
Abstract

CASE REPORT
A 22-year-old man was admitted with a soft, painless, compressible mass that had enlarged slowly since birth at the left side of the neck. He noted a marked increase in the size of the swelling during coughing and straining. There was no history of trauma or infection. Anteromedial to the left sternomastoid muscle was a soft mass, which had no pulsation with a diameter of 4 to 5 cm. Marked enlargement of the mass occurred during the Valsalva maneuver. No bruits were detectable. There was no palpable lymphadenopathy. The physical examination revealed no abnormality except for the findings in the left side of the neck. The clinical impression was that of a vascular lesion. Ultrasonographic examination of the neck revealed a 45 × 15-mm dilatation of the internal jugular vein, and Doppler study confirmed a vascular current in the mass. The contrast-enhanced computed tomography (CT) scan of the neck demonstrated fusiform dilatation of internal jugular vein and other anatomic structures as normal.
Even though the lesion caused no discomfort, psychologic distress from cosmetic deformity prompted surgical intervention. With the patient under general anesthesia in the supine position, the lesion was exposed using a left transverse cervical incision. The lesion was adherent to the sternocleidomastoid muscle and laryngotracheal cartilages. It was gently dissected, and the common carotid artery was localized posteromedially. It was confirmed that the lesion was a dilatation of the internal jugular vein. There was no arterial communication, and no mechanical obstruction was discovered during surgery. After identification of the superior and inferior ends of the dilatation, they were ligated consecutively (Fig 1). The dilated portion of the internal jugular vein was removed, and the patient made an uneventful postoperative recovery.
Macroscopically, the cystic mass was 7 × 4 × 2 cm and membranous with a thickness of 0.8 to 0.1 cm; the outer surface was covered with adipose tissue. The lumen of the cyst was smooth and grayish-yellow and had 2 narrow vascular lumens at the opposite ends. Microscopically, the lumen of the cystic mass was lined with endothelium, and irregular proliferations were revealed in the wall and the intima of the vessel. The wall of the vessel was thicker at various points, and the proliferations penetrating the surrounding mature adipose tissue were seen throughout the vessel (Fig 2).
DISCUSSION
An abnormal dilatation of a vein without tortuosity is called a phlebectasia. Although almost half of the vascular lesions of the body are localized in the head and neck region, phlebectasia involving the extrathoracic branches of the superior vena cava system is uncommon and infrequently encountered. The internal jugular vein constitutes two thirds of all head and neck phlebectasias, and the external jugular vein is the second most common site of involvement. 1
Because of its rarity, there remains controversy regarding the etiology of this phenomenon. The internal jugular vein unites with the subclavian vein to form the innominate vein behind the sternoclavicular joint; the right innominate vein lies more laterally in its course toward the superior vena cava and comes into direct contact with the right pleura. 2 Because of anatomic relationships of the internal jugular vein with the cupula of the lung and head of the clavicle, inflated cupula of the lung against the clavicle may produce obstruction and temporary distention of the vein. 3 The anatomic differences of the sides indicate why internal jugular phlebectasia more commonly occurs on the right side. 2 However, Yokomori et al 4 indicate that the venous pressures of the internal jugular vein on both the affected and the normal side are almost equal during spontaneous respiration, and this monometric study implies that there may be no obstructive process. They also demonstrated a muscle defect within the wall of the vein and congenital muscle defects in the jugular vein wall rather than constitutional mechanical obstruction in the lower neck or the mediastinum may contribute greatly to the formation of phlebectasia. 4 Mature adipose tissue in the wall of vein can have a congenital origin or be caused by degeneration of the lymphatic tissue. 5 Despite the lack of identified compression to the internal jugular vein, the existence of mature adipose tissue on the outer surface of the vein indicated that this was most likely congenital vascular malformation.
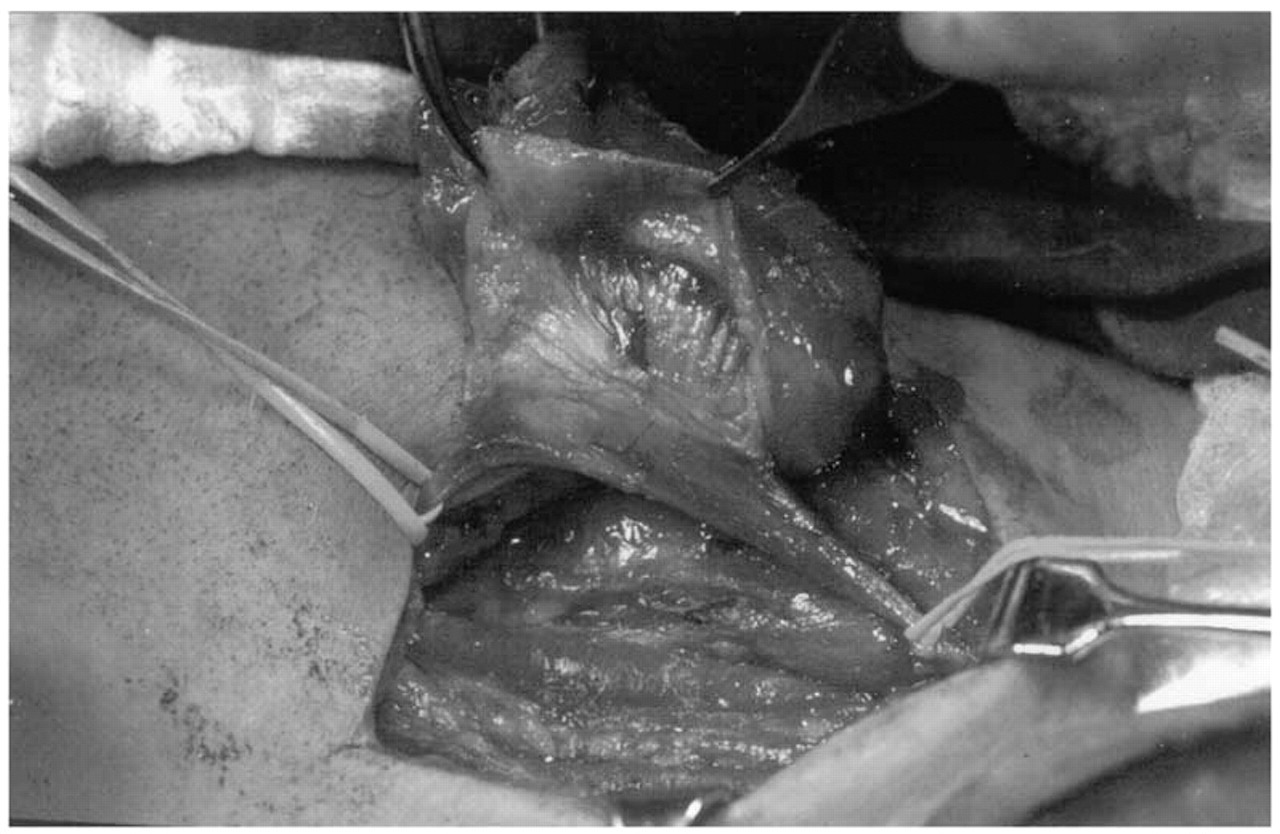
Intraoperative view of the mass covered with adipose tissue and the internal jugular vein passing through.
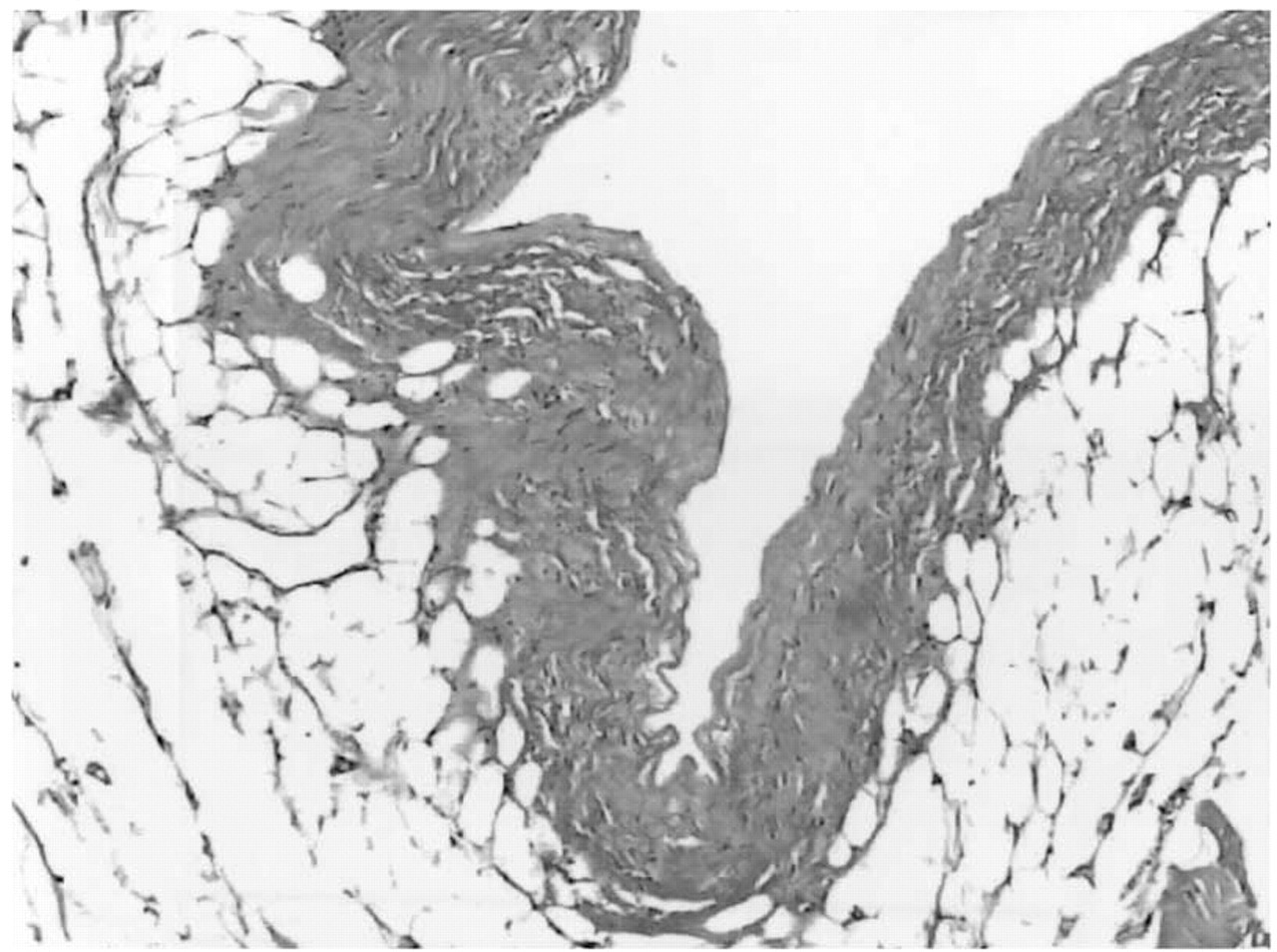
Intima and wall of the venous malformation surrounded by mature adipose tissue (hematoxylin and eosin stain; original magnification, x50).
The differential diagnosis of cystlike masses includes bronchial cysts, cavernous hemangiomas, arterial aneurysm, laryngeal diverticula, laryngocele, cervical adenitis, branchial cleft cysts, hygromas, and other cystic tumors. Although neck masses are not uncommon, the features of increasing in size during straining and Valsalva maneuver and of shrinking when the patient relaxes rule out most of the lesions. Tumors or cysts of the superior mediastinum, laryngeal diverticula, laryngocele, and venous enlargement possess this quality. The diagnosis can be made on a clinical basis and confirmed with noninvasive Doppler ultrasonographic and/or CT imaging. Neck ultrasonography is usually the primary modality in our clinic for the evaluation of neck masses. Doppler ultrasonographic shows an echo-free space that changes on Valsalva maneuver with phlebectasia. CT can also be used to confirm the dilatation of the internal jugular vein and is helpful for demonstrating any anatomic deformity and any lesion that can cause compression to the vein. Although various imaging studies can be used in differential diagnosis, invasive methods such as venography are usually unnecessary because they have been associated with complications.
Unlike venous dilatations elsewhere, phlebectasia of the extrathoracic branches of the superior vena cava system tends to be asymptomatic, and there have been no reported complications such as thromboembolism and rupture. 1,6 A swelling of neck usually causes psychologic distress for the patient or for the parents, and this cosmetic appearance constitutes an indication for the surgery.