
Abstract
The ototoxicity induced by cisplatin results in high-frequency hearing loss. The sound-pressure thresholds at extended high frequencies of 8 to 20 kHz were measured in 12 patients with head and neck cancer before and after the first administration of cisplatin. Ototoxicity was defined statistically by the newly introduced regression-line analysis. This analysis revealed that the threshold of 1 of the 12 patients increased evenly from 8 to 10 kHz, and the damage to the hearing system of this patient was permanent. The reasons for such a low rate of ototoxicity might be the long-term administration of low doses of cisplatin and the addition of fosfomycin.
In 1965 Rosenberg et al 1 observed that inorganic platinum compounds inhibit cell division in Escherichia coli. Several neutral platinum compounds were subsequently found to have antitumor activity. Cis-diamminedichloroplatinum II (cisplatin) has been the most extensively used derivative. In recent years, it has been an efficient chemotherapeutic agent against a wide variety of tumors, including testicular cancer, gynecologic cancer, bladder cancer, and squamous cell carcinoma of the head and neck. The most commonly reported severe side effects of the chemotherapeutic treatment have been myelosuppression, neurotoxicity, nausea, nephrotoxicity, and ototoxicity. The ototoxicity has consisted of tinnitus with and without hearing loss, symptomatic hearing loss, and most frequently, asymptomatic high-frequency hearing loss.
Despite the general agreement that cisplatin has ototoxic potential, the auditory status of many patients receiving this drug is monitored during treatment. Moreover, most ototoxic monitoring studies have not included a threshold evaluation of frequencies above 8 kHz. 2-4 Only a few investigators have reported ototoxicity measured in the extended high-frequency (EHF) range above 8 kHz. 5,6 In addition, individual audiometric hearing change has been neither defined clearly nor analyzed statistically. A new statistical analysis is required to evaluate individual ototoxicity.
The purpose of this investigation was to examine the potential ototoxic effects of cisplatin on audition at frequencies above 8 kHz. We monitored patients before and after administration of cisplatin for evidence of any changes in hearing sensitivity in the EHF range.
METHODS AND MATERIAL
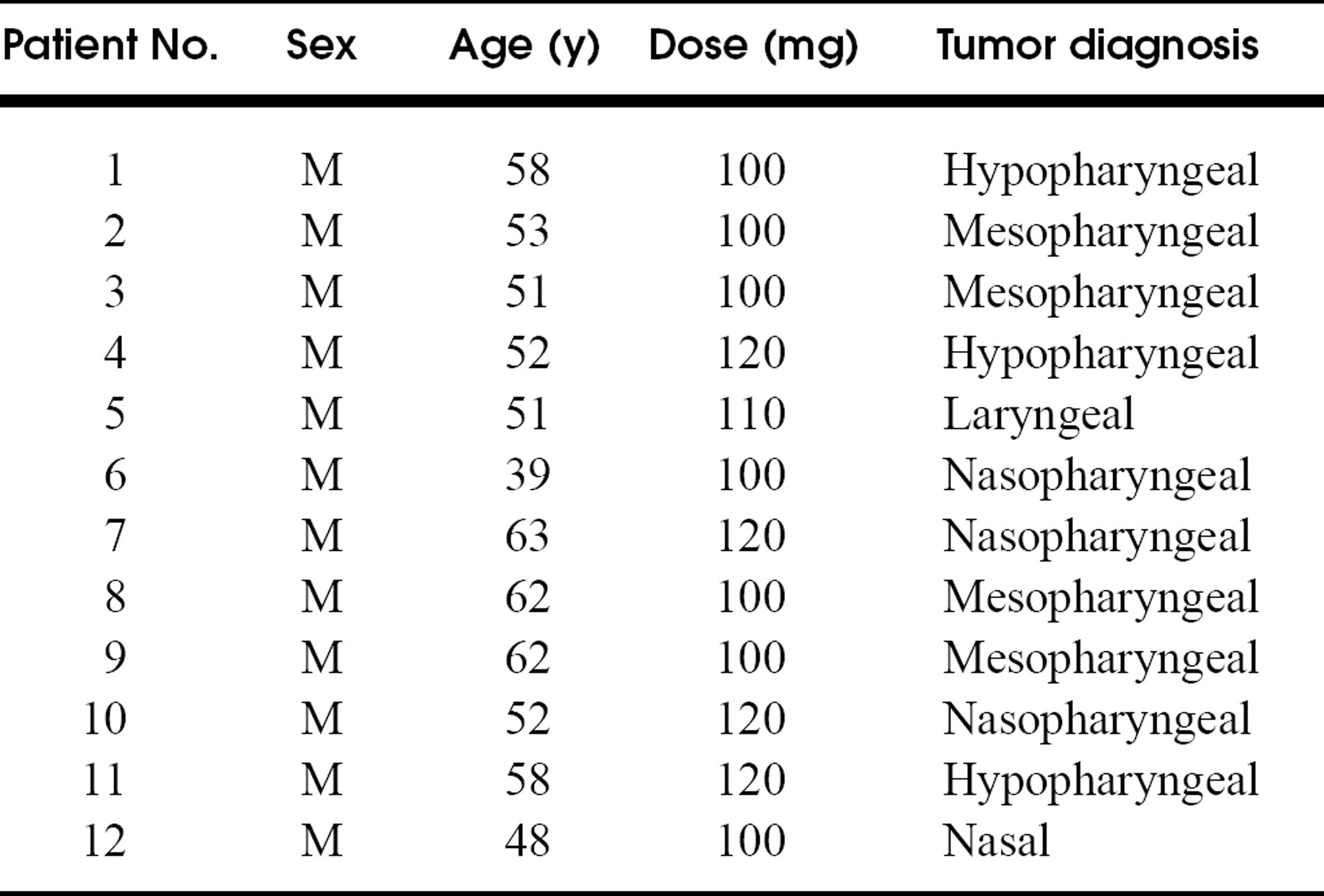
Subjects eligible for the study were all head and neck cancer patients undergoing their first cisplatin administration from August 1994 to January 1995 at the Department of Otolaryngology, University of Tokyo Hospital. Review and approval of the protocol were performed by the local institutional review board, and informed consent was obtained from each subject. All subjects were tested at conventional audiometric frequencies (125, 250, 500, 1000, 2000, 4000, and 8000 Hz). Their thresholds at these frequencies were judged to be within normal limits based on the age- and sex-based norms of ISO 7029. 7 In addition, individuals participating in the study had no prior history of significant hearing difficulties or noise exposure, showed no evidence of metastatic disease, and had not undergone radiotherapy to the temporal bone. Ototoxic drugs were limited to cisplatin. Subjects who could not be measured after administration because of strong nausea were also excluded. Of a total of 19 patients screened in this manner, 12 were chosen (Table 1). Coincidentally, all subjects were men, and all 24 ears were acceptable for the subsequent EHF tests. Each ear canal was cleaned before measurement.
A Rion audiometry (model AA-61B; Rion Co Ltd, Kokubunji, Tokyo, Japan) was used for conventional audiometry. The electrodynamic earphone was a Rion AD-02 with rubber supra-aural cushions. The calibration of acoustic output levels was performed with a coupler (IEC 318 type B&K 4153).
A Demlar EHF audiometer (model 20K; Demlar Medical Inc, Chapel Hill, NC) was used for measurement of EHF audiometry. This EHF audiometer covers a frequency range from 8 to 20 kHz in 1-kHz steps, and its signal intensity can be varied from 0 to 120 dB SPL in 1-dB steps. The tone burst was accepted as the stimulus wave because of its easy recognizability; the length of the tone burst was shortened to 250 ms and repeated every 400 ms. This audiometer is equipped with an electrodynamic high-fidelity earphone (Koss HV/1A Plus) with soft sponge supra-aural cushions. The frequency characteristics of this earphone are rather flat at higher frequencies, but it gains about 20 dB at 5 kHz.
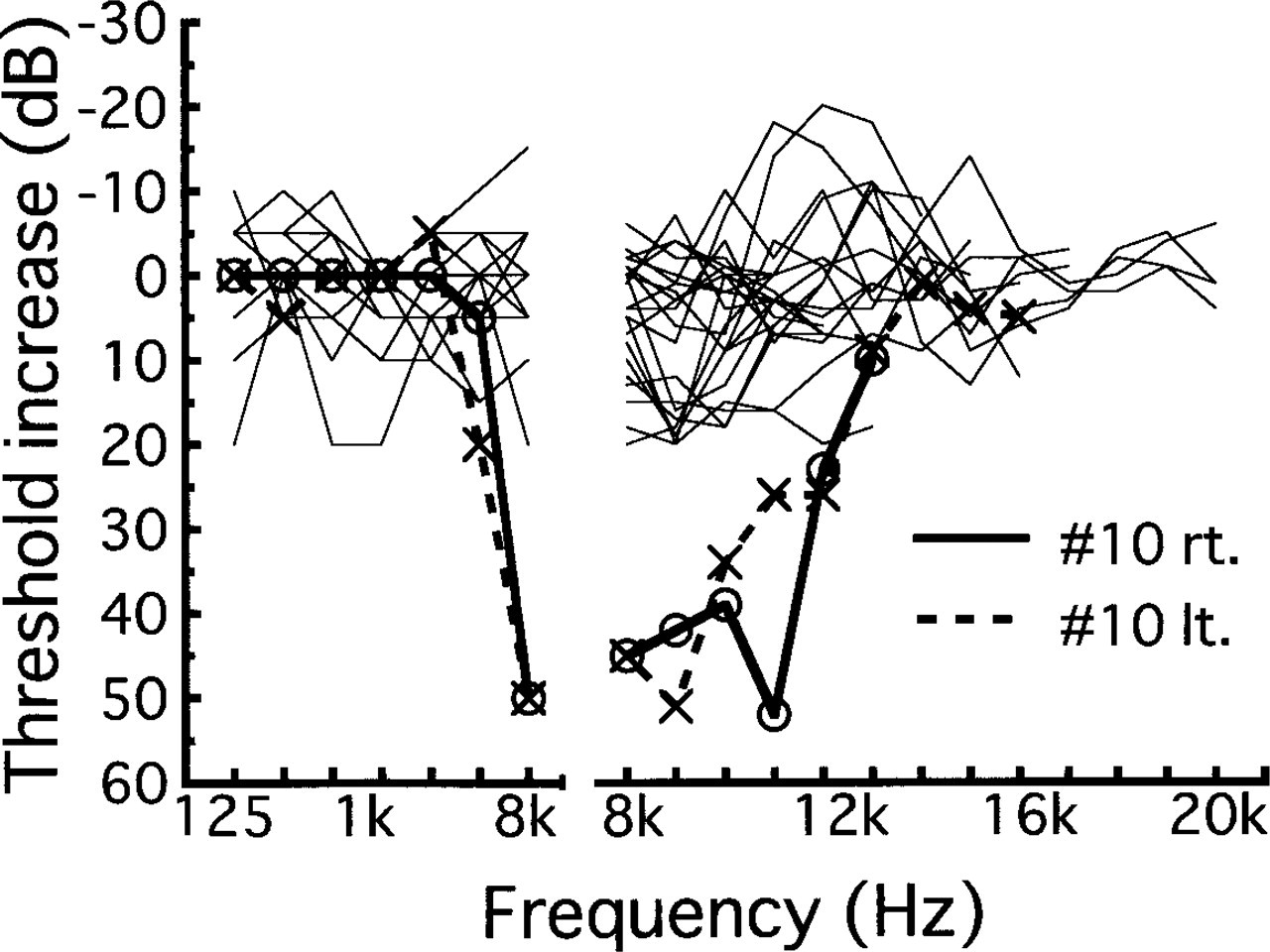
Increase rate of thresholds after administration of cisplatin on each subject compared with before administration. rt., Right; It., left.
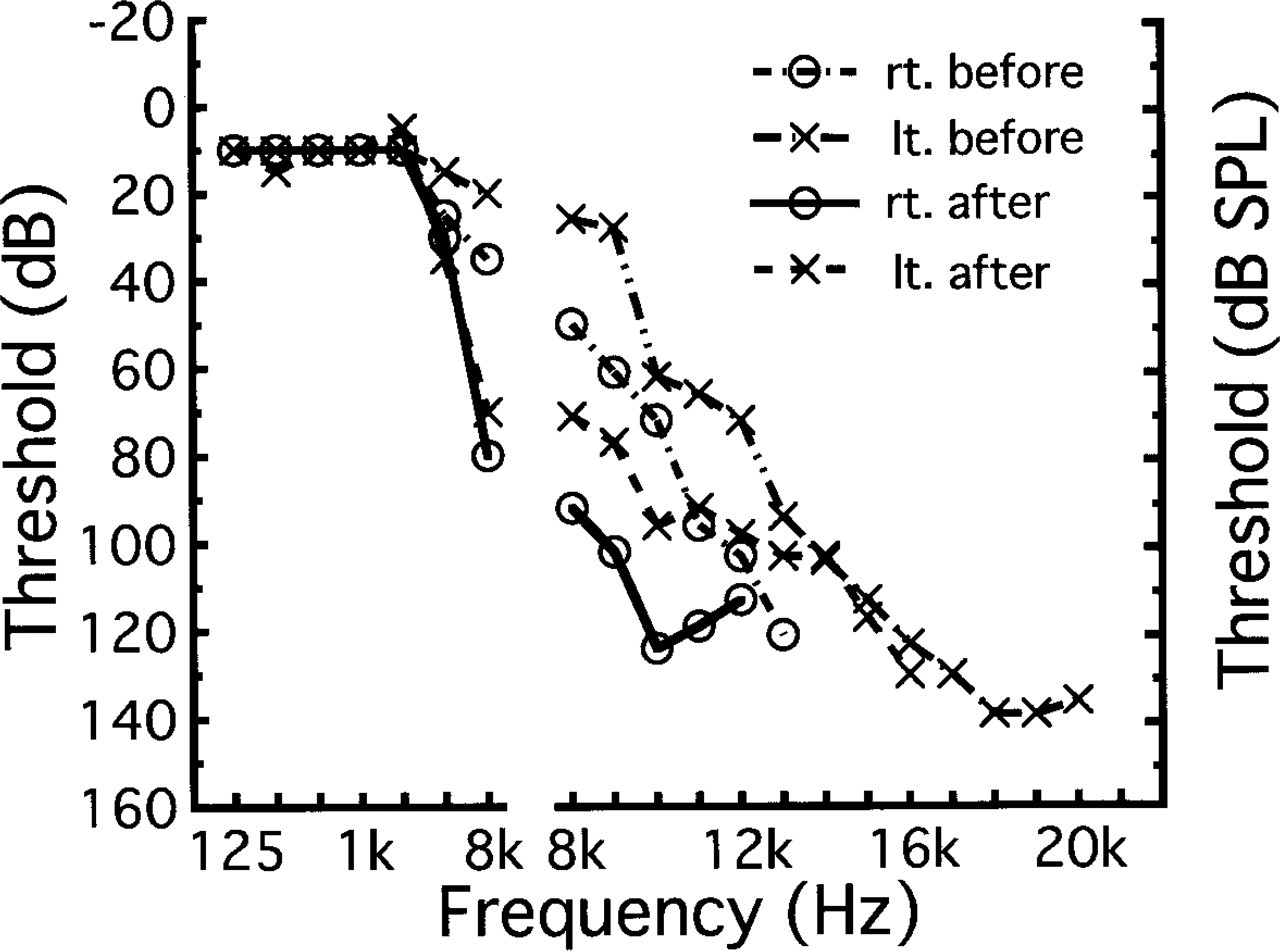
Threshold change at conventional audiometric frequencies and EHF in the patient who had ototoxicity before and after administration of cisplatin. rt., Right; It., left.
The calibration of acoustic output levels was also performed with a conventional coupler (IEC 318 type B&K 4153). The calibrated values are presented in the Results section. Contralateral masking was not used.
All measurements were conducted in an audiometric room fulfilling the criteria of ISO 8253-1 8 for measuring hearing thresholds down to 0 dB HL in the 125- to 8000-Hz range.
Measurements were performed before and 4 days after the administration of cisplatin. The dose of cisplatin was 70 mg/m2 body surface, with an upper limit of 120 mg per body (Table 1). Dexamethasone was administered venously for nausea at 16 mg/day for 2 days, and fosfomycin was administered at 4 g/day for nephrotoxicity and ototoxicity for 5 days.
The regression-line analysis is available for statistical analysis of individual threshold data. The threshold regression lines were calculated by the method of least squares on the following ranges of frequencies: 8 to 10 kHz and 14 to 19 kHz. To avoid threshold data at about 12 kHz and above 19 kHz, we divided the measurements into 2 ranges of frequencies. Slope and intercept were defined as follows, where f is frequency in kilohertz:
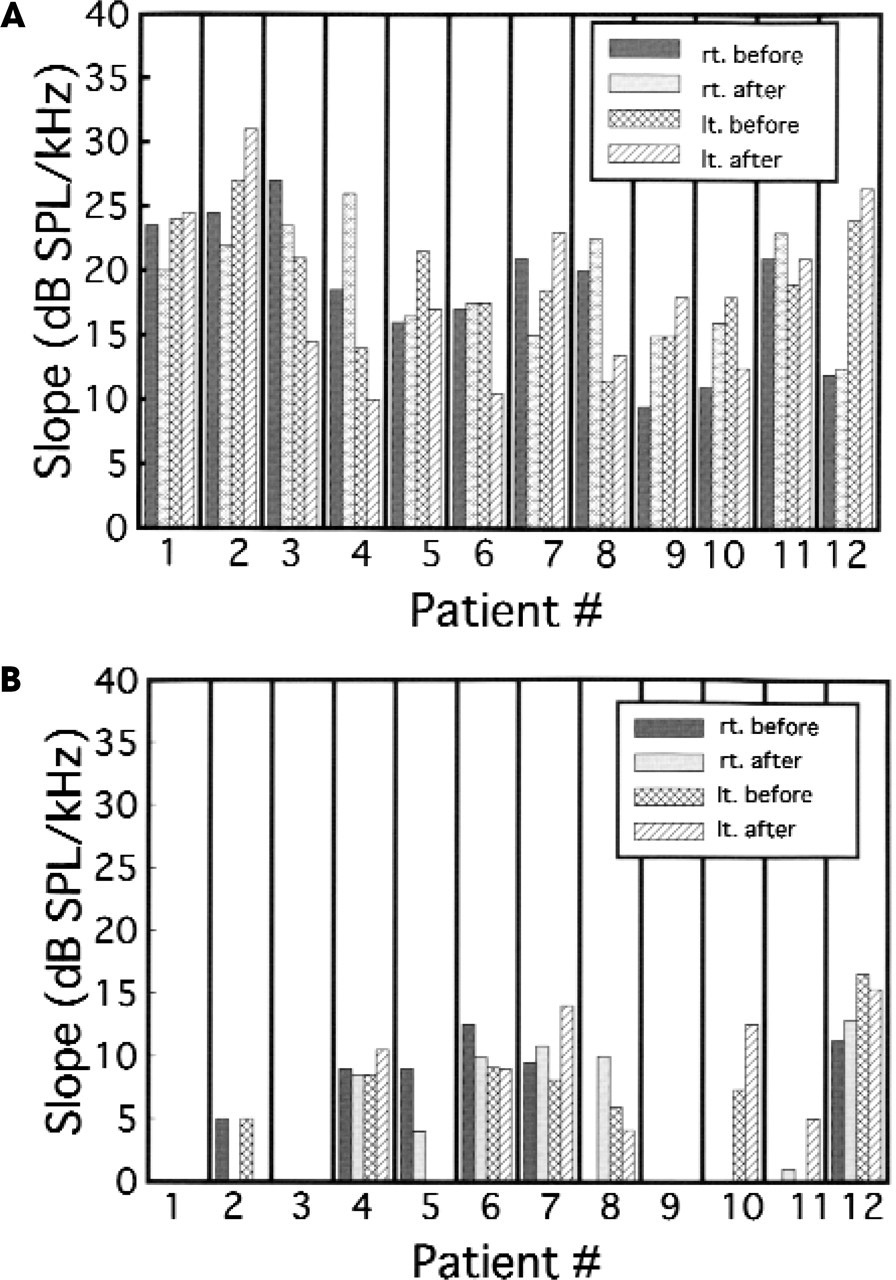
Slopes of the regression lines of the threshold at 8 to 10 kHz (
Sex, age, cisplatin dose level, and tumor diagnosis
Threshold = Slope (f-8) + Intercept (8-10 kHz)
Threshold = Slope (f-14) + Intercept (14-19 kHz)
RESULTS
After administration of cisplatin, no thresholds changed more than 20 dB at conventional audiometry frequencies and EHF, except the bilateral thresholds of patient 10 (Figs 1 and 2).
All of the patients could respond to frequencies from 8 to 10 kHz. However, because many thresholds were off the scale at the 14- to 19-kHz range, in only 5 (41%) of the 12 subjects could bilateral and 8 (67%) could unilateral regression lines be calculated before cisplatin administration for these frequencies (Figs 3 and 4).
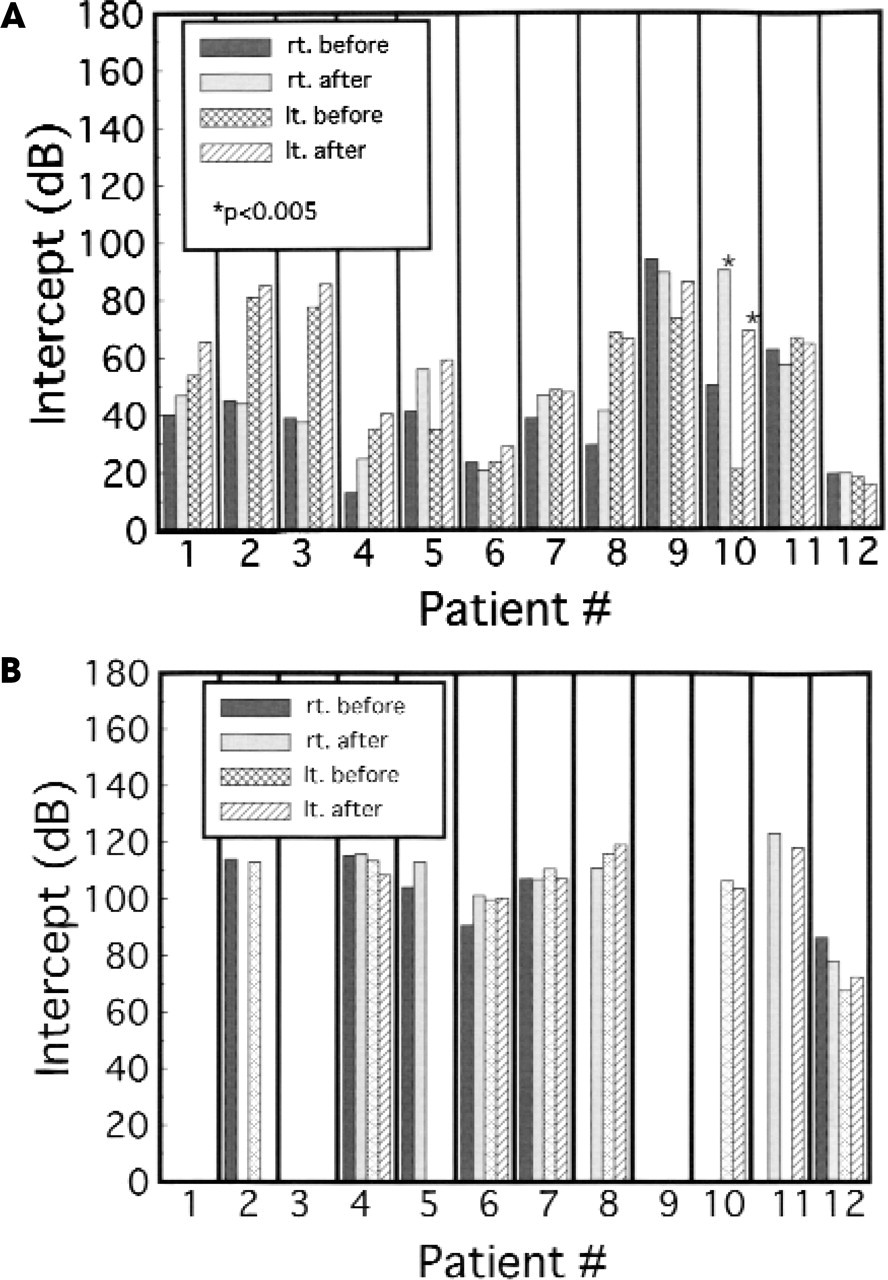
Intercepts of the regression lines of the threshold at 8 to 10 kHz (
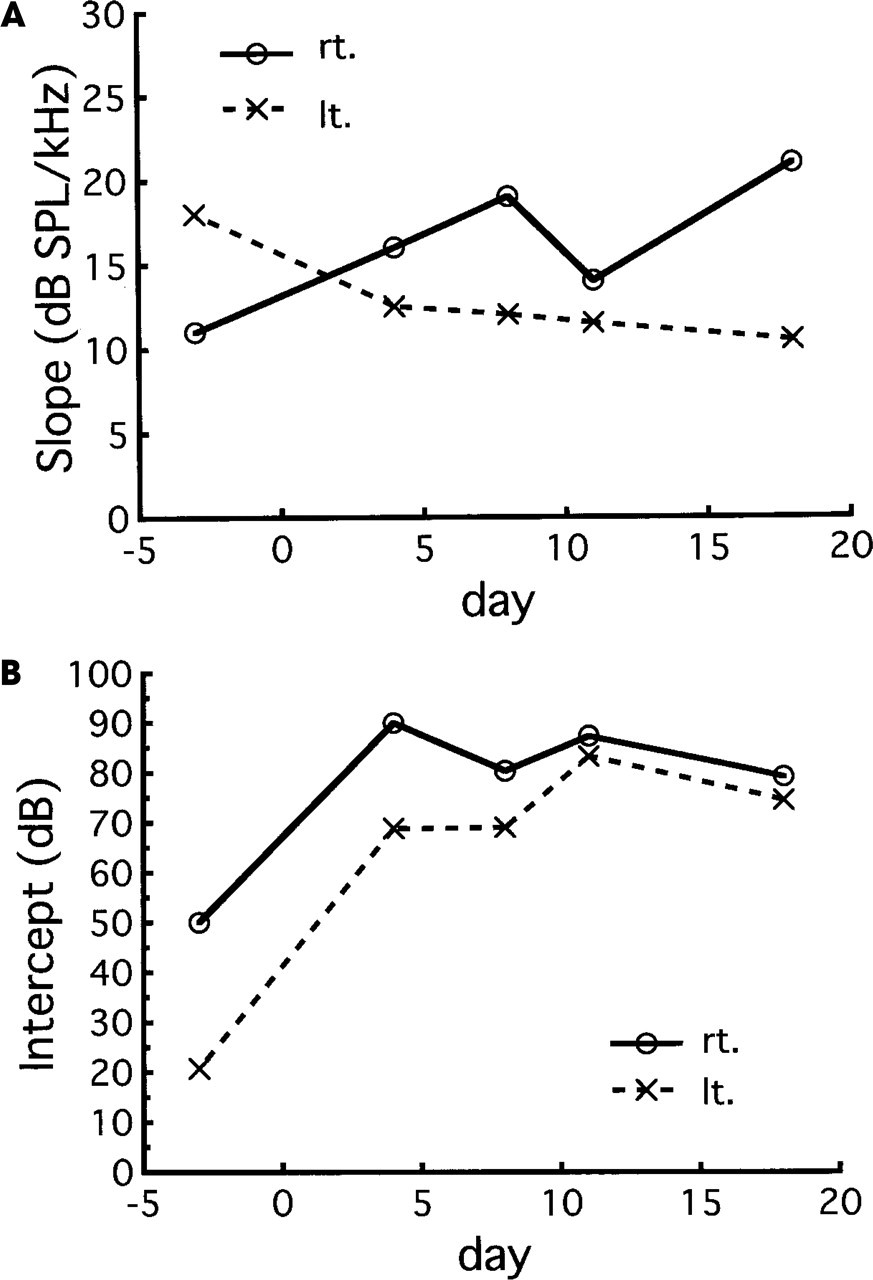
Analysis of covariance (ANCOVA) did not indicate any significant changes (P < 0.005) between the regression lines (slopes and intercepts) before and after the administration of cisplatin for all the patients, except for the bilateral intercepts from 8 to 10 kHz for patient 10 (Figs 3 and 4). Fig 2 shows the threshold changes for patient 10 at conventional audiometric frequencies and EHF before and after administration of cisplatin. The 14- to 19-kHz thresholds of this patient were off the scale for the right ear before and after the administration of cisplatin, but the threshold did not change at these frequencies in the left ear. The thresholds for patient 10 were measured 3 times during a 2-week period after the initial measurement. An ANCOVA revealed that the regression line of the threshold did not change significantly (P < 0.005) during this period (Fig 5). The interval between the first and second administration of cisplatin was 3 weeks, and the follow-up period for threshold measurement was also 3 weeks.
Vestibular function was not objectively assessed. However, there were no episodes of sudden or gradually developing vestibular symptoms in any of these patients.
DISCUSSION
Because the ages of the subjects in this study ranged high, from 39 to 63 years old (mean 54 years), some thresholds could not be measured because they were off the scale, and regression lines from 14 to 19 kHz could be calculated in only 41% bilaterally and 67% unilaterally before the administration of cisplatin.
Change of slope (
Individual threshold data could not be analyzed statistically in previous studies. A newly introduced regression-line analysis can, however, statistically analyze data for each individual. According to the analysis, a hearing loss at or above 8 kHz was faced in only 1 (patient 10) of the 12 subjects. For this patient, an ANCOVA revealed that although the intercepts increased significantly (P < 0.005), about 40 dB in the right ear and 50 dB in the left ear, the bilateral slopes did not increase from 8 to 10 kHz. Thus, the threshold increased evenly by 40 to 50 dB in the range from 8 to 10 kHz. Kopelman et al 5 also reported that there is a plateau phenomenon: an upper limit to hearing losses induced by cisplatin. According to their theory, a hearing loss of 40 to 60 dB can be expected because cisplatin selectively and progressively destroys the outer hair cells.
The energy of the acoustic waveform of this equipment must therefore include low-frequency noise at about −70 dB relative to the stimulus frequency. 9 Because the thresholds for patient 10 were 90 dB higher than those at low frequencies before administration of cisplatin, the patient might respond to that noise, and the thresholds did not change from 14 to 19 kHz.
The hearing loss of this patient did not recover during 3 weeks after the administration of cisplatin; this indicates that the damage to the hearing system was permanent.
Fausti et al 6 have reported that, if evaluation of the ototoxicity induced by cisplatin is limited to the conventional-frequency range, only 35.7% of ears showing an initial change can be detected, whereas monitoring EHFs would have enabled identification of 88.1% of ears showing an initial change. Ototoxicity of patient 10 induced by cisplatin appeared at the conventional audiometric frequency.
Strauss et al 3 have determined that the percentages of ototoxicity induced by cisplatin can range from 9% to 91%. The main features that can be culled from the literature to account for this variable occurrence of ototoxicity are differences in the technique, dosage, and duration of cisplatin administration. Bolus administration, high dosage per treatment, long-term therapy (≥6 months), and accumulated total dosage appear to be major factors accounting for greater ototoxicity. Our results showed the lowest rate (8.3%) of ototoxicity. The reasons for this could be the low dose (70 mg/m2 body surface with upper limit of 120 mg) and long-term administration (4 hours) of cisplatin and no previous chemotherapeutic treatment. Ohtani et al 10 have demonstrated in rats that the side effects, including cochlear toxicity, are reduced with the combined administration of intravenous cisplatin and fosfomycin with short-term drug administration. According to the histopathologic study, administration of fosfomycin reduces outer hair cell loss. The addition of fosfomycin administration for 6 days might be one of the causes of the low rate of ototoxicity for our subjects.