
Abstract
A retrospective study of 18 patients with malignant tumors of the external auditory canal and temporal bone was undertaken to gain an Asian perspective of this rare disease. Of these patients, 15 (83%) had squamous cell carcinoma (SCC) and 61% had stage T3 tumors at presentation. The mean age was 56 years (range 38-82 years). Seven (39%) of the 18 patients had radiation-associated tumors (RATs), and all had undergone radiotherapy for treatment of nasopharyngeal carcinoma. The 1-year cumulative recurrence for the RAT group was 100%, but there was no recurrence in the non-RAT group (P = 0.001). In malignancies of the external auditory canal and temporal bone, a different classification and staging system for patients with RATs may be warranted to better guide treatment strategies.
Reports from the West may not necessarily reflect the characteristics of an Asian population. Nasopharyngeal carcinoma (NPC) is common in the Chinese population, and radiotherapy is the usual modality of treatment for this disease. It is well known that radiation-induced malignancies may occur. The aim of this study was to gain an Asian perspective by reviewing our experience in Singapore's busiest tertiary referral hospital.
METHODS AND MATERIAL
A retrospective study of patients treated for histologically proven malignancy of the EAC and TB in the Otolaryngology Department of the Singapore General Hospital (between January 1989 and December 1997, inclusive) was undertaken. Malignancy of the auricle was excluded because the presentation, prognosis, and treatment differ greatly.
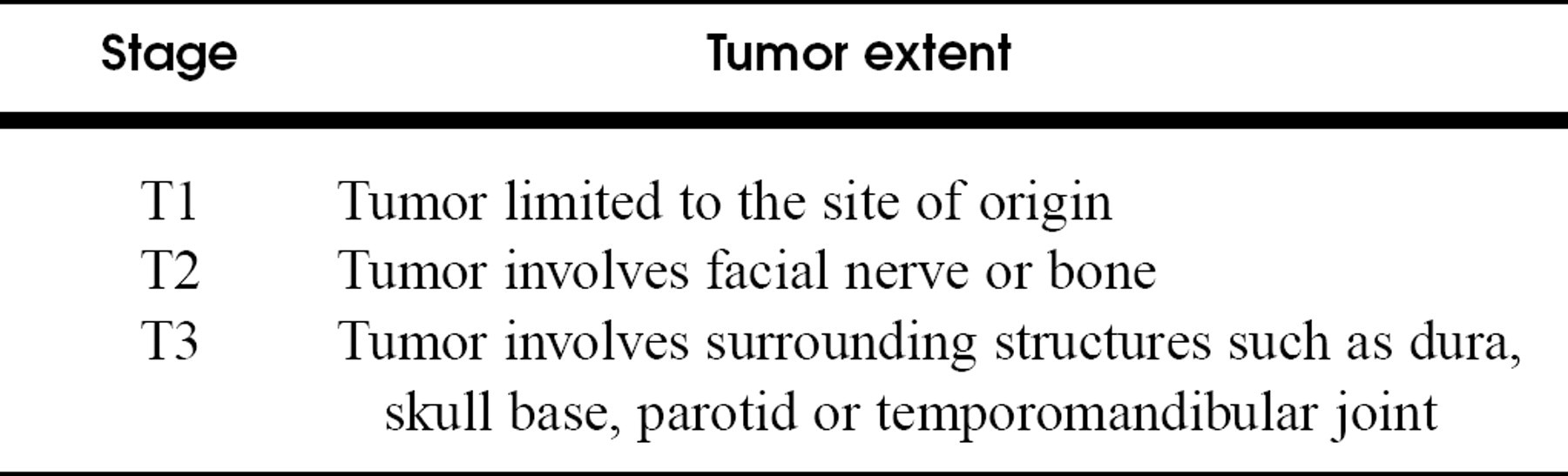
Stell and McCormick's (1987) staging system was used for the malignancy (Table 1). The malignancy is termed a radiation-associated tumor (RAT) if it satisfies the criteria of Cahan et al 1 : (1) patient has a history of radiotherapy, (2) tumor occurs in the field of radiation, (3) tumor has a histology distinct from that of the primary tumor, and (4) latency is arbitrarily taken as 5 years after radiotherapy. 1
If patients' wishes and general conditions permitted, all T1 tumors received only surgery. Radiotherapy was added for T2 and T3 tumors. Patients with T3 tumors underwent various combinations of surgery, radiotherapy, and chemotherapy.
Length of survival and disease-free interval were summarized by the Kaplan-Meier analysis, and patients with RAT versus non-RAT were compared by the log-rank test.
RESULTS
Ten patients were male, and 8 were female. Their ages averaged 56 years (range 38-82). Fourteen patients had disease limited to the EAC, 1 patient had tumor confined to the middle ear, and 3 had involvement of both the EAC and middle ear. Fifteen patients (83%) had squamous cell carcinoma (SCC). There was 1 case each of adenomatous carcinoma, osteosarcoma, and chondrosarcoma. In 7 patients, the disease satisfied the criteria for RATs. All of them had previous radiotherapy (4000-6500 cGy) for NPC.
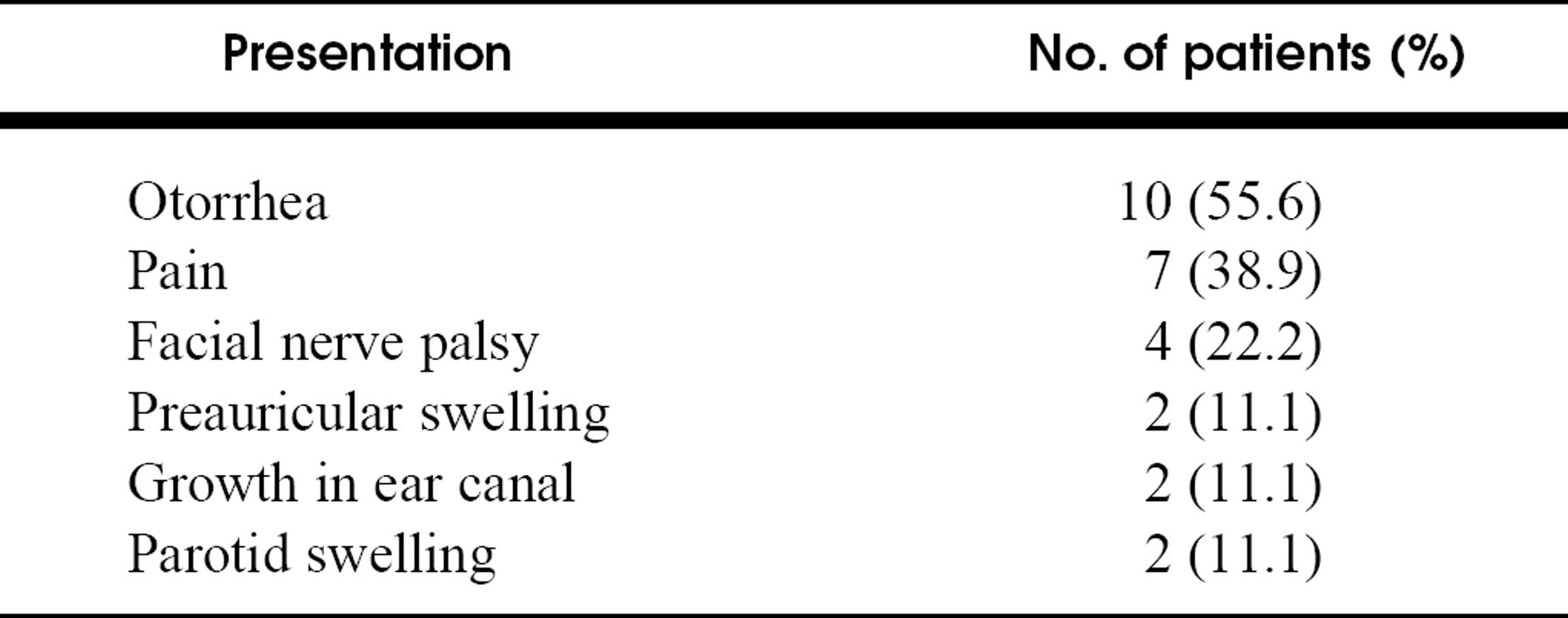
Table 2 shows the mode of presentation. Otorrhea topped the list. In 4 (22%) patients, otitis externa was initially diagnosed and treated for more than 3 months. Five patients presented to us late (more than a year after onset of symptoms), and all had advanced disease (stage 3).
The histology, management, and outcome of the 11 patients from the non-RAT group are shown in Table 3. Those for the 7 patients in the RAT group are shown in Table 4. The mean latency period before the RAT surfaced was 13 years.
Surgery was the only mode of treatment in all 5 T1 patients, and 2 had inoperable disease. Radiotherapy was given in all T2 and T3 disease. Chemotherapy was used in all 4 patients with intracranial involvement and in the 2 sarcomatous RATs. Neck dissection was performed only when lymphadenopathy was noted clinically or with CT (2 patients).
Stell and McCormick's (1987) staging system for ear malignancy
Patient presentation
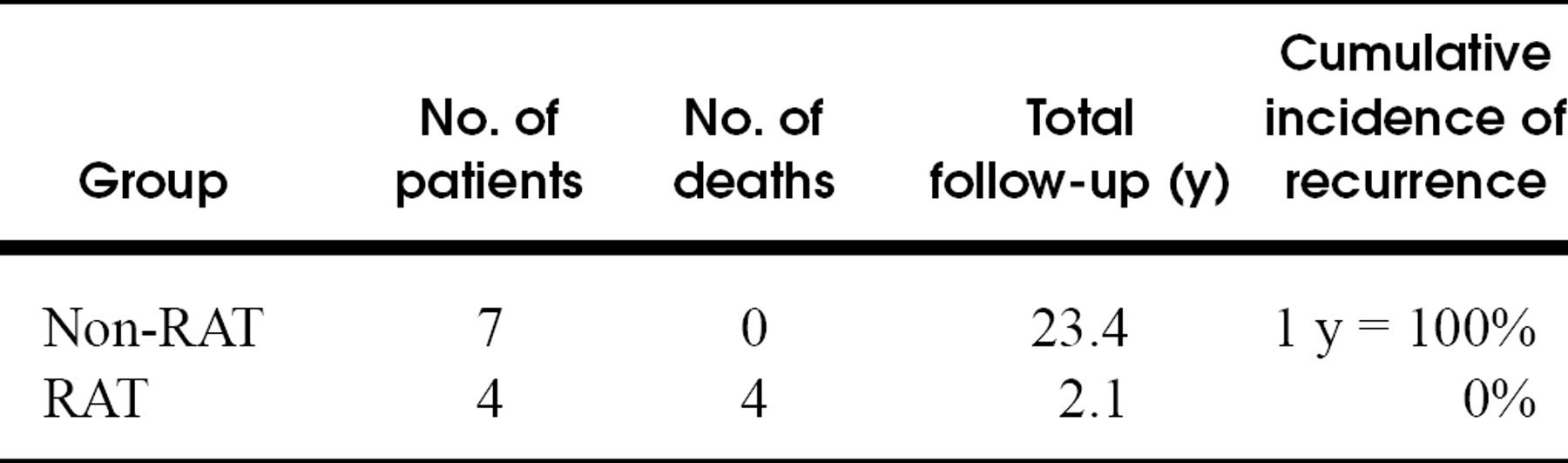
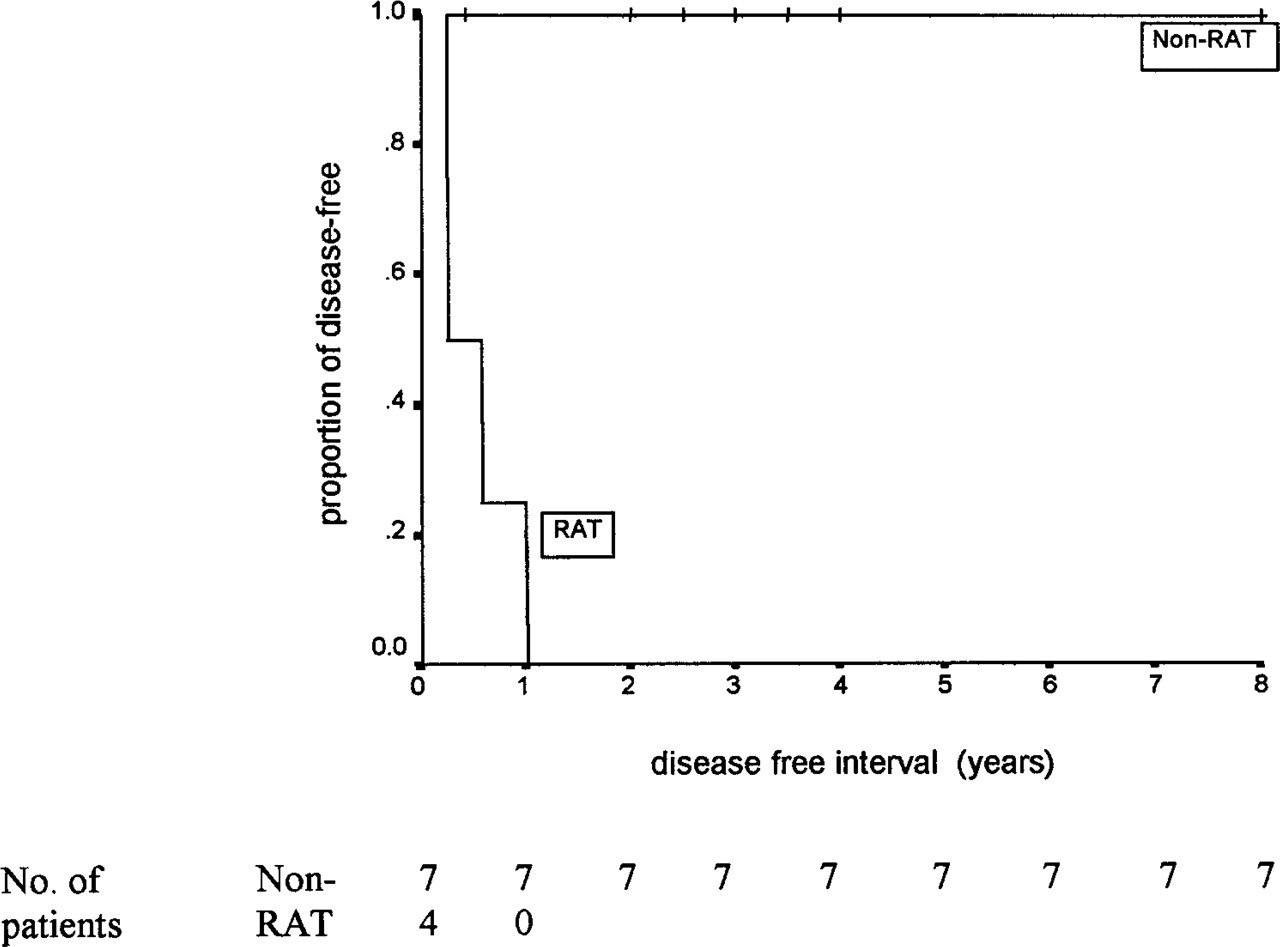
The survival difference between 18 non-RAT and RAT patients was not statistically significant (P = 0.07) with Kaplan-Meier analysis (Table 5). However, the cumulative incidence of recurrence difference between these 18 non-RAT and RAT patients was statistically significant (P = 0.001) with Kaplan-Meier analysis (Table 6 and Fig 1).
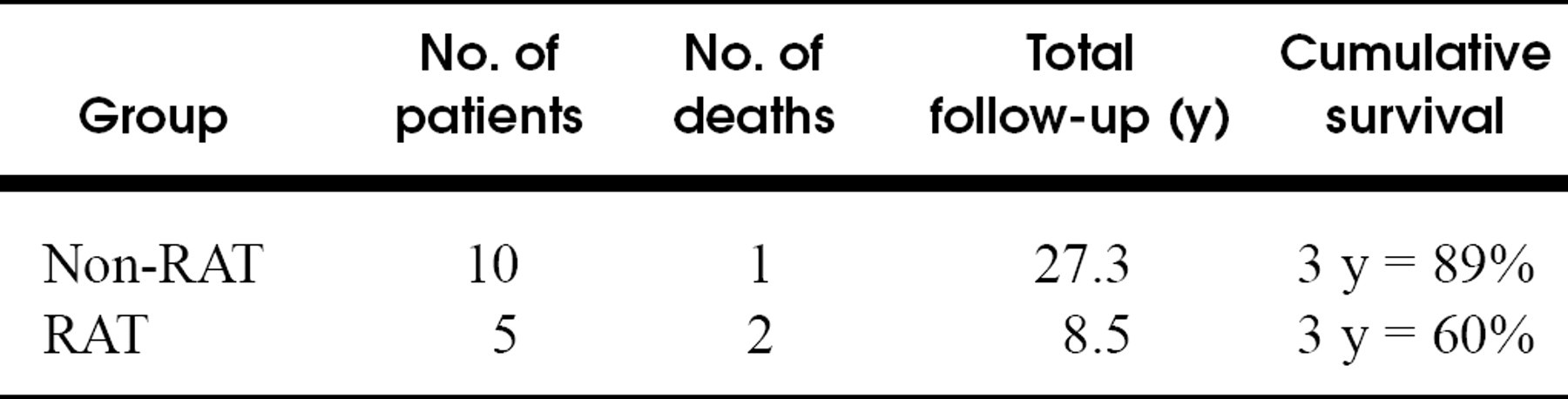
Due consideration was also given to the possibility that tumor characteristics for the 3 non-SCC patients (ie, 2 patients with sarcomas and 1 patient with adenomatous carcinoma) may have been different from those of the other 15 patients with SCC. As such, Table 7 shows the survival analysis of the 15 SCC patients separately. Again, there is no significant difference in survival between the non-RAT and RAT groups in the SCC patients (P = 0.16). Table 8 and Fig 2 show the disease-free analysis and curves of the same 15 SCC patients. Similarly, there is a significant difference in disease-free interval between the non-RAT and RAT groups for the SCC patients (P = 0.0007).
Our experience with patients shows the importance of close consultation with the histopathologist and an adequate representation of the lesion at biopsy. Patient 1 is a 50-year-old who, at presentation, had otorrhea and a mass in the EAC. Repeated transcanal punch biopsy specimens, which were taken with the patient under local anaesthesia, revealed pseudoepitheliomatous hyperplasia. The lesion failed to resolve with medication. A CT scan suggested a mastoid opacity. A transmastoid biopsy specimen was finally taken and revealed SCC. The tumor was at stage T3, but the patient is free of disease 42 months after surgery and radiotherapy.
Patients with non-radiation-associated ear malignancy
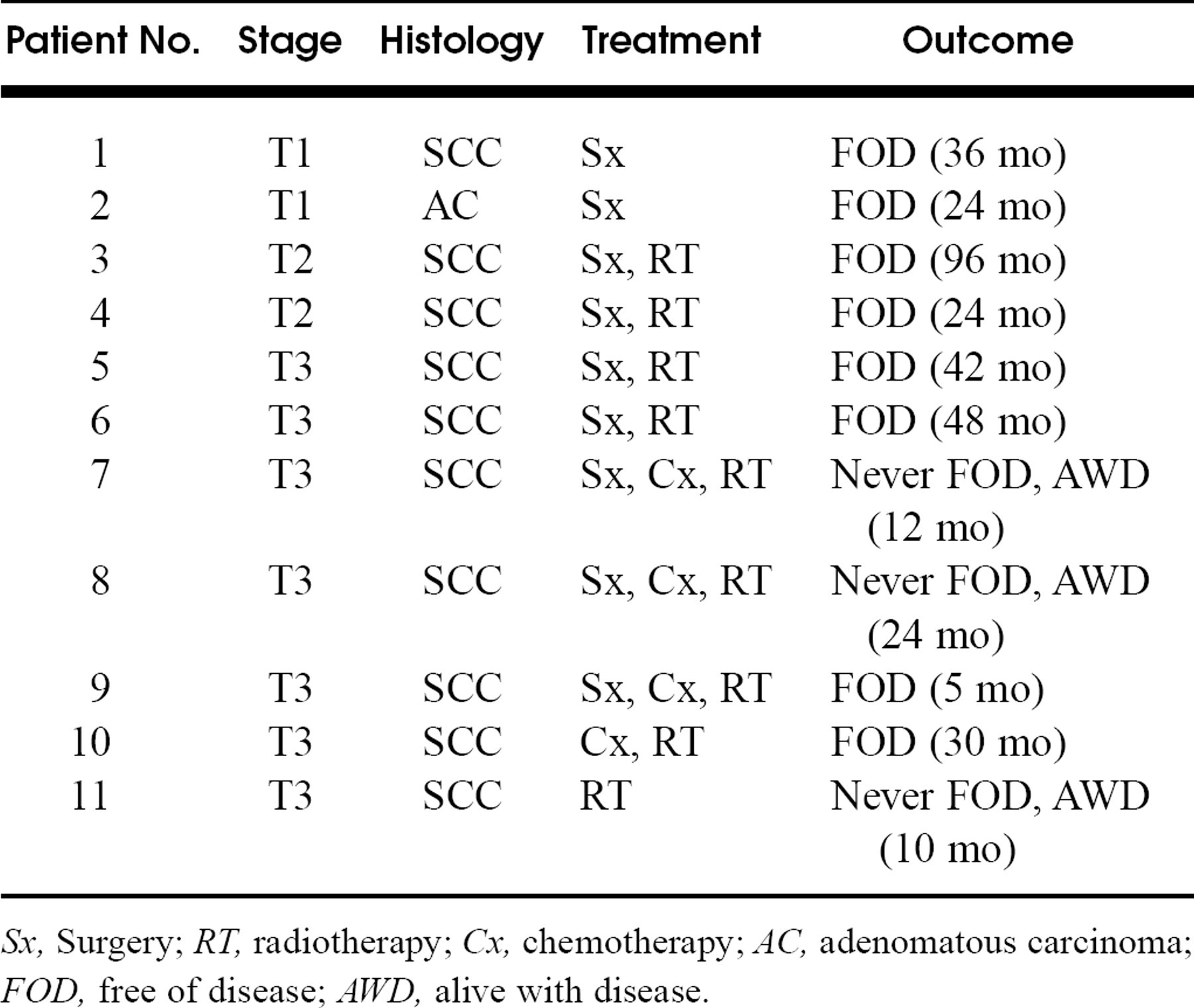
Sx, Surgery; RT, radiotherapy; Cx, chemotherapy; AC, adenomatous carcinoma; FOD, free of disease; AWD, alive with disease.
DISCUSSION
Malignancy of the EAC and temporal bone is rare. The age-adjusted incidence of malignancy of TB structures approximates only 1 per million per year in both the United States and England. 2,3 Of all malignant tumors of the ear, 60% are auricular tumors, which we have excluded from our study. 4 RATs of the head and neck are very rare, and RATs of the EAC and TB are very seldom reported. 5 This series of patients with malignancy of the EAC and TB is unique in that a significant proportion (39%) had RATs. This is largely attributed to the huge Chinese population in Singapore, which has a high incidence of NPC.
Almost two thirds of patients in the series had T3 disease at presentation. One reason could be that otorrhea, the most common presentation, was unfortunately also the least alarming. There is a tendency for the significance of this symptom to be underestimated. Four patients in this series were treated for chronic otitis externa for more than 3 months. We should be alert to the danger of chronic otorrhea masquerading as otitis externa, especially if it is blood tinged. By the time pain, facial palsy, and parotid swelling present, it is very late.
Patients with radiation-associated ear malignancy
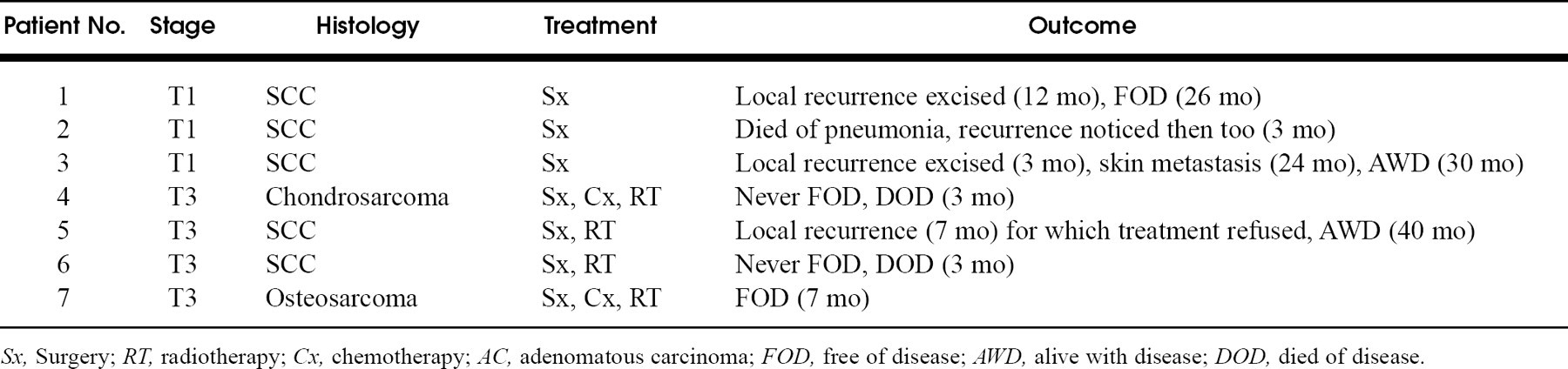
Sx, Surgery; RT, radiotherapy; Cx, chemotherapy; AC, adenomatous carcinoma; FOD, free of disease; AWD, alive with disease; DOD, died of disease.
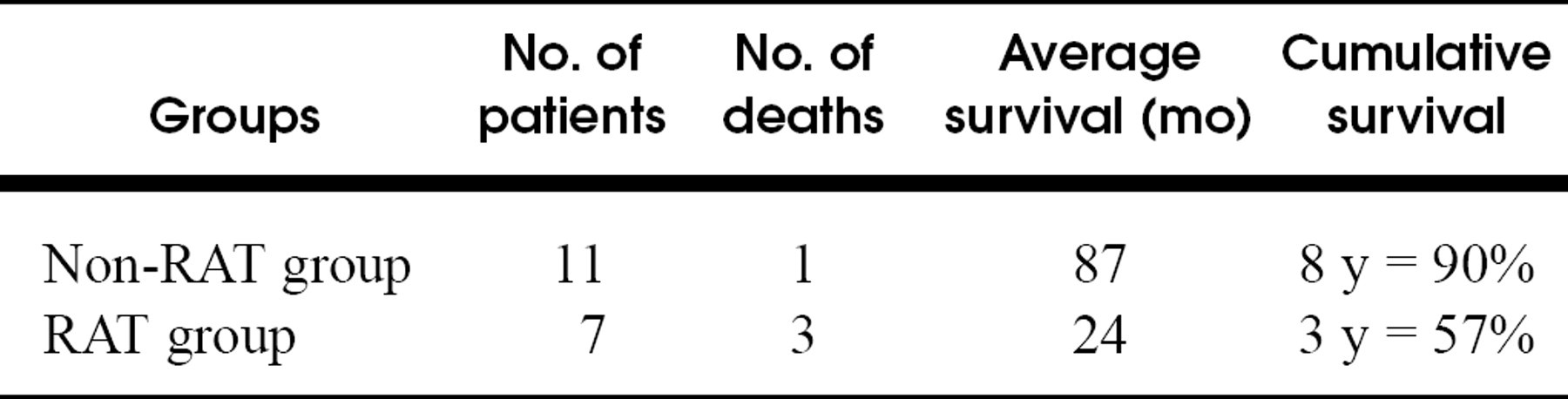
Survival in RAT and non-RAT group
Disease-free interval/recurrence in RAT group, non-RAT group, and entire study cohort

Of the 18 patients in the study, 5 were ineligible for the disease-free analysis because they had only palliative therapy or refused therapy
Survival in patients with SCC only
Disease-free interval/recurrence in patients with SCC only
Patient 1 illustrated another interesting reason for delayed diagnosis. An initial diagnosis of pseudoepitheliomatous hyperplasia was made based on small punch biopsy specimens from the external ear canal. Only larger and deeper specimens from the mastoid later on clinched the diagnosis. Misdiagnosis of SCC as pseudoepitheliomatous hyperplasia has been cautioned by Gacek et al, 6 and this case further emphasizes the importance of adequate and representative tissue biopsy specimens, as well as a close consultation with the histopathologist.
Early diagnosis of this disease is important because there is a significantly worse prognosis when tumors reach the late stages. 7-10 Prasad and Janecka 11 reviewed 96 papers and selected 26 containing information on 144 comparable patients. They noted that in advanced disease, only 2 of 144 survived more than 5 years. In this study, all 3 disease-related deaths were at stage T3, and the survival averaged only 5 months.
An interesting observation made from this study was that 5 of 7 patients with RATs had SCC, with only 2 having sarcomas. The literature so far on RATs has, to a large extent made RATs synonymous with a sarcomatous histology. 5,12-14 The reason for the predominance of SCC in the ear after irradiation to the nasopharynx is unclear. One possible explanation is that the chronic irritation caused by postradiotherapy chronic ear infections contributes to the development of SCC.
This is the first article that is able to make a comparison between patients with malignancies of the ear belonging to the RAT and non-RAT groups. A statistically significant difference (P = 0.001) was demonstrated for the disease-free interval, with the non-RAT group having a longer disease-free interval. Even after the 3 non-SCC patients are excluded from analysis, disease-free interval is still significantly different (P = 0.0007) for the 15 SCC patients with the RAT and non-RAT groups. The 3-year cumulative survival of the 18 patients in the RAT and non-RAT groups was 57% and 90%, respectively. This difference is difficult to ignore, although it is not statistically significant (P = 0.07). It may possibly be due to the relatively small number of patients studied. The impression that patients in the non-RAT group do better is consistent with the observation from other authors who estimated that for patients with RATs, 2-year survival is 22% to 32% and 5-year survival 11% to 32%, whereas for non-RAT patients, 5-year survival is 50% and 10-year survival is 30%. 5,10
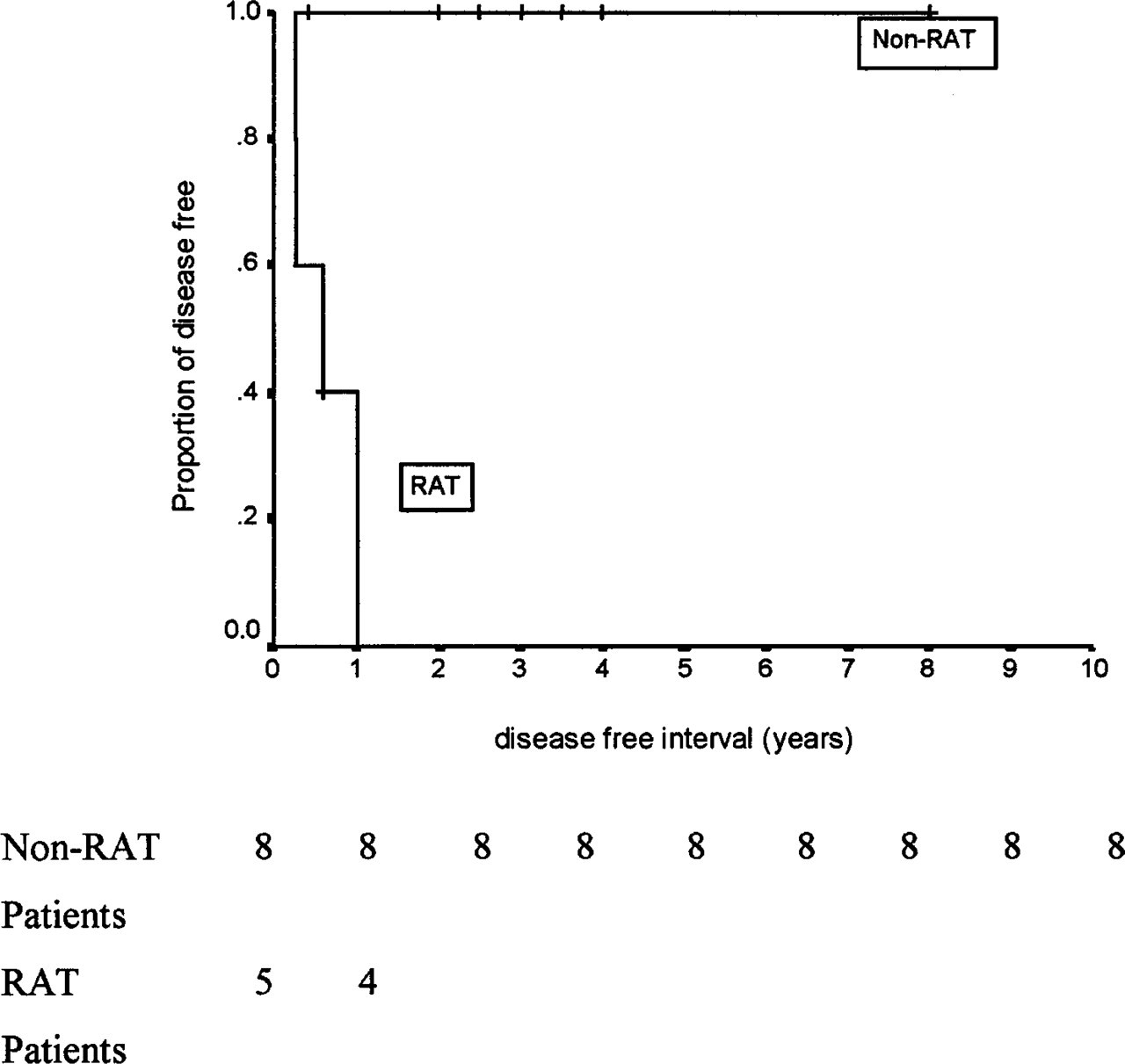
Kaplan-Meier disease-free curves for the 18 non-RAT and RAT patients.
Kaplan-Meier disease-free curves for the 15 SCC patients with RATs and non-RATs.
Possible reasons contributing to the generally poorer prognosis of patients from the RAT groups include postirradiation compromise of local immunity and difficult histologic interpretation. Furthermore, a cautious approach is usually taken in considering further radiotherapy after surgery because of the potential radiation-induced complications. More aggressive surgery would be appropriate, but surgery is often made more difficult by postradiation fibrosis.
In view of the above arguments, a case can be made for the RATs of the TB and EAC to have a different classification and staging system. On the basis of this system, treatment strategies that are different from those used in the non-RAT group may be more suitably applied. However, more studies involving larger series of patients are required before a meaningful system can be recommended.
CONCLUSION
This is the first study comparing RATs and non-RATs of the TB and EAC. Recurrence rate was significantly higher for the RAT group. Three-year cumulative survival for the RAT group was only 57%, compared with 90% for the non-RAT group. This poorer prognosis of the RAT group makes a case for consideration of a different classification and staging for the RAT group, which may better guide treatment strategies.
We thank Miss Gao Fei, MSc, from the Clinical Trials and Epidemiology Research Unit, Ministry of Health, Singapore, for help in analysis of the statistics.