
Abstract
OBJECTIVE: We sought to estimate the prevalence and severity of tinnitus in patients with chronic pain.
STUDY DESIGN AND SETTING: We conducted a prospective nonrandomized study in which a survey and the Tinnitus Handicap Inventory (THI) were distributed at a tertiary chronic pain clinic.
RESULTS: Seventy-two patients participated. 50 women (mean age, 53 years) and 22 men (mean age, 47.5 years); 54.2% reported having tinnitus. There was an even distribution of patients reporting the onset of tinnitus as before versus after the onset of pain. Four patients reported a direct association between tinnitus and pain. The mean THI score was 27 (of 100) (n = 35). Fifteen subjects scored less than 16, indicating no handicap, and 4 scored over 58, indicating a severe handicap.
CONCLUSION: The study results suggest a high incidence of tinnitus within this population. There were few strong associations between pain and tinnitus. Tinnitus does not significantly handicap the majority of these patients.
SIGNIFICANCE: Tinnitus is a common symptom in the chronic pain population but is not a significant problem for these patients.
Similarities also exist between patients with chronic tinnitus and patients with chronic pain. Chronic pain patients have been subjected to numerous psychologic profiles. They are known to have hypochondriasis, obsessive-compulsive behaviors, increased tendency to self-focus, perceived lack of control over symptoms and life events, maladaptive coping strategies, and other conditions. Folmer et al 5 recently compared these characteristics with those of patients with tinnitus and found that “tinnitus” and “pain” could often be substituted when describing these patients. Both groups are caught in a vicious circle whereby their symptoms lead to increased depression, fatigue, and anxiety, which in turn exacerbate their symptoms.
In addition, both of these disorders are difficult to treat, requiring a series of individualized treatment trials. Once first-line therapies for each disorder are exhausted, patients may be offered anti-depressants, biofeedback, electrical stimulation, or acupuncture.
Similarities in neurobiological models, patient psychologic profiles, and treatment options warrant greater attention. We distributed a 2-part survey to new patients evaluated in a chronic pain clinic to investigate these similarities. We wanted to know how many of these patients have tinnitus, whether tinnitus related to pain in onset or severity, and whether any of the treatments received for chronic pain affect tinnitus.
METHODS
Approval for the project was granted by the institutional review board. A 2-page survey was distributed to nonrandomized new patients evaluated at a tertiary care pain clinic over a 6-month period. Demographic data as well as information regarding otologic health were obtained. Participants who denied having tinnitus did not proceed further; participants who reported having tinnitus were asked to continue. The remaining questions on the first page attempted to qualify tinnitus, identify tinnitus risk factors, and identify associations between tinnitus and pain. An abbreviated version of the first page appears in the Appendix. The second page of the survey was the previously validated Tinnitus Handicap Inventory (THI). 6 The purpose of the THI was to objectively quantify the severity of the tinnitus and its impact on patients' lives.
Patients were met at the check-in counter of the clinic and asked to participate. The survey was then explained, and written informed consent was obtained. The explanation of the survey included a brief scripted definition of tinnitus to ensure that every patient had the same understanding of tinnitus. The surveys were completed and collected immediately before the clinic visit.
Data were then entered into a computerized database (Microsoft Excel for Office 2000; Microsoft, Redman, WA), and statistical calculations were carried out with a statistical software package (Minitab Version 13: Minitab Corp, State College, PA).
RESULTS
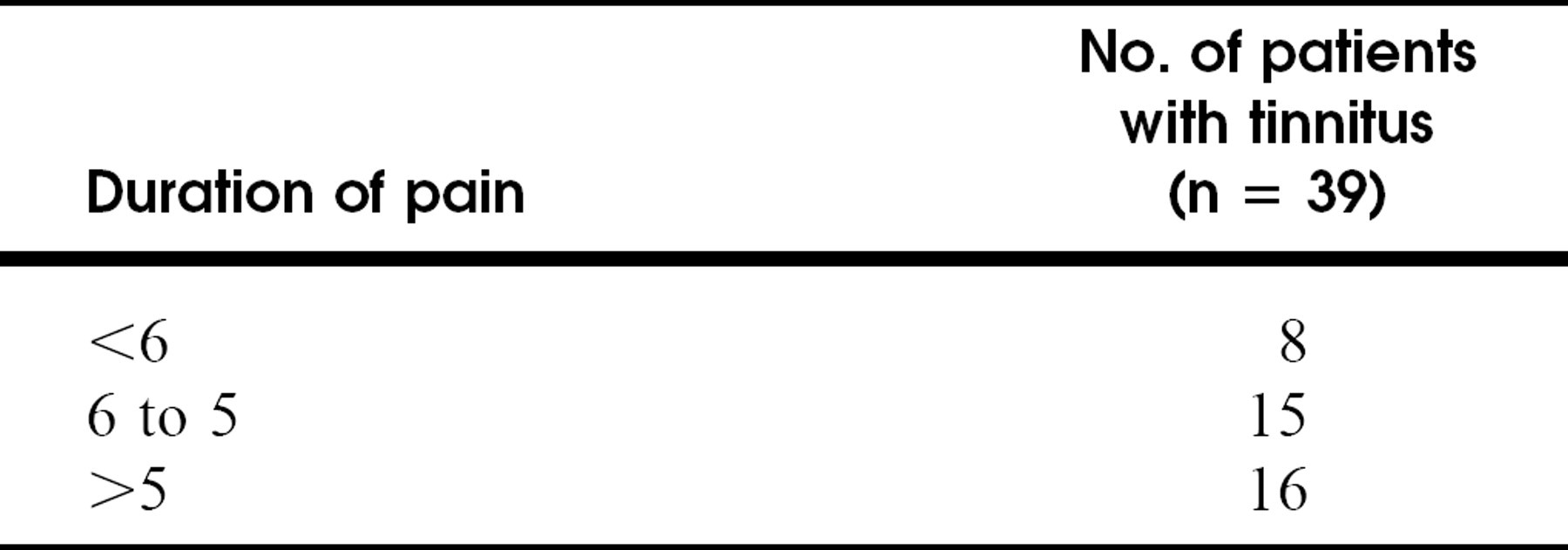
A total of 72 patients were asked to fill out the survey, and all agreed to participate. Not all patients answered all questions, and this is reflected by changes in n values. Fifty were women (average age, 53 years; age range, 16 to 88 years) and 22 were men (average age, 47.5 years; age range, 24 to 81 years). Duration of pain was most commonly recorded as greater than 5 years (16 of 39, or 41%). The distribution of pain sites was roughly equivalent for men and women.
Thirty-nine subjects (n = 72, or 54.2%) reported having tinnitus; 29 were women (average age, 52.8 years; age range, 16 to 88 years) and 10 were men (average, 44.3 years; age range, 24 to 67 years). Duration of pain in this group was most commonly recorded as between 6 months and 5 years. “Back” was most frequently reported as the primary site of pain (n = 39, or 53.9%) (Fig 1).
The average pitch of tinnitus was graded as 6.1 on a 10-point scale where a lower score indicates a lower pitch. The average volume of tinnitus was graded as 4.9 on a 10-point scale where a lower score indicates a lower volume.
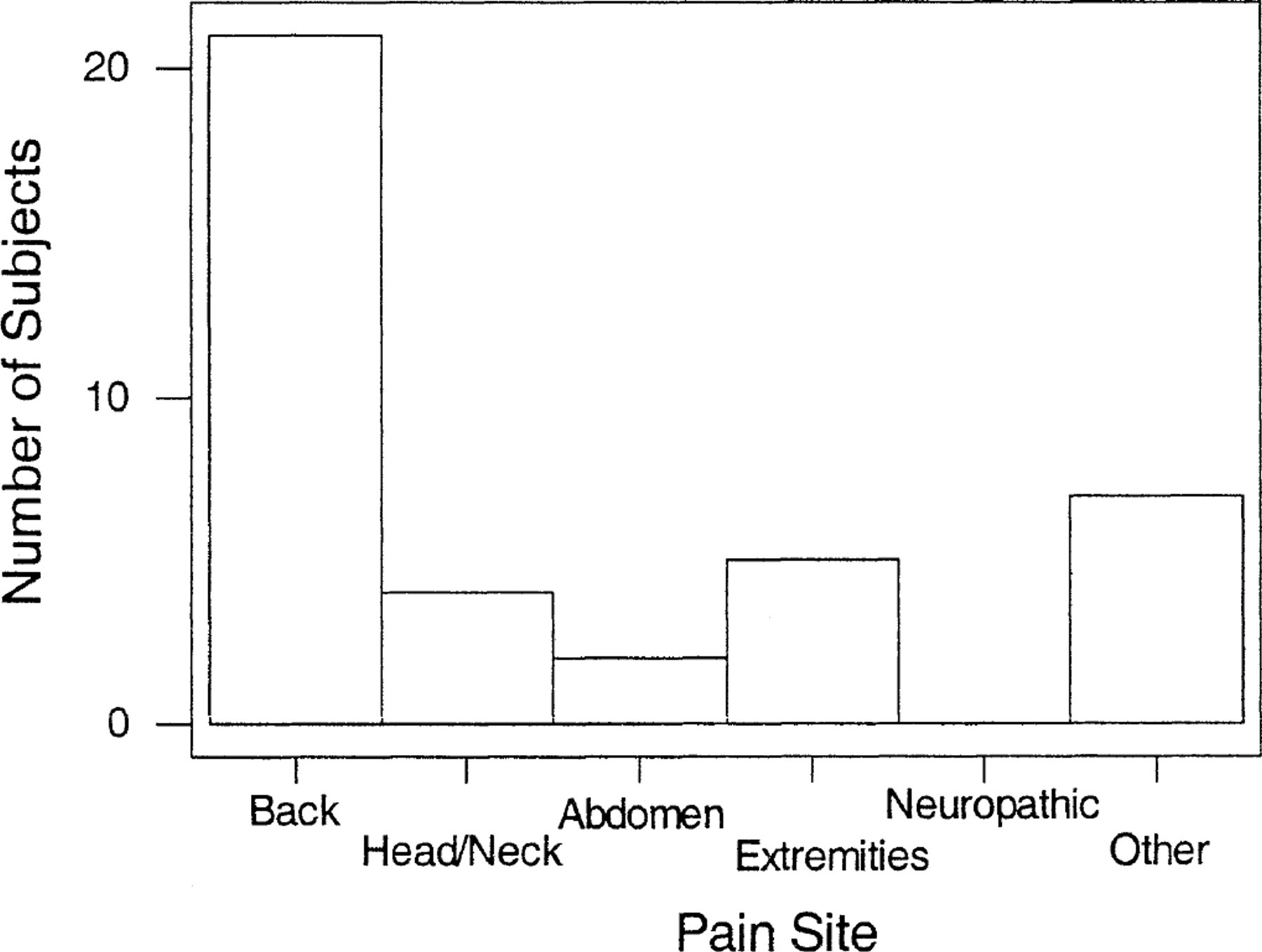
Site of pain reported by patients with tinnitus.
Eighteen subjects reported a previous subjective hearing loss (n = 37, or 48.7%). Fifteen subjects reported a previous history of noise exposure (n = 36, or 41.7%). Only 4 subjects had a history of previous head injury (n = 36, or 11.1%). Twenty-six subjects drank caffeinated beverages daily (n = 36, or 72%) with a range of 1 to 8 cups, with 1 subject admitting to drinking 31 cups of coffee per day. Twenty-two subjects drank 2 or more cups per day (n = 36, or 61%). Nine subjects reported using aspirin or aspirin-containing products regularly (n = 34, or 26.5%).
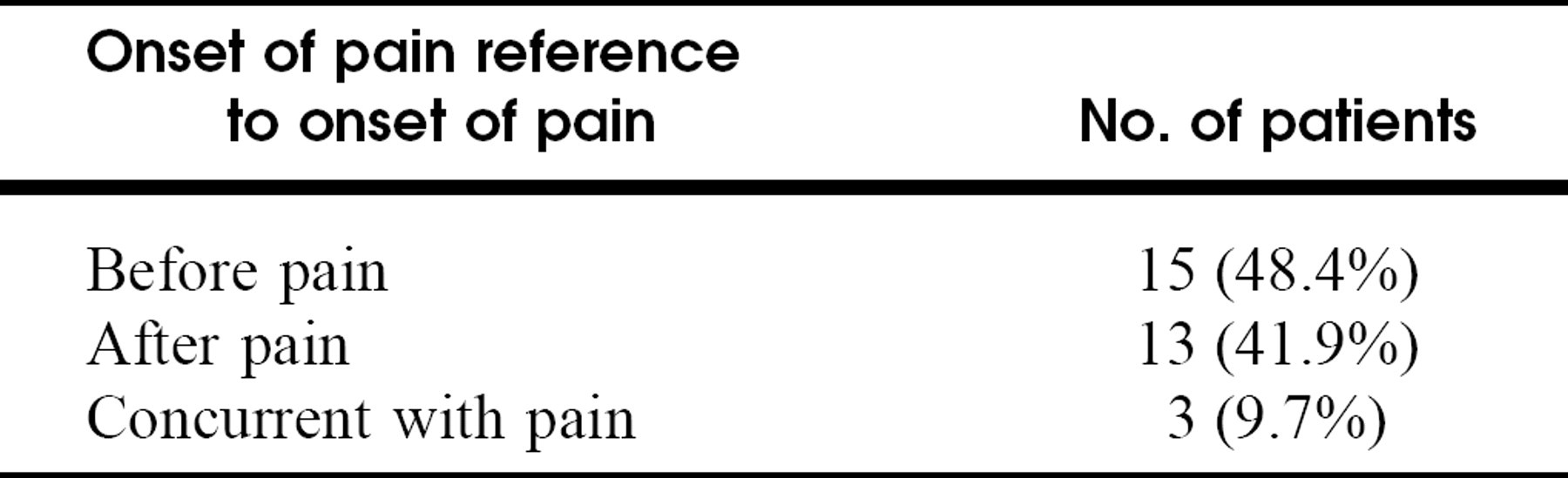
The average duration of tinnitus was 13 years (Table 1). Fifteen subjects reported the onset of tinnitus before the onset of pain (n = 31, or 48.4%), 13 subjects reported the onset of tinnitus after the onset of pain (n = 31, or 41.9%), and only 3 (n = 31, or 9.7%) reported that the 2 began concurrently (Table 2). Four subjects reported an association between tinnitus and pain (n = 31, or 12.9%). Eight subjects (n = 27, or 9.6%) reported that a specific pain treatment improved their tinnitus (Table 3).
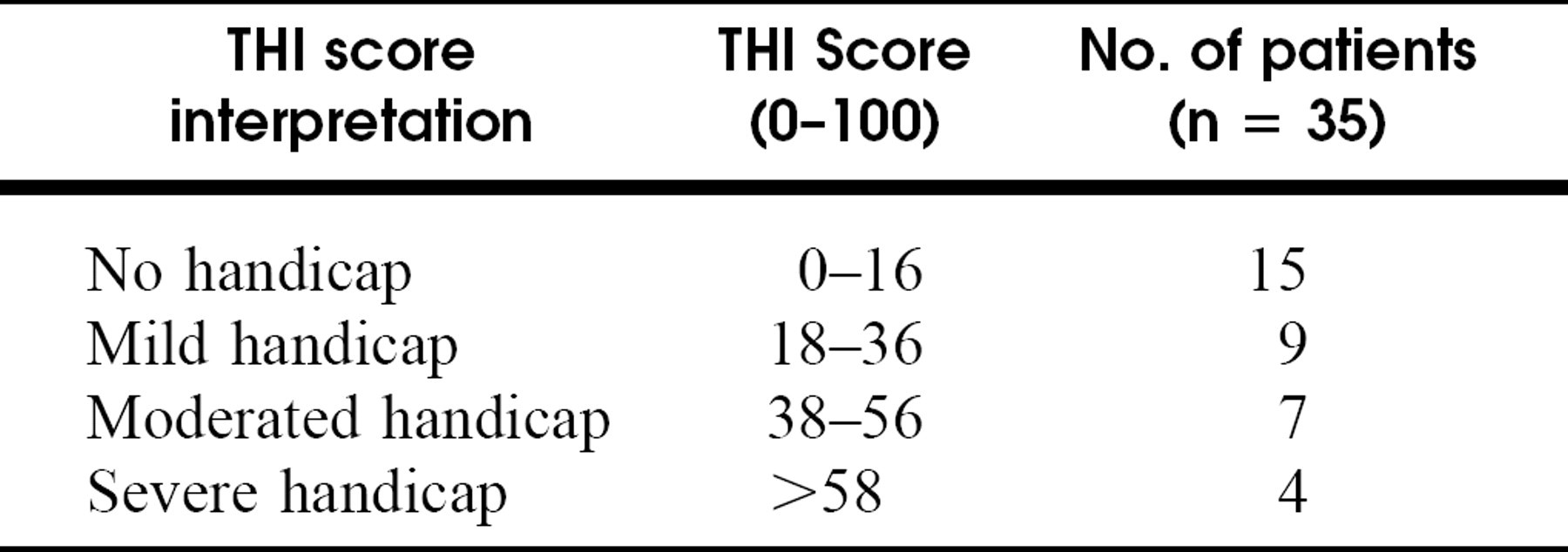
Scores on the THI were as follows (Table 4). The mean THI score was 27 (of a possible 100) (n = 35; range, 0 to 96), indicating only a mild handicap for the group as a whole. No handicap (score, 0 to 16) was demonstrated in 15 (42.9%), mild handicap (score, 18 to 36) was demonstrated in 9 (25.7%), moderate handicap (score, 38 to 56) was demonstrated in 7 (20%), and severe handicap (score, >58) was demonstrated in 4 (11.4%) patients. An analysis of variance failed to find any significant relationship between handicap from tinnitus and duration of pain, site of pain, or duration of tinnitus.
Duration of pain
Onset of tinnitus in reference to onset of pain
Treatments that improved tinnitus
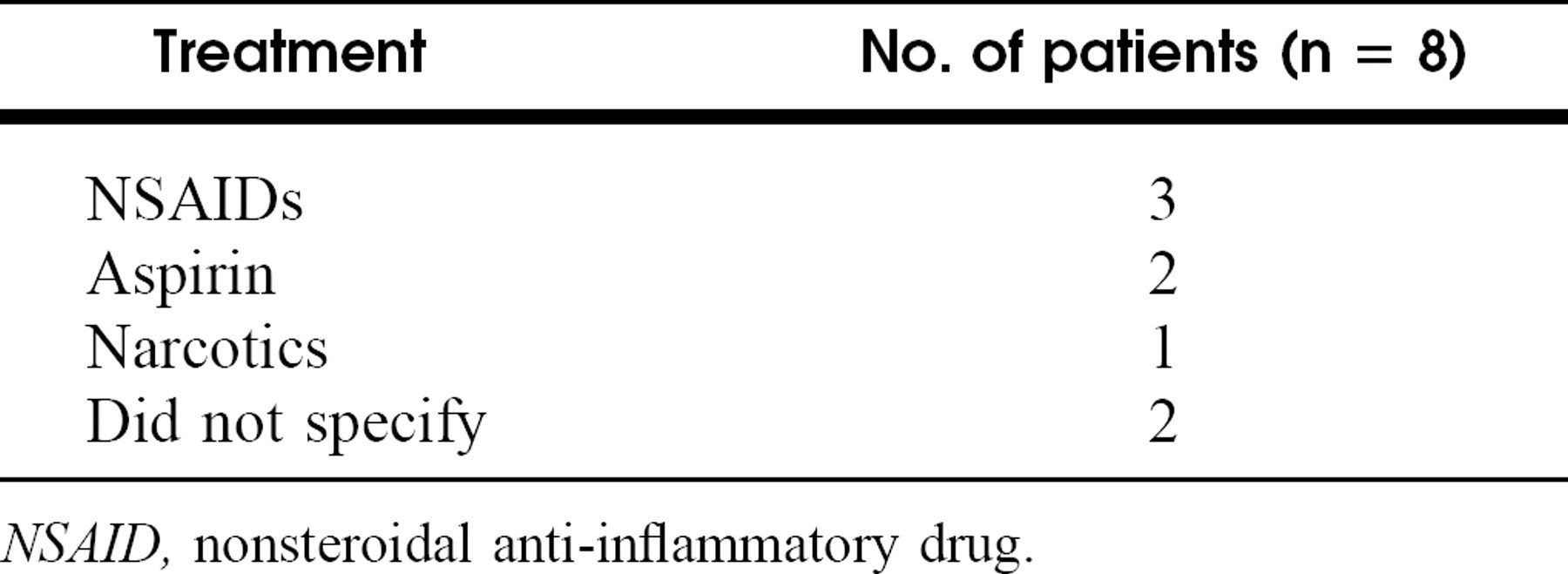
NSAID, nonsteroidal anti-inflammatory drug.
Results of the Tinnitus Handicap Inventory (THI)
DISCUSSION
Much has been written regarding the similarities between tinnitus and pain and the similarities between the patients who have these symptoms. von Bekesy 7 initially described similarities between perception of sound and skin sensations in 1957. In 1987, Tonndorf 8 theorized that tinnitus production was similar to pain production by equating inner and outer hair cell function to that of large and small diameter afferent nerve fibers described in the “gate control theory of pain.” Others have also weighed in on the analogy between tinnitus and pain. 2–4
Most recently, Folmer et al 5 reviewed survey data from their tinnitus patients, looking for similarities between their patients and pain patients. They summarized the similarities between tinnitus and pain, pointing out that both are continuous but fluctuating subjective sensations, may be masked, are controlled by the central nervous system, and are treated peripherally with limited success. They also stated that both symptoms are accompanied by a significant amount of psychologic overlay and that multimodal treatment often is indicated. They used the existing pain management literature as their comparator group.
The personalities of patients with chronic pain and patients with tinnitus have been scrutinized. Chronic pain patients are noted to have elevations in hypochondriasis, depression, and hysteria when evaluated by the Minnesota Mulitphasic Personality Inventory. 9,10 They also have obsessive-compulsive tendencies, high degrees of self-focus, perceived lack of control over life events, and maladaptive coping strategies. 5 Personality disorders are present in 31% to 59% of pain patients compared with 0.5% to 3% of the general population. 11
Tinnitus patients have been studied with the use of the Minnesota Mulitphasic Personality Inventory as well. Meric et al 12 evaluated a large group of French patients with tinnitus in 1998. They found that although their patients did not differ significantly from the general population, patients with severe tinnitus did differ significantly. These patients had a greater tendency to have depression, paranoia, hypochondriasis, and anxiety. They found depression to have the strongest association with severe tinnitus. This is similar to the findings in pain patients.
Newman et al 13 also looked at the psychologic make-up of tinnitus patients. They found that patients with increased self-focused attention showed significantly greater perceived tinnitus handicap, distress from tinnitus, and depression.
All of the above-mentioned similarities prompted us to examine a chronic pain population. Although tinnitus is estimated to afflict between 16% and 35% of the general population of the United States, 4,14 53.9% of our subjects reported tinnitus. The high prevalence may be due to the psychologic overlap between groups of patients with tinnitus and patients with pain. The average duration of tinnitus appeared long (13 years), but the number of subjects reporting the pain began before the tinnitus was roughly the same as that reporting the pain began after the tinnitus. Only 4 subjects felt that their tinnitus was related in any way to their pain, and only 8 subjects reported that their tinnitus improved when their pain was successfully treated. Interestingly, the treatments that improved their tinnitus are traditionally thought to worsen tinnitus (ie, aspirin and nonsteroidal antiinflammatory drugs).
Furthermore, tinnitus did not appear to be a handicap for our particular population. Only 4 subjects scored in the severe handicap range, with the majority of subjects (n = 24) scoring in the mild to no handicap range. We failed to find any significant relationship between tinnitus handicap and duration of pain, site of pain, or duration of tinnitus. We speculate that tinnitus might not be a significant problem in our population as these patients are so focused on their pain issues that all other symptoms become secondary. We did not score intensity or handicap from pain; therefore, we were not able to look at this in relation to tinnitus handicap. We also did not include an instrument to measure depression.
Several factors may have hampered our study. We did not have a control group and relied on historical data as a comparator. Our sample was nonrandomized and fairly small but extended over a significant time period. It is possible that a larger sample of patients or a larger sample of patients with pain at a specific site may reveal a more convincing association of pain and tinnitus.
CONCLUSION
Tinnitus is found at a high incidence in patients seen at a pain management clinic in the tertiary care setting. The tinnitus does not seem to be directly related to the specific complaint of pain and may not change despite successful pain management. Tinnitus was not perceived as a significant handicap in our sample of patients experiencing chronic pain.
Footnotes
APPENDIX: ABRIDGED VERSION OF TINNITUS SURVEY PAGE 1
Age: years
Gender: male, female
Site of pain
Do you have any of the following?
Hearing loss (Y/N)
History of ear infections (Y/N)
Vertigo (Y/N)
Imbalance (Y/N)
Tinnitus (Y/N)
Those without tinnitus stopped here, those with tinnitus were asked to continue.
Please grade the pitch of your tinnitus:
Low (like a foghorn) 1 2 3 4 5 6 7 8 9 10 High (like a whistle)
Please grade the volume of your tinnitus: Very faint 1 2 3 4 5 6 7 8 9 10 Very loud Have you had a history of noise exposure?
(Y/N) If yes please explain.
Did you wear ear protection? (Y/N)
Have you had a severe head injury? (Y/N)
How much caffeine do you ingest daily? (please include cups of coffee and caffeinated soft drinks)
How much aspirin containing products do you take daily?
How long have you had tinnitus? (in years)
Did it begin before, at the same time, or after your pain began?
Do you feel it is associated in any way with your pain?
Do any of the treatments you take for pain affect your tinnitus?
Appendix
Following are the correct digital object identifier (doi) numbers for the articles in the April 2003 issue of Otolaryngology–Head and Neck Surgery.
Hao S-P. The use of the facial translocation technique in the management of tumors of the paranasal sinuses and skull base. (Otolaryngol Head Neck Surg 2003;128:571–5) doi:10.1016/ S1094-59980300092–5
Ammari FF. Tuberculosis of the lymph glands of the neck: A limited role for surgery. (Otolaryngol Head Neck Surg 2003;128:576-80) doi:10.1016/S1094-59980300121–9
Chen Y-K. Keratoacanthoma of the tongue: A diagnostic problem. (Otolaryngol Head Neck Surg 2003;128:581–2) doi:10.1016/ S1094-59980300087-1
Moore BA. Maffucci's syndrome and cartilaginous neoplasms of the trachea. (Otolaryngol Head Neck Surg 2003;128:583–6) doi:10.1016/S1094-59980223292–1
Sutay S. Large submandibular gland calculus with performation of the floor of the mouth. (Otolaryngol Head Neck Surg 2003;128:587-8) doi:10.1016/S1094-59980223280-5
Wasinwong Y. Eustachian tube mature teratoma. (Otolaryngol Head Neck Surg 2003;128:589-91) doi:10.1016/S1094-59980223310-0
Pérez Fernández CA. Sudden deafness as a manifestation of the rupture of a cerebral arteriovenous malformation. (Otolaryngol Head Neck Surg 2003;128:592–4) doi:10.1016/S1094-599803 00130-X
Kelly TF. Endoscopic management of an intranasal hemangioma: A case report and literature review. (Otolaryngol Head Neck Surg 2003;128:595-7) doi:10.1016/S1094-59980223283–0
Nakahara H. Congenital-type nystagmus in Arnold-Chiari malformation. (Otolaryngol Head Neck Surg 2003;128:598-600) doi: 10.1016/S1094-59980223210-6
Vora NM. Metastatic leiomyosarcoma to the tongue. (Otolaryngol Head Neck Surg 2003;128:601–2) doi:10.1016/S1094-599802 23263–5
Derkay CS. Phonomicrosurgical techniques for treatment of RRP in children. (Otolaryngol Head Neck Surg 2003;128:603) doi:10.1016/ S1094-59980300006-8