
Abstract
OBJECTIVE: This study was designed to explore the changes in patient-relevant clinical outcomes in a selected group undergoing surgery for nasal septal and turbinate abnormalities.
STUDY DESIGN: Seventy-nine consecutive patients with headache and correctable anatomic nasal obstruction were seen at the study institution from March 1998 to May 2000. These patients were evaluated for changes in patient-relevant clinical outcomes measures after surgical correction of their anatomic abnormalities.
RESULTS: Seventy-one patients underwent surgical correction of nasal obstruction. More than half of these patients had contact points preoperatively. Statistically significant improvements were observed in the patient population with respect to 8 of the 10 clinical outcomes measures. Importantly, a decrease in the severity and frequency of headaches was noted after surgery, especially after the correction of contact points.
CONCLUSION: The surgical correction of the septum and turbinates resulted in predictable improvement in headache and a majority of other important outcomes measures.
CLINICAL SIGNIFICANCE: Pain may improve after surgical correction of septal and turbinate abnormalities in a properly selected group.
The most common anatomic abnormalities cited in the literature include septal deviations (due to deflection, buckling, and spurring) and turbinate deformities (conchae bullosae, paradoxical curvature) and hypertrophy. 1-3,5 Often these abnormalities result in contact points between the septum and turbinates. This study was designed to explore the changes in the patient-relevant clinical outcomes in a select group undergoing surgery for anatomic obstruction secondary to nasal septal and turbinate abnormalities.
METHODS
Seventy-nine consecutive patients with headache and anatomic nasal obstruction were seen at the Vanderbilt University Asthma, Sinus, and Allergy Program (ASAP) from March 1998 to May 2000. Before filling out the questionnaire, informed consent was obtained from each patient. All patients underwent a thorough evaluation including completion of the questionnaire, a full head and neck examination, nasal endoscopy, and same-day coronal sinus computed tomography (CT) scanning. Inclusion criteria for the study included (1) a complaint of episodic headaches for longer than 2 months and (2) an anatomic abnormality (nasal septal deviation, turbinate deformity or hypertrophy, and/or a contact point) on physical examination. Exclusion criteria included previous nasal surgery; clinical or radiologic evidence of sinusitis, nasal polyps, or masses; and failure to follow up with completion of the survey. All patients underwent a screening allergy test and additional testing with treatment if found to be allergic. Treatment for allergic rhinitis included avoidance, systemic antihistamines, topical steroid nasal sprays, and immunotherapy when necessary. Those patients thought to have vasomotor rhinitis were treated appropriately with steroid nasal sprays and decongestants. Any patients fitting the above criteria with lack of improvement despite medical management were moved into the surgical group, and all study patients underwent correction of their abnormalities by the senior author (J.D.).
Septoplasty was performed in the typical fashion with removal of the deviated cartilaginous and bony septum, as well as any bony spur involvement in the maxillary crest. In the case of the hypertrophied or deformed middle turbinate, a middle turbinectomy was performed using turbinate scissors to cut the vertical attachment and a straight-through bite to remove the horizontal attachment. Approximately one third of the middle turbinate was left remaining after middle turbinectomy. In those patients with enlarged or deformed inferior turbinates, we used a suction-bovie to cauterize the inferior-medial portion of the turbinate, followed by lateralization with a nasal fracture elevator. No other surgical intervention, such as sinus surgery, was performed on any patient.
The Vanderbilt ASAP center questionnaire includes portions of 2 valid and reliable clinical outcomes measures of nasal and paranasal sinus symptoms (Fig 1). Questions from the Rhinosinusitis Outcomes Measure (RSOM-31) 6 and the Rhinoconjunctivitis Quality of Life Questionnaire 7 have been adapted into a standard questionnaire completed by each patient for every visit. Patients completed the standard questionnaire and rated their symptoms from 0 (not troubled) to 6 (extremely troubled) using a Leikert severity scale. Although the Vanderbilt ASAP questionnaire has not been validated to produce a clinically relevant total score, the questions on this survey are thought to have validity on an individual basis.
RESULTS
Seventy-nine patients with headache and anatomic nasal obstruction underwent surgery after maximal medical therapy demonstrated no benefit. Eight patients were excluded because of inadequate follow-up. Seventy-one patients (32 men and 39 women; age range, 18 to 64 years) were followed for an average of 21 months (16.7 months postoperatively). All patients underwent surgical correction of their anatomic abnormalities. In total, the 71 patients required 69 septoplasties, 36 unilateral turbinate reductions, and 25 bilateral turbinate reductions.
At the initial presentation, all patients complained of headache, and 39 (55%) patients listed headache as their chief complaint. Although 11 patients (15%) complained of exclusively unilateral headaches, a history of predominantly unilateral headaches was experienced in 48 patients (68%). Twelve of the 71 patients described bilateral headaches. In an attempt to localize the pain of their headaches, most described frontal pain (83%), whereas other less common sites were retro-orbital (26%), temporal (22%), and maxillary (22%).
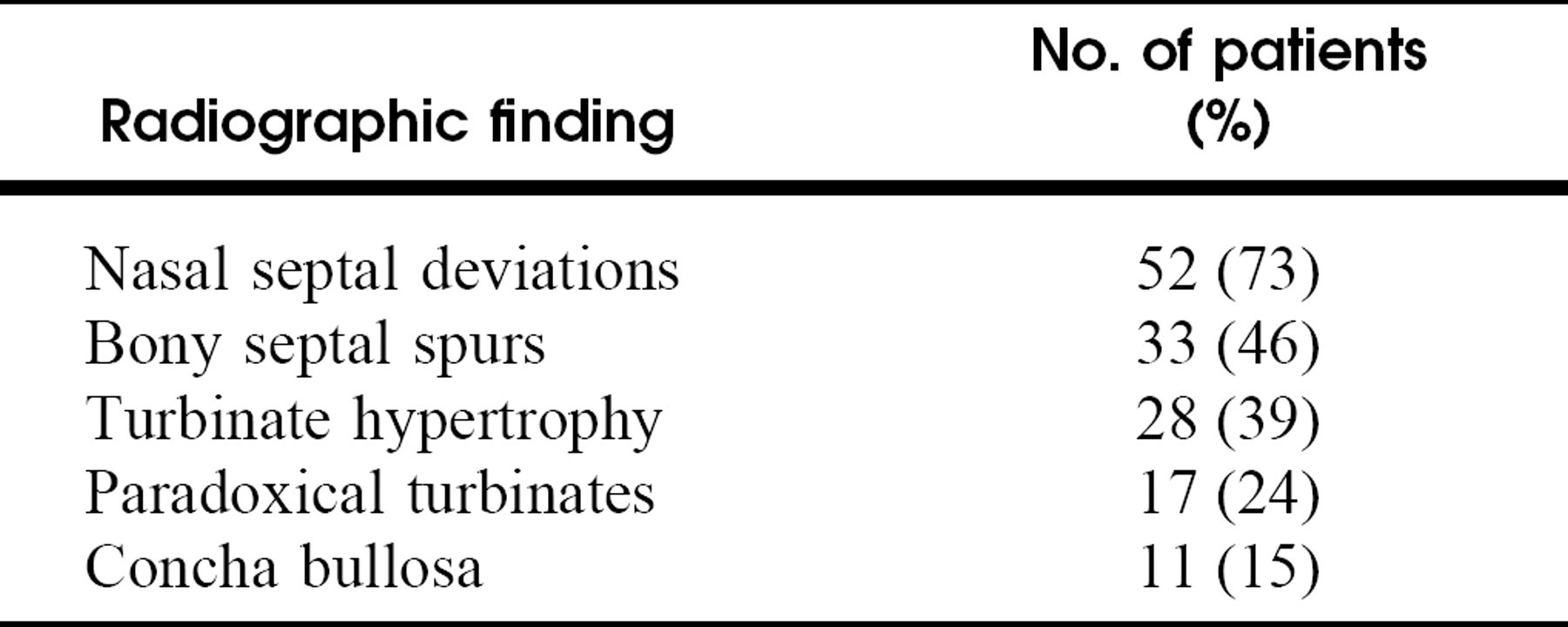
All patients had an anatomic abnormality of the septum noted on their initial examination and/or CT scan. Radiographic demonstration of anatomic abnormalities can be found in Table 1. Some patients were thought to not have significant septal deviation radiographically (27%). However, many of these patients had a significant enough amount of septal deviation or bony spurring clinically to require septoplasty.
Statistically significant improvements were observed in the entire patient population with respect to 8 of the 10 clinical outcomes measures (Figs 2 and 3), including headache during the past 1 week (P < 0.001) and 8 weeks (P < 0.001), facial pain (P < 0.01), nasal obstruction (P < 0.01), patient frustration (P < 0.001), irritability (p < 0.001), restlessness (P < 0.001), and embarrassment (P < 0.001). No significant change was found in the symptoms of eye soreness (P = 0.19) or tooth pain (P = 0.7).
Substantial benefits were also recognized in the group with mucosal contact points. These patients totaled 43 and represented 61% of the entire group. When questioned regarding headache at 1-year follow-up, 19 (44%) patients with contact points denied headache during the past week, whereas 18 (42%) reported an extended headache-free period of at least 8 weeks.
DISCUSSION
Before surgery, our patients complained of many of the same problems other investigators have confronted: chronic, recurrent, and predom-inantly unilateral headaches, always in association with nasal obstruction and often in conjunction with restlessness and irritability. 2,3,8 In addition, these patients were refractory to medical therapy aimed at increasing nasal airflow and decreasing obstruction. We have found that the surgical correction of obvious anatomic abnormalities in carefully selected patients can significantly improve several important clinical outcomes, including headache. These anatomic abnormalities most commonly at fault include deviation of the nasal septum, septal spurring, and deformed or hypertrophied turbinates.
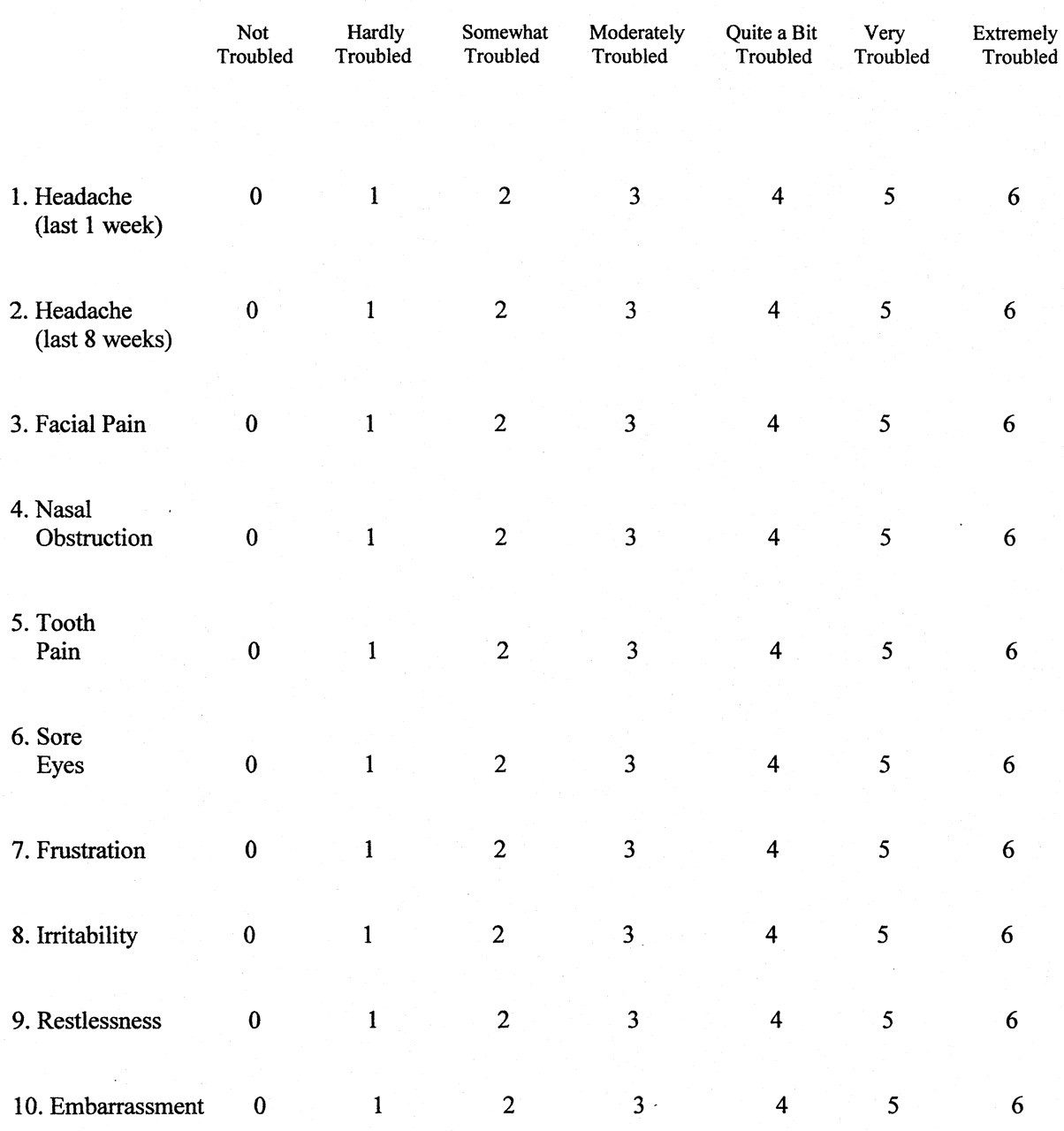
Sample ASAP questionnaire.
Radiographic abnormalities in the study group (N = 71)
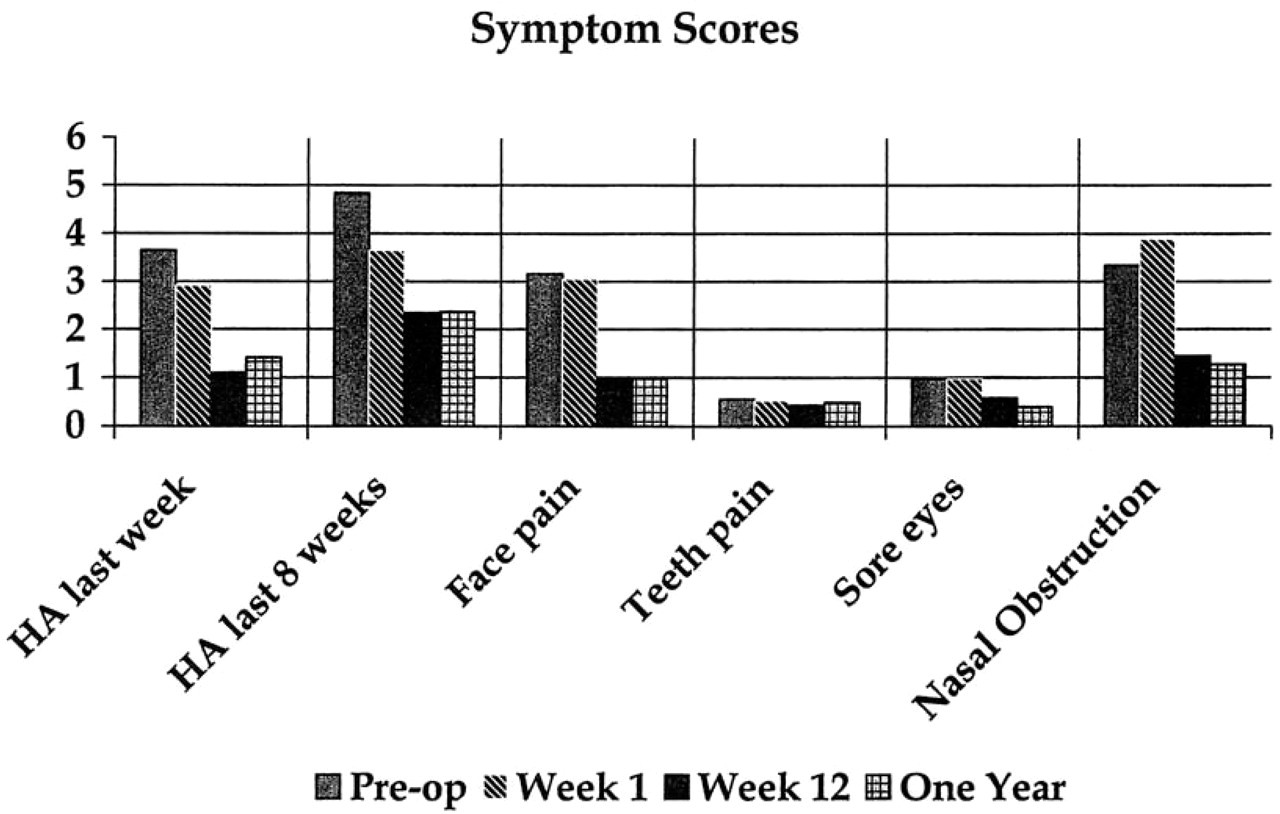
Mean physical symptom scores for the group preoperatively and 1 week, 3 months, and 1 year postoperatively.
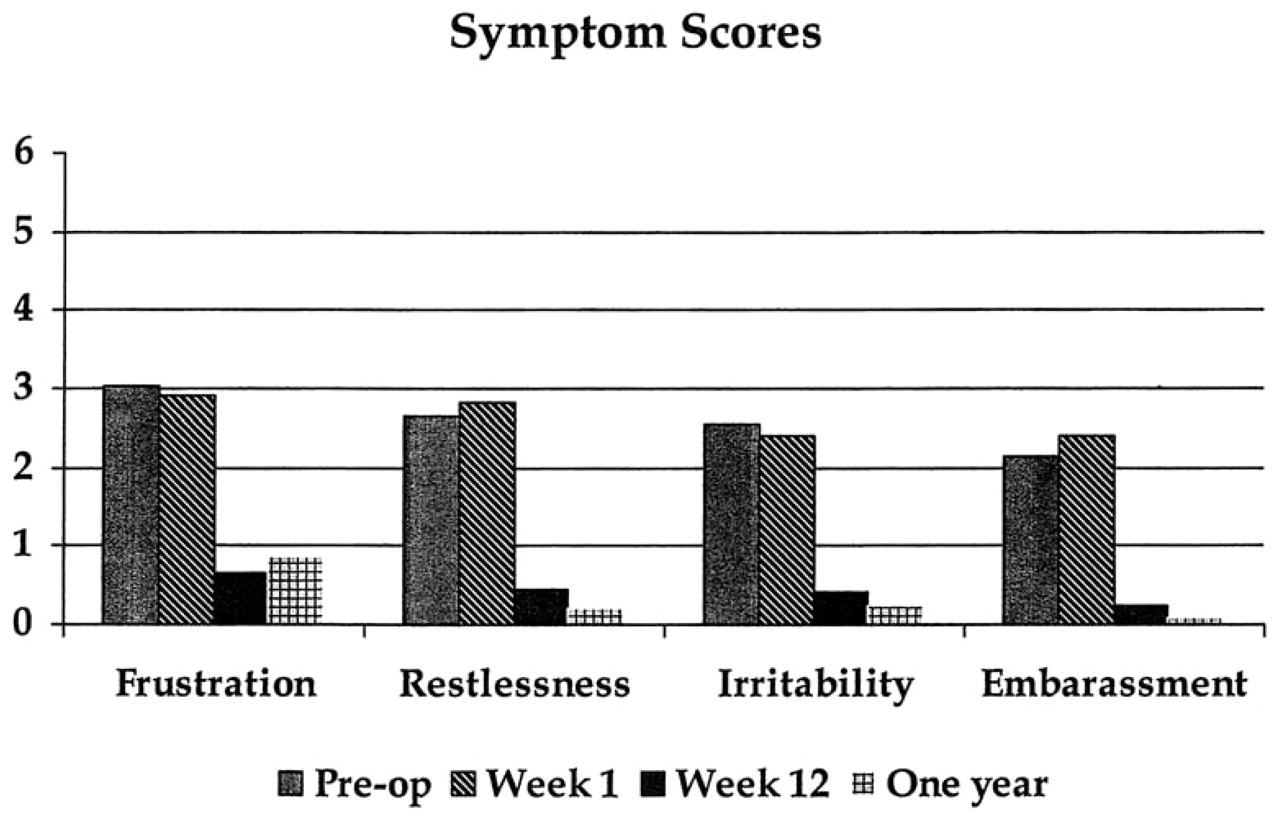
Mean emotional symptom scores for the group preoperatively and 1 week, 3 months, and 1 year postoperatively.
Although radiographic findings were helpful in evaluating our patients, we agree with Parsons and Batra 3 that there are no “absolutes” present on preoperative CT scanning predictive of the degree of success. When clinical examination alone indicated anatomic obstruction, we chose to surgically correct the abnormality, even if radiographic studies did not demonstrative any abnormal finding. With regard to positive CT findings, we discovered that in many cases unilateral headaches were associated with the radiographic finding of significant septal spurring on the side of the headache. In removing these spurs, especially those resulting in a contact point with the inferior turbinate, we saw a substantial relief of pain and improvement in symptoms.
The surgical correction of these abnormalities benefited the patients according to the patient-relevant clinical outcomes measures used here. Although Figures 2 and 3 present the data in terms of numerical value, responses to the ASAP questionnaire provide a better qualitative description of changes in patient symptoms than do these quantitative scores. The possible responses to the questions on the questionnaire correspond to the following: 0, not troubled; 1, hardly troubled; 2, somewhat troubled; 3, moderately troubled; 4, quite a bit troubled; 5, very troubled; and 6, extremely troubled. Preoperatively, the average scores for those patients with headache over the past 1 week and past 8 weeks approached “quite a bit troubled” and “very troubled,” respectively. Postoperatively, as a whole this group is now “hardly troubled” by headache. Additionally, many of the subjects experienced complete relief, especially those who previously had contact points. As a group, these patients were better rested, less irritable, and less frustrated after undergoing surgery.
The conventional study of rhinogenic pain has been difficult because of the varied nature of patients' complaints, the presence of comorbidities, and the lack of objective physical findings to follow. Patient-relevant clinical outcomes, however, are helpful in measuring the change in patient experiences even in the face of many perplexing variables. In our group, the surgical correction of anatomic abnormalities of the septum and turbinates, particularly contact points, resulted in predictable improvement in patient-relevant outcomes measures with regard to headache severity and frequency, nasal obstruction, and level of patient frustration, irritability, and restlessness.
The authors thank Lou Reinisch, PhD, for assisting with statistical analysis.
As a service to our subscribers, copies of back issues of Otolaryngology-Head and Neck Surgery for the preceding 5 years are maintained and are available for purchase from Mosby until inventory is depleted. The following quantity discounts are available: 25% off on quantities of 12 to 23, and one third off on quantities of 24 or more. Please write to Mosby, Subscription Customer Service, 6277 Sea Harbor Dr, Orlando, FL 32887, or call 800-654-2452 or 407-345-4000 for information on availability of particular issues and prices. If unavailable from the publisher, photocopies of complete issues may be purchased from ProQuest Information and Learning, 300 N Zeeb Rd, Ann Arbor, MI 48106-1346; phone, 734-761-4700 or 800-521-0600.