the least suppressive effect, with the placebo group demonstrating an intermediate but nonsignificant level of antigen induced wheal suppression.
This study also attempted to assess the effect of montelukast on any delayed responses induced by intradermal Candida injections. No effect was noted on suppression of delayed whealing with C albicans with either of the study medications or with placebo.
CONCLUSIONS
The present study demonstrated that montelukast failed to cause any suppression of allergy-induced skin whealing using standard intradermal testing techniques with 1:2500 antigen dilutions. Based on the current results, we conclude that montelukast does not need to be discontinued prior to intradermal allergy testing.