
Abstract
OBJECTIVE: We conducted a pilot study to assess the effects of antigen stimulation on the appearance and function of the larynx.
STUDY DESIGN AND SUBJECTS: The prospective, double-blind, randomized study included 9 adult patients with a skin-prick test positive for Dermatophagoides pteronyssinus.
MAIN OUTCOME MEASURES: Subjects were blindly challenged via nebulizer with either an active antigenic suspension or placebo. Baseline and 30-minute evaluations of the larynx were performed. Assessments included subjective voice and video-stroboscopic assessments, acoustic analysis of voice, speech aerodynamic testing, and allergy and voice handicap questionnaires.
RESULTS: Although both inflammation and increased mucus were noted, there were no significant differences between the antigen- and placebo-exposed subjects on any of the measures obtained.
CONCLUSIONS: Our preliminary investigation was not successful in demonstrating a direct causal relationship between antigen exposure and physical or functional changes in the larynx. Future studies will involve modifications to our current methodology, including increasing the concentration of antigen, prolonging the exposure time, and observing for late phase responses.
Allergic rhinitis has been estimated to affect approximately 20% to 25% of the US population. The disorder has been well described in the literature and has been extensively characterized in terms of its pathogenesis and pathophysiology. Allergic diseases have been noted to have a significant negative impact on patient quality of life and productivity. 1
Despite the extensive literature on the nasal effects of allergy, relatively little objective information has been published on the effects of allergen exposures on the larynx. Intermittent throat clearing, cough, and dysphonia are common in patients with laryngeal inflammation. 2 Frequently, these patients are diagnosed with laryngopharyngeal reflux disease. 3 Many of these patients, however, have frequent symptoms of allergic rhinitis and note an exacerbation of their laryngeal symptoms that accompanies their nasal and sinus symptoms. 4 Jackson-Menaldi et al 5 described 17 patients in a community otolaryngology practice who had allergic disease confirmed by skin testing. All of these patients complained of concomitant laryngeal symptoms such as hoarseness and voice strain. Acoustic analyses and videostroboscopic evaluations of these patients revealed vocal fold edema as a common pathologic feature among these individuals. Although there was a concordance between the patients' symptoms and their skin test results, a causative relationship between these factors could not be determined.
The purpose of this investigation was to examine more specifically the relationship between the response to antigen stimulation among patients with allergy to a perennial allergen, Dermatophagoides pteronyssinus, and the appearance and function of the larynx. Our hypothesis was that in patients with a known history of allergy to dust mite, laryngeal exposure to D pteronyssinus would elicit a type I, IgE-mediated allergic response. We believed that this response would be noted on acoustic analyses, speech aerodynamic testing, digital audio recordings, and videostroboscopic examination.
METHODS
Design
We performed a prospective double-blind randomized study using a 2-group, pretest/post-test design in which one group was challenged with the active antigen for D pteronyssinus and the other group was exposed to a placebo suspension. Subjects underwent allergy testing for the dust mite antigen D pteronyssinus. The subjects with a positive skin-prick test were then challenged with either the active antigenic suspension or placebo via a nebulizer. Subjects completed the full testing battery before taking the challenge and 30 minutes after exposure. The test battery included subjective questionnaires for voice and sinus symptoms, acoustic voice analysis, speech aerodynamic testing, digital audiotape recordings, and videostroboscopic examination.
Subjects
Approval was obtained from the Human Investigation Committee at Wayne State University to recruit healthy, dust mite–allergic adult subjects from the patient populations of the Wayne State University/University Otolaryngology, PC otolaryngology clinics. Nine adults (6 males and 3 females) with histories of dust allergy sensitivities served as the subjects for this study. The subjects all complained of symptoms consistent with perennial allergic rhinitis exacerbated by dust exposure. Patients were advised of the study and the requirements for participation, and informed consent was obtained from all subjects before proceeding with the study. Patients were then tested for allergic sensitivity to the common dust mite D pteronyssinus. If the test was positive, the subjects were asked to continue in the full evaluative phase of the study. Because the study involved direct antigen exposure to the larynx and lower airways, extensive exclusion criteria were established. Subjects were excluded if they were under the age of 17 or over the age of 70 years, if they were pregnant (determined with a urine human chorionic gonadatropin [hCG] assessment before testing), or if they had a history of smoking within the past 2 years, current asthma, treatment with systemic corticosteroids in the prior 6 months, immunotherapy for allergy within the past 2 years, or a forced expiratory volume at 1 second (FEV1) of less than 80% of predicted value immediately before the challenge.
Allergy Testing
The presence of significant inhalant allergy to D pteronyssinus was assessed through a screening skin-prick test using the Multi-Test II device (Lincoln Diagnostics, Decatur, IL). Testing was done with 0.01 mL of a 1:20 weight-to-volume concentrate of Der P1 antigen placed into the superficial dermis. Subjects were confirmed with a diagnosis of allergy to D pteronyssinus based on a positive skin wheal response of 5 mm or greater. A positive histamine control was used to ensure normal skin reactivity, whereas a glycerin control was also used to ensure that subjects were reacting to the antigen tested and not to the glycerin preservative diluent.
Laboratory Testing Battery
All assessments occurred in the speech physiology laboratory within the Department of Otolaryngology outpatient clinical facility. The testing sequence for each subject was as follows: (1) spirometry for FEV1, (2) Voice Handicap Index (VHI) questionnaire, (3) allergy symptoms questionnaire (Sinus Symptom Questionnaire [SSQ]), (4) laryngovideostroboscopy, (5) acoustic and speech aerodynamic analyses, (6) voice sampling, and (7) antigen or placebo exposure via a nebulizer. Steps 1 through 6 were repeated at 30 minutes postexposure.
Laryngovideostroboscopy
Laryngeal anatomy and physiology were analyzed using the Kay Elemetrics stroboscopy system (model 9100 (Lincoln Park, NJ)) with 70-degree rigid endoscope (Kay model 9105). No topical anesthesia was used. Video recordings were obtained of the laryngeal inlet, vocal folds, and surrounding soft tissue boundaries during vowel (i) prolongations, repetitions, and pitch glides; repetitions of the vowel-consonant-vowel train [ihi]; and quiet and deep breathing maneuvers. An NEC PC-videotape recorder and Mitsubishi color video copy processor were interfaced for data storage, reproduction, and subsequent analyses. The following parameters were appraised for their presence, nature, and degree: (1) perilaryngeal and endolaryngeal secretions, (2) vocal fold and supraglottal erythema and edema, (3) vocal fold vibratory and general mobility characteristics, and (4) supraglottal hyperactivity. A 5-point rating scale was developed for these analyses, in which a score of 1 represented absence or normal characteristics and 5 indicated profound evidence or disturbances of the measured parameter.
Acoustic and Speech Aerodynamic Testing
The Kay Elemetrics Computerized Speech Lab (model 4300) and Aerophone (model 0592-100) systems were used to measure various acoustic (jitter, shimmer, fundamental frequency [Fo], and harmonic-to-noise [H/N ratio) and speech aerodynamic (mean transglottic airflow, glottal resistance [Rg], and subglottal pressure [Ps]) parameters. Specific examination details have been described elsewhere. 8 To measure maximum phonation time (MPT) in seconds, regardless of any underlying dysphonia, subjects were asked to take a deep breath and to prolong the vowel /a/ for as long and steady as possible. This last measure was performed 3 times with the mean value being recorded for future analyses.
Audiotape Recordings
Samples of vowel prolongations, contextual speech derived from descriptions of an action scene drawing, and oral reading of a standard paragraph (“My Grandfather”) were stored on a digital audiotape recorder (Sony model TCD-D3), using a compatible stereo condenser microphone. These recordings were obtained in the Voice Laboratory with very limited background noise. A mouth-to-microphone distance of 10 cm was held constant throughout these recordings. A 1- to 5-point equal-appearing interval scale was used to rate separately prosodic sufficiency, speech intelligibility, and possible voice disturbances such as straining, hoarseness, breathiness, and/or wet quality. At the extremes of this scale a rating of 1 represented no evidence of clinically significant difficulty with a given speech or voice feature, and 5 indicated the most deviant from normal possible.
Antigen Challenge
The active antigenic suspension was made by a technician using 1 mL of a 1:20 (wt/vol) DerP1 antigen concentrate (Antigen Laboratories, Liberty, MO) in 9 mL of 0.4% phenylated normal saline, resulting in a 1:200 (wt/vol) suspension. The placebo was made by placing 1 mL of colored 50% glycerin in normal saline into 9 mL of 0.4% phenolated normal saline. Colorization was completed through the insertion of 3 drops of yellow food color into a 50-mL vial of 50% glycerin in saline. The suspensions were then randomized and coded by a technician so that those administrating the test battery would be blind to subject group assignment. For laryngeal challenge, 0.5 mL of either the 1:200 (wt/vol) DerP1 antigenic suspension or the control was administered to the subjects using a DeVilbiss nebulizer. The subjects were instructed to breathe normally through their mouths as the suspension was nebulized. The subjects inspired the material transorally over a period of 5 minutes. Subjects were observed throughout this period for any adverse reactions. After a 30-minute period, the subjects repeated the entire testing battery.
Examiners and Judges
The examiners, who were responsible for administering the skin-prick screen, nebulizer, and test battery, were blinded to whether the subject was exposed to antigen or placebo. Three separate judges analyzed the videostroboscopy and audio-tape recordings (2 board-certified laryngologists and 1 ASHA-certified speech pathologist). The judges were blinded to the identity of the subjects and to whether the recordings were obtained before or after exposure. These individuals used the aforementioned scoring forms for their ratings. To control interjudge and intrajudge reliability, the judges were required to render ratings on 2 separate occasions. Their results for any given evaluation had to be within 1 point of each other and of the other judges' on both occasions to be included in this study.
Data Analysis
Descriptive assessments of the questionnaires, videostroboscopic evaluations, acoustic analysis, aerodynamic testing, and perceptual voice findings were performed using standard bar graphs.
RESULTS
Questionnaires
The VHI questionnaires revealed that 4 of the 9 subjects perceived voice difficulties on a frequent basis before the study. Three of these 4 individuals received the antigenic suspension. None, however, reported an acute change in the VHI after their exposure.
The sinus questionnaire demonstrated that 4 of the 9 subjects also complained of various symptoms on the morning of their study; these complaints included nasal drainage, sneezing, coughing, and throat irritation. After exposure, one of these subjects complained of worsening nasal symptoms. Another patient, who had no symptoms listed on his preexposure questionnaire, complained of throat irritation and globus sensation after receiving the antigenic suspension.
Acoustic and Speech Aerodynamic Analysis
Acoustic and aerodynamic data were collected in our speech physiology laboratory (Fig 1). Subjects who received the antigenic suspension have an asterisk next to their number in the graphs. These data do not reveal a difference between those patients receiving the antigenic suspension and the control group. Fundamental frequency, harmonic to noise ratio, jitter, and shimmer values were nearly identical for each subject's pretest and posttest. Similarly, maximum phonation time, average flow, glottal resistance, and subglottal pressure were essentially unchanged from each subject's pretest to posttest.
Digital Audio Recordings
Ratings of the digital audio recording samples obtained from each subject were performed with 100% interjudge and intrajudge reliability (Fig 2). Prosody (a), speech intelligibility (b), and “wetness” of voice (c) were judged to be normal for all subjects before and after exposure. Subjects 2 and 3 had a mild straining quality and breathiness to their voice (d and e). Neither of these patients received the antigenic suspension. Six subjects were rated to have a mildly hoarse voice before exposure (f). Four of these patients received the antigen and were not judged to be worse after their exposure.
Perhaps most notable was the amount and quality of endolaryngeal secretions present in each subject (a). Eight of the nine subjects (89%) were judged to exhibit mildly excessive secretions as a baseline. The judges rated the secretions in subject 9 worse after his exposure to the antigen.
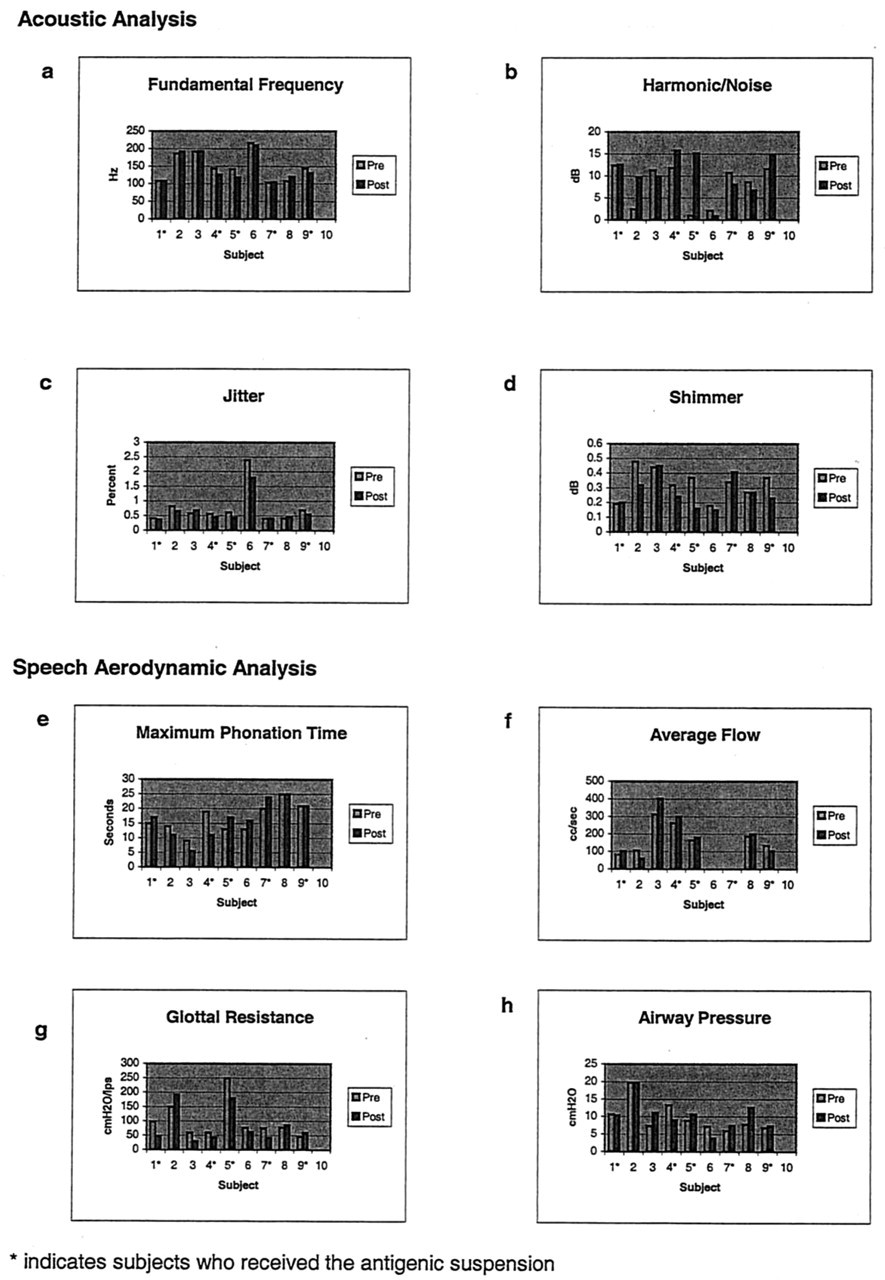
Acoustic and aerodynamic analysis of voice.
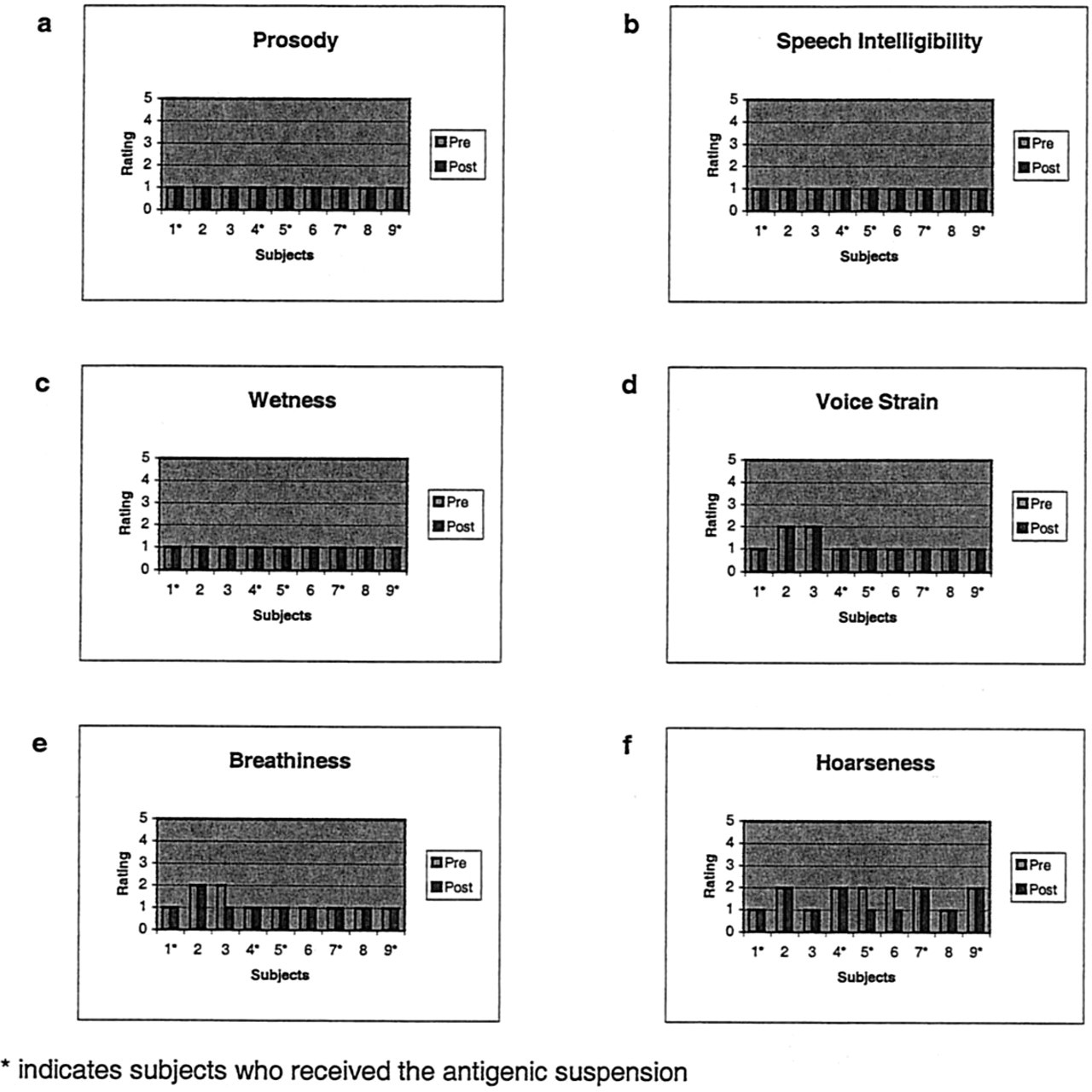
Voice perception ratings.
DISCUSSION
Allergic reactions of the larynx occur in acute and chronic forms. The first, or acute, type involves an anaphylactic reaction in which the loose areolar tissues of the larynx develop severe, rapid edema that may be life threatening if proper airway management is not promptly initiated. Its causes are well documented in the literature and are known to include a wide variety of medications, foods, chemicals, and insect venom. The chronic form of laryngeal allergy is much more controversial. Some believe that the laryngeal symptoms associated with allergic rhinitis are an extension of an allergy in the upper airway, as opposed to a distinct pathological process in the larynx itself. 9 The literature available on laryngeal allergy, however, argues against this and supports the notion that allergens affect the laryngeal mucosa directly. Williams 10 reported responses received from a questionnaire mailed to colleagues who practiced otolaryngic allergy. He reported 22 cases of “authenticated” allergic laryngitis caused by inhalants or food. Furthermore, Duncan and Duncan 11 examined 680 patients treated for respiratory allergy and found that nearly one third exhibited laryngeal signs and symptoms, including throat irritation, soreness, burning, and laryngitis. Virtually all of these individuals (94%) experienced improvements in their symptoms after allergy-specific therapy.
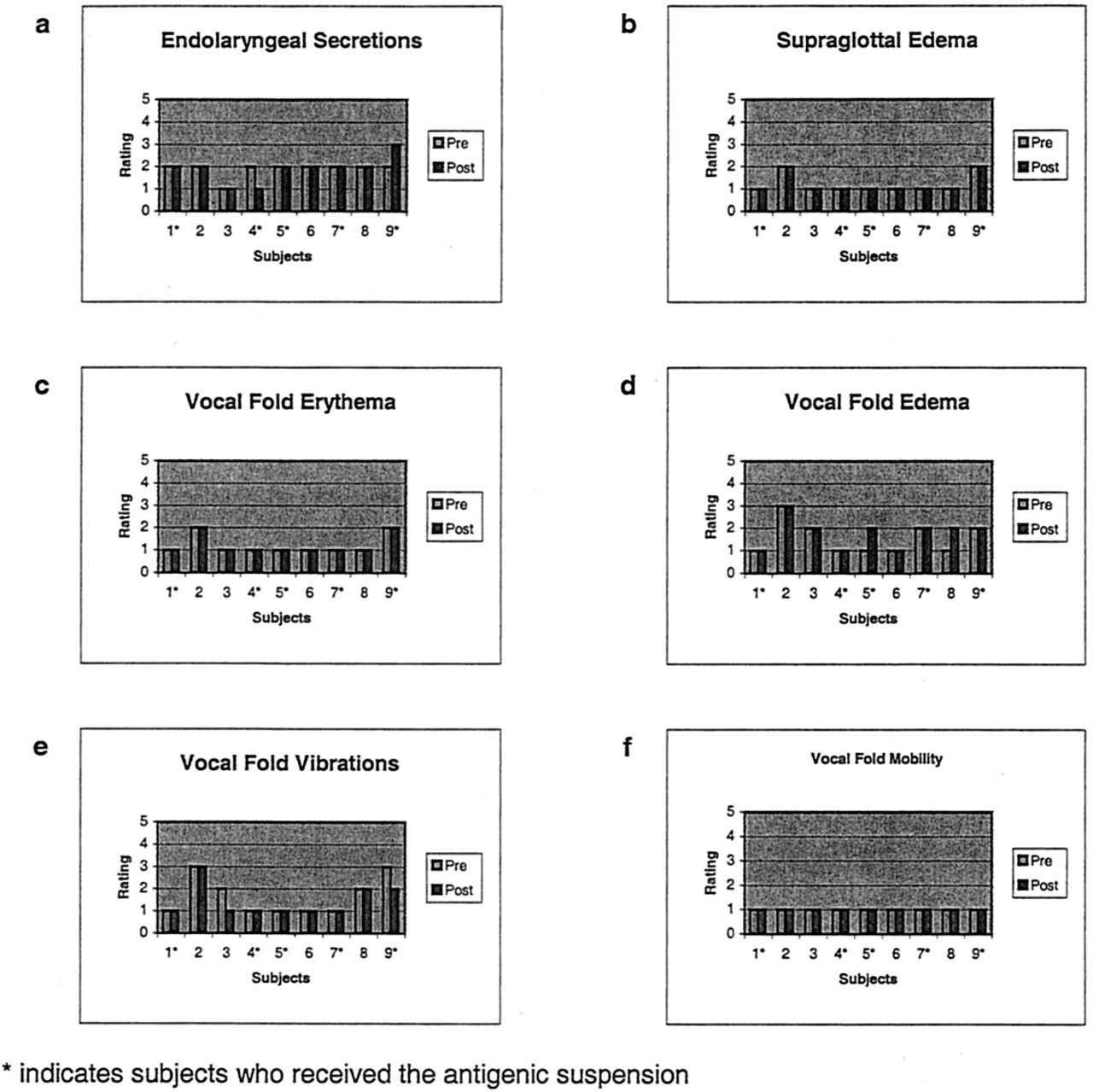
Videostrobe ratings.
In this preliminary phase of our current investigation, we were unable to demonstrate a direct relationship between exposure to dust mite antigen and changes in the appearance and function of the larynx. We predicated our hypothesis on the concept that the respiratory mucosa is contiguous throughout the nasal cavity, larynx, trachea, and bronchial tree. Although the concentration of mast cells is thought to be less in the mucosa of the larynx, 12 we believed that direct allergen exposure to the larynx would elicit a type I, IgE-mediated response similar to that seen in the nasal mucosa in patients affected with allergic rhinitis. Although the VHI revealed that 45% of our subjects with a known history of allergy had laryngeal symptoms, we were unable to document a change in these symptoms after exposure to the antigen. Similarly, our acoustic analyses, speech aerodynamic testing, and perceptual ratings of voice and videostroboscopic examinations failed to show a difference in these subjects before and after exposure to D pteronyssinus. Perhaps the amount or duration of antigen exposure was insufficient to elicit a significant change in laryngeal appearance and function.
Our preliminary data did highlight 2 interesting points. First, perceptual ratings from the digital audio recordings revealed that 66% of our patients had baseline hoarseness. Moreover, videostroboscopic examinations demonstrated a higher degree of endolaryngeal secretions compared with what would be expected in an otherwise normal population. Although we did not have a nonallergic control group with which to compare these data, these findings are in accordance with reports by Jackson-Menaldi et al 5 and Sala et al, 13 who found thick secretions, hoarseness, erythema, and edema in their patients with a known history of inhalant allergy. Unfortunately, these findings are neither specific nor significant enough to discern a direct causal relationship between antigen exposure and allergic responses in the larynx.
CONCLUSIONS
Our current pilot investigation was not successful in demonstrating a direct causal relationship between antigen exposure and physical or functional changes in the larynx, although among the allergic subjects in our study there was a considerable incidence of laryngeal inflammation. Future studies should incorporate a higher concentration of antigen, longer exposure time to the antigen, exposure to other types of antigen, and 24-hour follow-up to observe for late phase allergic responses. In addition, future research should assess the effects of antigen challenge on allergic patients with a significant history of chronic laryngitis.