
Abstract
BACKGROUND: Transnasal fiberoptic laryngoscopy (TFL) is frequently performed by otolaryngologists, speech language pathologists, and various other health care providers. Historically, topical sprays have been administered to patients to decongest and anesthetize the nasal mucosa, thus minimizing the discomfort of the procedure. Recently, it was reported that patients undergoing TFL with topical anesthesia experienced no improvement in comfort compared with those who received oxymetazoline or saline. This observation is in direct opposition to our clinical experience that patients tolerate the procedure better with topical anesthesia. PURPOSE: We sought to compare patient comfort levels during TFL after the administration of cocaine, oxymetazoline, or saline.
METHODS: Fifteen subjects undergoing TFL were prospectively evaluated. Each had TFL performed on 3 separate occasions. Before TFL, each patient received either 4% cocaine, 0.05% oxymetazoline, or saline topically administered via an atomizer to both nasal cavities (1 spray of 2-second duration). By the conclusion of the study, each patient had undergone TFL with each of the test agents. The subjects rated the discomfort they experienced on a scale ranging from 1 (minimal discomfort) to 5 (severe discomfort). Both patient and examiner were blinded to the test agent used.
RESULTS: The mean nasal discomfort score for saline was 2.8 ± 1.1. The scores for oxymetazoline and cocaine were 3.4 ± 0.9 and 2.0 ± 0.9, respectively. Compared with saline and oxymetazoline independently, TFL with topical cocaine appeared to provide more comfort (P < 0.05 and P < 0.005). CONCLUSION: The continued routine use of topical anesthetics such as cocaine before the performance of TFL is justified because it significantly decreases the patient's discomfort.
Since its introduction in 1968, transnasal fiberoptic laryngoscopy (TFL) has become an important tool for the otolaryngologist. The TFL is small in diameter (2 to 3 mm) and flexible and is easily passed through the nasal cavity into the aerodigestive tract, providing excellent views of the nasopharynx, pharynx, tongue base, larynx, and subglottis.
In addition to playing a role in the head and neck examination, TFL has allowed the development of several tests in which its use plays a primary role. In the flexible endoscopic evaluation of swallowing (FEES), the scope is used to visualize the mechanics and efficiency of swallowing and to detect laryngeal penetration and aspiration. 1,2 In the FEES with sensory testing (FEESST), the TFL is connected to an air pulse generator. Discreet puffs of air are directed at the larynx as a means of directly testing laryngopharyngeal sensation (LPS). 3–6 TFL can also be used in videostroboscopy and flexible tracheoscopy.
Previous studies concerning the use of topical nasal anesthesia (TNA) before TFL have concluded that its use does not improve patient comfort during examination. 7–9 At our institution, we use TNA in all patients before examination. We believe that although some patients may be able to tolerate an examination without TNA, the majority of patients undergoing TFL in this manner find the examination to be, at best, uncomfortable. Often patients are unable to complete an examination or an examination becomes marginal in quality due to patient discomfort and agitation. Therefore, we undertook the current study to evaluate the effect of TNA on patient comfort during TFL.
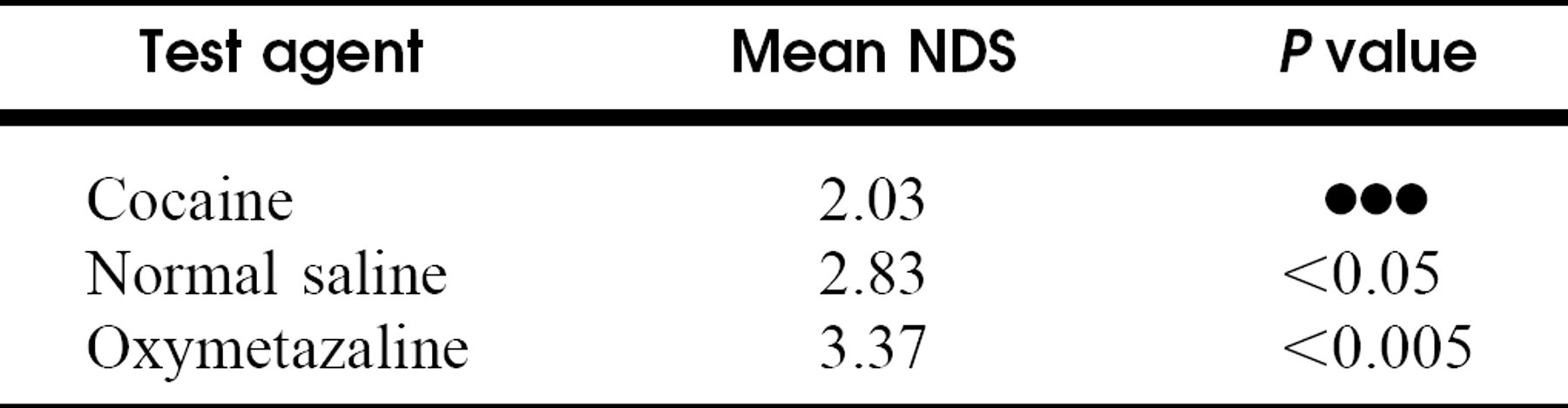
Comparison of mean nasal discomfort scores
METHODS
Fifteen asymptomatic volunteers were enrolled. The study was approved by the investigational review board of the Wake Forest University Baptist Medical Center. All patients signed an informed consent before participation in the study. Before the performance of TFL, both sides of each subject's nasal cavity were topically treated with one 2-second puff of either aerosolized 2% cocaine, 0.9% saline, or 0.05% oxymetazoline. This was done in a double-blinded fashion so that neither subject nor tester knew the identity of the test agent being administered. A standard flexible Pen-tax TFL was then passed through the nasal cavity and into the aerodigestive tract. The scope was left in place at the level of the supraglottic larynx for 60 seconds. This time period was chosen to approximate the length of an examination performed by the average otolaryngologist. Each subject underwent the testing on 3 separate occasions so that by the end of the study all subjects had undergone the procedure with each agent once. Each separate examination was performed on the same side of the nasal cavity. After each examination, the test subject was asked to assign a level of discomfort for the examination on a 5-point index scale that was used in similar studies in the past. The data for each test agent were then compared with those for the other agents using the paired t test. A value of P < 0.05 was considered significant.
RESULTS
Fifteen subjects (11 men and 4 women) were enrolled in the study. The average age of participants was 34 years. The average nasal discomfort score (NDS) for cocaine was 2.03 mm Hg. The NDSs for saline and oxymetazoline were 2.83 and 3.37, respectively (Table 1). The NDS for cocaine was found to be statistically significant compared with that for nasal saline (P < 0.05) or oxymetazoline (P < 0.005) (Table 1).
DISCUSSION
The results of our study indicate that patients undergoing TFL have less nasal discomfort when they are administered TNA before the examination. Although this finding may seem intuitive, previous studies have suggested that TNA does not increase nasal comfort during TFL.
Singh et al 7 evaluated 60 patients undergoing TFL. The patients were administered 4% cocaine to one side of the nose and saline to the other. The patients then had TFL performed on each side of the nose and rated the nasal discomfort for each on a scale of 0 to 5. The authors looked for a difference in the number of patients whose discomfort scores fell in the range of 0 to 2 versus 3 to 5 the TNA side versus the saline side. They found no statistical difference in the number of patients in each group.
Leder et al 8 evaluated 152 consecutive patients undergoing TFL. The patients were randomized into 1 of 3 groups: TNA, decongestant, and placebo. The patients ranked their discomfort on a scale of 1 to 5. Although their results demonstrated a trend toward lower discomfort scores in the TNA group, this was not statistically significant. Frosh et al 9 compared the results of 82 consecutive patients undergoing TFL. Subjects in this study were randomized to receive either TNA, saline, or nothing. A visual analog scale was used to assess the subjective experience of the examination. The results of this study demonstrated a statistically significant increase in pain and discomfort when TNA was used.
Our results contradict those of previous investigations into the effect of TNA on patient comfort (Table 1). We found that patients treated with TNA before TFL had significantly less discomfort that those given saline or oxymetazoline. The differences in our findings versus those of prior studies likely stem from differences in study design or statistical methods. In the study by Singh et al, 7 patients were assigned to 1 of 4 groups; those assigning an NDS ranging from 0 to 2 for either cocaine or saline and those assigning an NDS ranging from 3 to 5 for each test agent. Reporting a mean discomfort scale for the nasal cavities administered TNA and comparing this with the mean scores for the side administered saline would have provided a much clearer picture of any benefit of TNA in nasal discomfort. The design used by Leder et al 8 and Frosh et al 9 had each patient undergoing an examination only once and therefore subjected to only one test agent. This is in opposition to our design, in which each patient was examined on 3 separate occasions with a different agent on each examination. The use of this cross-over design makes the present study superior to the previous studies. In a cross-over study each subject serves as their own control, thus improving the reliability of the results.
Based on the results of this study, we will continue the routine use of TNA on all patients undergoing TFL in our clinics. From a subjective standpoint, we believe that patients are happier and better able to tolerate their examinations when TNA is used. Patient comfort and relaxation during TFL translate into better and more reliable examinations. We also recommend the use of TNA on patients undergoing TFL as part of an FEES or FEESST examination; we recently demonstrated that the use of TNA does not alter laryngopharyngeal sensation and thus can be used in FEES and FEESST testing. 10
CONCLUSION
The results of the current study demonstrate that patients undergoing TFL have significantly less discomfort when administered TNA before the examination. Patients will be much more likely to allow complete examinations, and results obtained in other studies such as FEES or FEESST may be more reliable when TNA is used. We recommend the use of TNA before any examination involving TFL.