
Abstract
Vocal fold granulomas are benign but frequently recurrent lesions that can cause frustration for both the patient and the treating physician. Etiologic factors include endotracheal intubation, vocal abuse, and gastroesophageal reflux. Conventional treatment for granulomas has included medical, voice, and surgical therapy, none with uniform success. In this study 8 patients with vocal fold granulomas were treated with intralaryngeal injection of botulinum toxin. The resultant temporary paresis of the vocal folds allowed for a window of time during which the vocal process could heal and the granulomas could resolve without being exposed to ongoing intermittent contact and friction with the opposing arytenoid. Although the underlying cause of a granuloma must also be addressed, we have found that botulinum toxin can be a useful adjunct to traditional therapy and can lead to avoidance of repetitive surgical procedures.
The pathogenesis of vocal fold granulomas is still debated. Etiologic factors including endotracheal intubation, 2 vocal abuse, 3 habitual throat clearing, 4 gastroesophageal reflux (GER), 5 low-pitched voice, 6 and psychosomatic disorders 7 have all been cited. Smoking, postnasal drip, and throat infections may also be causative agents. A mechanical basis was first proposed by Jackson and Jackson, 8 who suggested that superficial ulceration and focal granulation result from a “hammer and anvil” action between the vocal processes.
Many different therapeutic approaches to vocal fold granulomas have been used, but none with uniform success. Voice rest, speech therapy, antibiotics, corticosteroids (injected, inhaled, or parenteral), antireflux therapy, and surgical removal have all been used, none with a distinct advantage. Often, multiple surgical procedures are needed to eradicate the granulomas, whether performed with cold excision, laser vaporization, or cautery.
This study examines the results of a new approach to treating vocal fold granulomas with intralaryngeal injections of botulinum toxin.
METHODS AND MATERIAL
To date, 8 patients with recurrent vocal fold granulomas have been treated with botulinum toxin. All of the patients had undergone at least 1 (and up to 5) surgical procedure with excision of their granulomas and confirmation of benign, inflammatory histology. All patients were male nonsmokers, and their granulomas were attributed to 1 or more of the following causes: intubation (2 patients), GER (4), vocal abuse (1), blunt neck trauma (1), inhalation injury (1), adductor spasmodic dysphonia (1), and upper respiratory tract infection (1). Every patient had 1 or more of the following symptoms: foreign-body sensation in the throat, vocal fatigue, vocal weakness, throat soreness, cough, hemoptysis, or hoarseness.
Botulinum toxin type A (Botox A; Allergan Inc, Irvine, CA) was injected into 1 or both (ie, right and/or left) thyroarytenoid muscles by the transcutaneous route. Two patients received supplemental injections of botulinum toxin through direct laryngoscopy when granuloma excision was performed. Dosage ranged from 1.25 to 20 U of neurotoxin per injection, with an average of 10 U per injection. Informed consent was obtained from all patients, after they were counseled with regard to the potential for irreversible changes in the muscles into which the botulinum toxin would be injected. Botulinum toxin was used with institutional knowledge and approval of the University of California, San Diego. All injections in the awake patients were performed transcutaneously with insulated injection needles and electromyographic confirmation of needle placement. Patients were asked to phonate /i/, and activation of the thyroarytenoid muscle was confirmed by the presence of motor unit potentials. The 2 injections that were performed during general anesthesia through direct laryngoscopy were placed lateral to the free edge of the vocal fold under direct microscopic visualization. The minimum estimated dose of botulinum toxin sufficient to induce thyroarytenoid paresis that prevented contact between the vocal processes during vocal fold adduction was used. Follow-up examination and interview confirmed whether adductor paresis was achieved, and in the 4 patients who had persistent vocal process contact despite partial paresis, 1 or (in 1 patient) 2 supplemental injections were administered. One patient received bilateral thyroarytenoid injections as initial treatment for both adductor spasmodic dysphonia and vocal fold granuloma. Two other patients received bilateral injections in a sequential fashion (ie, right thyroarytenoid injection with subsequent left thyroarytenoid injection) because of persistent vocal process contact.
Results of botulinum toxin injection therapy for vocal fold granuloma in 8 patients
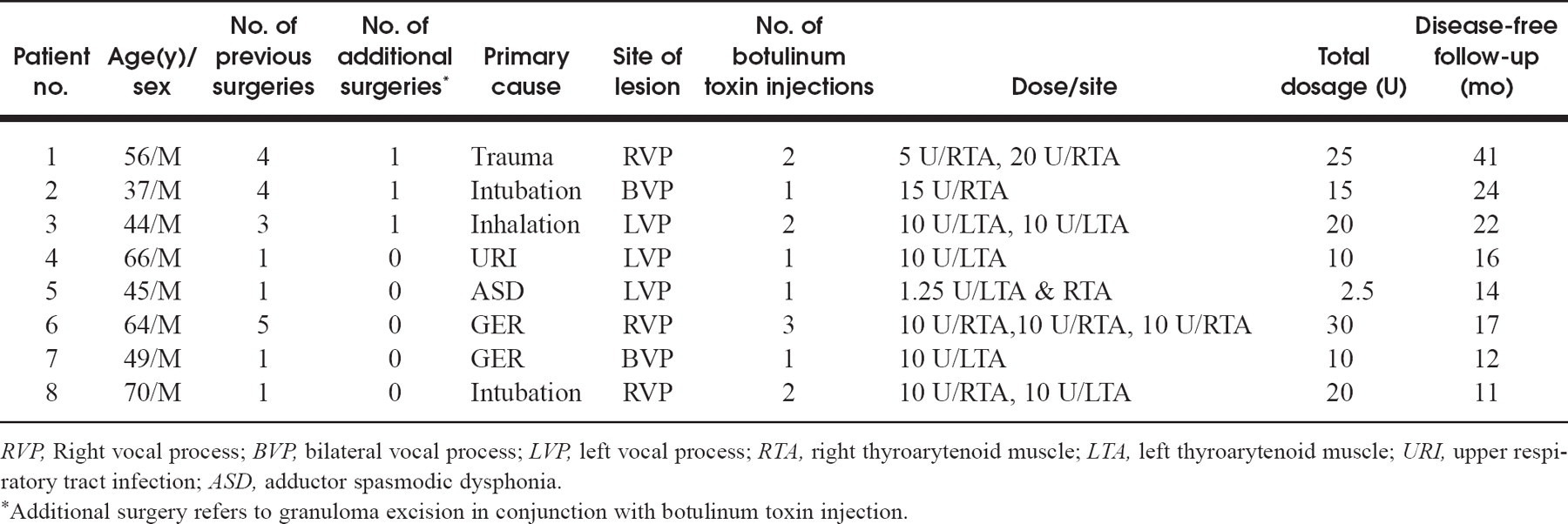
RVP, Right vocal process; BVP, bilateral vocal process; LVP, left vocal process; RTA, right thyroarytenoid muscle; LTA, left thyroarytenoid muscle; URI, upper respiratory tract infection; ASD, adductor spasmodic dysphonia.
∗Additional surgery refers to granuloma excision in conjunction with botulinum toxin injection.
Patients with GER were also treated with behavior modification and medical therapy. Behavioral measures included avoiding provocative dietary agents (coffee, alcohol, chocolate, acidic foods, fried foods, spicy foods, etc), increasing the interval between dining and sleeping, reducing stress, and elevating the head of the patient's bed. Medical therapy consisted of routine use of ranitidine or omeprazole. The diagnosis of GER was made on the basis of history and physical examination, and it was confirmed by response to antireflux therapy. One patient in this group underwent 24-hour pH monitoring and esophagogastroduodenoscopy after successful treatment of his granuloma because of breakthrough symptoms of reflux despite ongoing medical and behavioral therapy. Three other patients were maintained on antireflux therapy after granuloma resolution on the basis of their histories, examinations, and improved well-being while receiving medical therapy.
Patients with vocal abuse or misbehavior were also treated with individual voice therapy by one of us (S.N.G., a speech pathologist).
RESULTS
Results are summarized in table 1. Unilateral and bilateral vocal fold granulomas resolved in all patients within 8 weeks. The first 3 patients treated with botulinum toxin were also treated surgically for recurrent vocal fold granuloma. Their lesions were excised by direct microlaryngoscopy, and none recurred despite up to 4 previous recurrences. Encouraged by these early successes after excision in conjunction with botulinum toxin therapy, the next 5 patients were treated with botulinum toxin and medical or behavioral management only, without additional surgery. In these patients the granulomas resolved without surgical excision. A second injection of botulinum toxin was needed in 4 patients, and a third injection was needed in 1 patient, because all of these patients continued to show vocal process contact and friction despite partial weakening of their thyroarytenoid muscles. Ultimately, sufficient adductor paresis was induced in all patients to allow vocal process healing to occur without contact by the opposing vocal process.
There have been no granuloma recurrences in this group of patients, with a minimum follow-up of 11 months and a maximum follow-up of 41 months.
DISCUSSION
Because vocal fold granulomas are usually the result of several additive insults, their treatment should be multidimensional. Identifying and eliminating the cause or causes is the most important step in treating granulomas and in preventing their recurrence. For this reason, speech therapy is often used in an effort to improve vocal hygiene and minimize vocal abuse as a contributing or perpetuating behavior. Vocal behavior modification that eliminates the “hammer and anvil” phenomenon of vocal process contact is one key to reducing reoccurrence.
Most of the patients in this study were also treated with some sort of regimen to eliminate GER as an initiating or promoting factor. When a patient's history is suggestive of GER, behavior modification to prevent reflux and medical therapy (with antacids, H2-receptor blockers, proton pump inhibitors, and/or promotility agents) are appropriate. We empirically treated 7 of our patients with antireflux medication (ranitidine or omeprazole) in conjunction with botulinum toxin injection therapy after these patients' granulomas had failed to resolve with prior antireflux therapy in conjunction with surgery. Four of these patients have been receiving medical therapy for chronic GER disease after granuloma resolution.
Surgical treatment of vocal fold granulomas generally eliminates the lesion but not the cause; therefore the recurrence rate is greater than 50%. 9 No distinct advantage of CO2 laser excision over cold excision has been demonstrated. Surgery is indicated only to remove obstructive lesions and lesions that cause repetitive throat clearing that perpetuates the granuloma, or to treat suspected malignancy.
Voice rest is often prescribed, either before or after surgery. However, avoiding phonation does not prevent adduction and contact of the arytenoids, which occurs during swallowing and coughing. The goal of completely eliminating apposition of the vocal processes was the impetus for injecting botulinum toxin into the adductor muscles of the larynx.
Botulinum toxin is a peptide protease that binds specifically and noncompetitively to the presynaptic cell membranes of cholinergic neurons. 10 The toxin blocks acetylcholine release through zinc-dependent cleavage of protein components of the neuroexocytosis apparatus and causes weakness in the muscles into which it is injected. The motor end plates to which the toxin is bound are irreversibly changed, and such changes are identifiable on repeat electromyography. The effects of botulinum toxin, however, are gradually overcome as axonal outgrowth occurs by collateral and noncollateral sprouting that results in reinnervation. 11 Thus few patients will have permanent clinical voice changes. During the last decade, botulinum toxin injections have become the treatment of choice for a number of movement disorders, including spasmodic dysphonia. 12 As with injections for spasmodic dysphonia, botulinum toxin injection for vocal fold granulomas is an off-label use of this medication, and patients are counseled accordingly. Since we first applied botulinum toxin to the treatment of vocal fold granuloma, we have noted the success of Nasri et al 13 in implementing a similar approach to treating vocal fold granulomas using botulinum toxin in 6 patients.
Unlike the need for serial intralaryngeal injections of botulinum toxin to suppress the symptoms of spasmodic dysphonia, it appears from our preliminary results that no additional botulinum toxin therapy is necessary once patients with granulomas have resolution of their lesions. Four of our patients did require more than 1 injection of botulinum toxin within the first few weeks after their first injection, to induce sufficient adductor paresis. We typically injected the thyroarytenoid muscle on the side of the dominant lesion, but when vocal process contact persisted, we subsequently injected the contralateral thyroarytenoid in 2 patients. Interestingly, both vocal fold granuloma and adductor spasmodic dysphonia were diagnosed simultaneously in 1 of our patients, who continues to receive botulinum toxin therapy for his spasmodic dysphonia without any evidence of granuloma recurrence to date. Elimination of the overly forceful adduction of the vocal folds and arytenoids in this patient seems to be addressing the cause of his secondary lesion. It is worth repeating that ongoing management of other contributing factors such as GER 4 and vocal misbehavior 14 is essential to ensure prevention of recurrent vocal process inflammation and granuloma formation. Thus, in our patient group, those with GER disease continue to receive medical treatment for this condition, and recurrent granulomas have not developed in any.
The potential side effects of intralaryngeal botulinum toxin include breathiness of voice, dysphagia, local pain, aspiration, and decreased efficiency of the Valsalva maneuver. We observed mild-to-moderate breathiness in 7 of our 8 patients, and 1 reported decreased Valsalva effect. No other complications occurred, and patients were counseled before treatment about the likelihood of a temporary weakening of the voice, which resolved within 4 months in all patients.
CONCLUSION
In our series of 8 patients treated with intralaryngeal botulinum toxin, we have observed a 100% success rate in eliminating vocal fold granulomas that have been refractory to more traditional forms of therapy. Five of our toxin-treated patients showed resolution of their vocal process lesions without additional surgical intervention; 3 of our patients avoided re-recurrence after multiple failed surgeries through the use of botulinum toxin in conjunction with surgical excision and appropriate medical and behavioral therapy directed against GER and vocal abuse. Although ongoing follow-up is required to be certain of cure, these results suggest that, when friction and contact are eliminated as perpetuating factors and underlying causative agents are controlled, vocal fold granulomas can be reversed and prevented even in refractory cases.