
Abstract
OBJECTIVE: We evaluated the effectiveness of a management approach that combines the canalith repositioning maneuver (CRM) and vestibular rehabilitation (VR) in the treatment of benign positional paroxysmal vertigo (BPPV) in elderly persons.
STUDY DESIGN AND SETTING: Forty-seven patients (>70 years old) with the diagnosis of unilateral posterior semicircular canal BPPV formed the study population. This study has 2 parts. In the first part, patients were randomly assigned to 1 of 2 groups: the CRM and avoidance (no treatment). Patients were evaluated 1 month after the first visit. Those patients not responding to treatment were enrolled in the second part of the study, treated with an individualized combination of CRM and VR, and then reevaluated 3 months later.
RESULTS: Statistically significant improvement of vertigo and provoked nystagmus in 64% of patients in the CRM group compared with the no-treatment group. After the addition of VR, 77% of all patients improved.
CONCLUSION: A combination of CRM and VR improves BPPV in the elderly.
SIGNIFICANCE: These findings suggest that although CRM is more effective than no treatment, VR can be added to improve the results in the treatment of BPPV.
The currently accepted mechanisms of BPPV are cupulolithiasis 1 and canalithiasis, 5 but the exact pathophysiology of BPPV is still not completely understood. In cupulolithiasis, otoconial debris in the posterior semicircular canal becomes attached to the cupula, rendering this canal sensitive to gravity. In canalithiasis, the debris is assumed to be free-floating in the endolymph and to cause a hydrodynamic drag effect resulting in displacement of the cupula. Whether cupulolithiasis or canalithiasis, the displacement of these attached or free-floating particles by physiotherapeutic procedures is the basis of the most commonly used treatment modalities today. 6–16
The available treatment modalities for BPPV include expectant observation (due to anticipated spontaneous resolution), the avoidance of precipitating positions, medications, repositioning maneuvers, habituation exercises, and surgery. Because we could expect spontaneous self-reported resolution of symptoms in approximately half of the patients, 1,9 it is best to validate the success of any treatment modality using an untreated control group. Despite the abundance of reports of treatment of BPPV, only a few studies have used a control group. Blakley 9 compared the efficacy of the canalith repositioning maneuver (CRM) versus no treatment in 38 patients with BPPV and concluded that half of the patients show subjective improvement after 2 to 3 months regardless of treatment and the length of their symptoms. However, this study has been criticized for (1) using only a subjective method of outcome assessment rather than a repeat Hallpike test and (2) the addition of habituating exercises to those patients who have not improved by the first month of follow-up.
In contrast to reports of spontaneous recovery, Lynn et al 10 published a randomized, controlled trial showing the efficacy of treatment with a repositioning maneuver over that of a sham maneuver (control). At 1 month, 89% of the treatment group had a negative Hallpike, compared with a 27% rate of recovery for the control group patients. Other controlled studies have shown beneficial effects of repositioning maneuvers, 11–13 exercise therapy, 14,15 and the liberatory maneuver. 16 Conversely, antivertigo medications have been found to be ineffective in controlled clinical trials. 14 No studies with a proper control group have been performed to evaluate the efficacy of surgery in BPPV. Surgical interventions are reserved for recalcitrant cases and do carry a small risk of hearing loss.
Certain age-related comorbidities such as degenerative osteoarthritic disease, cerebrovascular disease, peripheral neuropathy, autonomic dysfunction, and cognitive dysfunction are more common in the elderly. These comorbidities may affect the performance of the maneuvers for the diagnosis and treatment of BPPV, such as the Dix-Hallpike test and the particle dispersion or repositioning maneuvers. In some elderly patients, these maneuvers may need to be modified to include gentle, slower movements and limited neck torsion. When these physiotherapeutic maneuvers are unsuccessful or when these maneuvers cannot be performed effectively due to limitations imposed by accompanying comorbidities, additional treatment modalities are indicated. The aim of this study is to evaluate the efficacy of a management approach that combines the CRM and a customized program of VR in the treatment of BPPV in a population of patients 70 years old or older.
PATIENTS AND METHODS
The study was conducted in a private neurotologic practice. Patients aged 70 years or older were eligible for the study if they had complaints of vertigo provoked by changes in head position, lasting less than 1 minute, and accompanied by the typical vertigo and nystagmus of posterior semicircular canal BPPV during the Dix-Hallpike test using Frenzel glasses. The diagnosis of posterior canal BPPV was based on the observation of torsional-upbeating nystagmus, lasting less than 1 minute, elicited during the Dix-Hallpike test, with the fast phase of the superior pole of the eye moving toward the undermost ear.
All of the subjects underwent a comprehensive evaluation directed to identify other labyrinthine or neurological disorders. This evaluation included a history, physical examination, an evaluation of spontaneous, head-shake and positional nystagmus with Frenzel glasses, Romberg test, audiogram, and electronystagmography. Demographic data and duration of symptoms until treatment were recorded for each patient. We only included patients with unilateral posterior semicircular canal BPPV who completed the first part of the study; we excluded patients with other forms of BPPV and those who did not return for the follow-up visits.
This study is divided into 2 parts. The first part is a prospective, randomized, controlled trial of the efficacy of the CRM. During the patients' first visit, after confirming the diagnosis of BPPV by the results of the Dix-Hallpike test, the subjects were randomly assigned (random number tables) to either the CRM group or the no-treatment group. We discussed with all of the patients the diagnosis of BPPV and the options for treatment and obtained their informed consent before they enrolled. Subjects in the treatment group underwent CRM at the first visit and returned 1 month later for electronystagmography and reevaluation. Control patients were scheduled to return in 1 month for the completion of electronystagmography, at which time we repeated the Dix-Hallpike test and performed CRM if still needed. The subjects in both groups were instructed to avoid the vertigo-provoking movements and to use antivertigo medication as needed.
The electronystagmography test comprised tests of oculomotor function (saccades, smooth pursuit, optokinetic nystagmus), spontaneous nystagmus with and without visual fixation, gaze-evoked nystagmus, positional nystagmus, and bithermal caloric testing. Horizontal and vertical eye movements were recorded with skin electrodes.
We perform a modification of the Epley maneuver 7 as follows: while in the sitting position, the patient's head is turned 45 degrees toward the affected ear and then the patient is moved into the Dix-Hallpike supine position with minimal head extension. The characteristic nystagmus is observed with Frenzel glasses and, when the nystagmus ceases, the head is slowly turned 90 degrees to the opposite Dix-Hallpike position. After 1 minute, the patient is slowly returned to a sitting position and instructed to tuck his or her chin. Mastoid oscillation is used on the affected side throughout the maneuver. The maneuver is repeated up to 3 times if the nystagmus persists. The patient is instructed to use a soft cervical collar, to sleep in an upright position, and to avoid strenuous or vertigo-provoking movements for 48 hours.
The criteria for success were the absence of the characteristic vertigo and nystagmus during Dix-Hallpike test with Frenzel glasses, 1 month after the initial visit. Eliciting vertigo and/or nystagmus was considered as the persistence of BPPV and therefore a treatment failure. We recorded the treatment results at the first visit (immediately after performing the CRM) and at 1 month.
Patients in the control group that showed persistence of nystagmus and/or vertigo at the 1-month visit underwent treatment with the modified Epley maneuver as described here. Their results (vertigo and nystagmus) were noted immediately and at 1 month after treatment.
In the second part of the study, 18 subjects with persistence of the BPPV vertigo or nystagmus were enrolled in a supervised program of vestibular rehabilitation (VR) that included particle-dispersing exercises 6 and customized habituation exercises. 15 The physical therapist (R.H.) performed the initial assessment and designed the customized VR program for each patient. She explained the rationale for and potential problems of the exercises and met with patients 2 or 3 times a week for 4 to 6 weeks. She guided patients and ensured they performed the head and body movements vigorously enough to maximize results. In addition, patients were instructed to perform the exercises at home twice a day. At the end of the 4- to 6-week period, the patients were referred to the neurotology clinic for a repeat evaluation that included the Dix-Hallpike test.
Statistical analysis included χ 2 test for discreet variables and 2-sample Student t test for continuous variables.
RESULTS
Figure 1 shows the results and flow of the 2 parts of this study. Table 1 shows data on patient gender, age, side of lesion, duration of symptoms, abnormal electronystagmographic results, and cure rate for the control and treatment groups. At the 1-month follow-up visit, 64% (18 of 28) of patients in the treatment group and 5% (1 of 19) of patients in the control group had a negative Dix-Hallpike test (no vertigo or nystagmus). This difference is statistically significant (χ 2 difference [df] = 1; P < 0.001). The control and treatment groups did not differ in age, gender ratio, side of lesion, duration of symptoms, and prevalence of abnormal electronystagmographic results.
Eighteen patients from the control group who still had a positive Dix-Hallpike after 1 month of observation were treated with CRM. One month after CRM, 10 patients had a negative Dix-Hallpike test, 2 patients had positioning vertigo but no nystagmus during the Dix-Hallpike test, and 6 patients had both vertigo and nystagmus during the Dix-Hallpike test. Patients with positioning vertigo and/or nystagmus 1 month after treatment are considered CRM failures. The cure rate of this subgroup of 18 patients was not different from the cure rate of the treatment group (χ 2 test, [df] = 1, P = 0.553).
In the second part of this study, 18 patients who were CRM failures were then enrolled in the VR program: 10 patients from the treatment group in the first part of the study and the 8 patients who were observed for 1 month (control group) and then treated with CRM without success. After 6 weeks from the onset of VR, 7 patients were cured (no vertigo and negative Dix-Hallpike), 6 patients had a positive Dix-Hallpike (2 patients with nystagmus and vertigo, 4 patients with vertigo but no nystagmus), and 5 patients failed to complete the VR program or to return for a final assessment with a repeat Dix-Hallpike. Overall, 77% (36/47) of subjects were cured, and 11 patients (23%) either dropped out or failed treatment with CRM and VR.
It is noteworthy that during the performance of the Dix-Hallpike test in this cohort, we did not observe any patient with BPPV nystagmus who did not also report positioning vertigo. After treatment, patients had either a negative Dix-Hallpike test (ie, no vertigo or nystagmus) or a positive test (ie, vertigo with or without nystagmus).
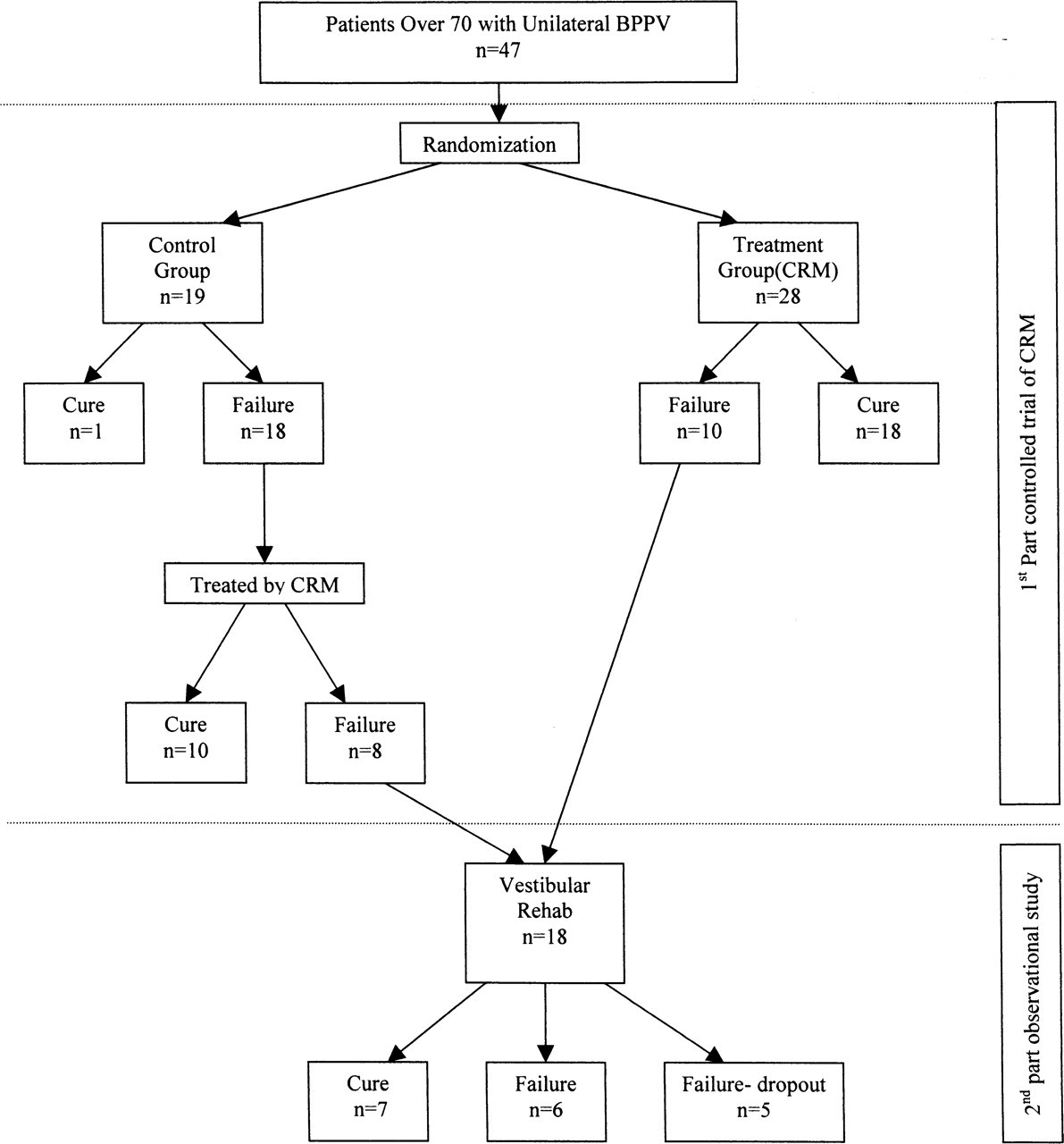
Systematic management of BPPV in the elderly: study flow and results.
DISCUSSION
This study clearly shows a beneficial effect of CRM for posterior semicircular canal BPPV in elderly persons. There was significant improvement of the provoked vertigo and resolution of the typical nystagmus. Improvement was already evident immediately after completion of the CRM session (1 to 3 treatments) and was not associated with any adverse side effects. Although spontaneous resolution is a possibility, the effectiveness and simplicity of CRM warrants its use as the first line of treatment for BPPV in the elderly.
Demographic data and treatment response in 47 elderly patients with posterior semicircular canal benign positional paroxysmal vertigo
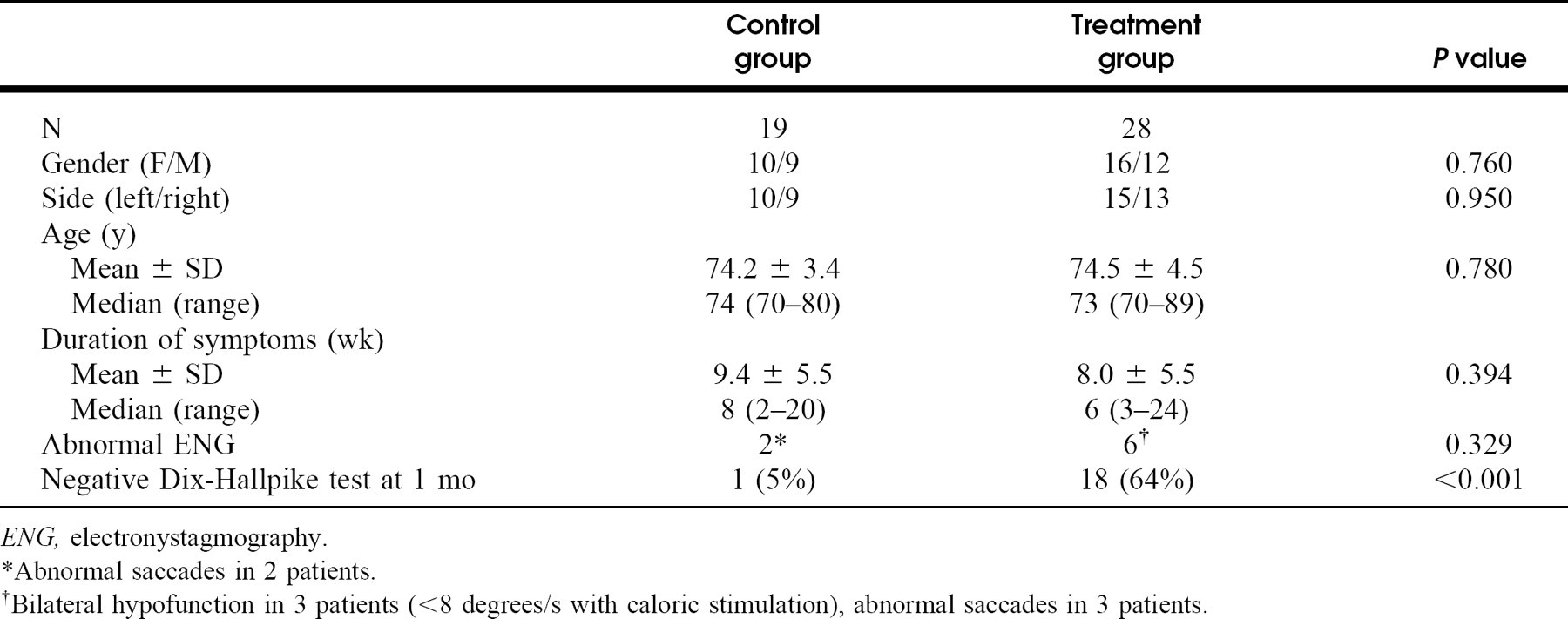
ENG, electronystagmography.
*Abnormal saccades in 2 patients.
†Bilateral hypofunction in 3 patients (<8 degrees/s with caloric stimulation), abnormal saccades in 3 patients.
The diagnosis of BPPV is usually evident on the history and physical examination, and quantitative vestibular laboratory testing (ie, electronystagmography) is not required. It is important to observe nystagmus carefully and to recognize manifestations that accompany other diagnoses, such as unilateral hearing loss, tinnitus, atypical nystagmus, or other neurologic deficit. 17 In cases where the diagnosis is in doubt or when patients fail to respond to conservative treatment such as CRM, other evaluations may be indicated.
Osteoarthritic spine disease and cerebrovascular disease are prevalent in the later years of life. Elders with these comorbidities present a challenge to the diagnosis and treatment of BPPV. Although adverse side effects of the repositioning maneuver have seldom been reported, 16 both the Dix-Hallpike test and the repositioning maneuvers involve significant neck torsion and extension, which can result in strain on the spine column, vertebrobasilar system insufficiency, and dislodged carotid artery atheromatous emboli. Patients at risk should be identified during the anamnesis and physical examination.
We have found that only minimal neck extension such as that obtained by having the patient's head rest flat on the table is necessary to elicit nystagmus, and therefore we were able to avoid the head hanging position during the Dix-Hallpike test. When performing the CRM, a nurse stands by the table's side to support the patient's body and limbs, while the practitioner holds the head to avoid extreme lateral torsion of the neck. Moreover, we avoid the classic Semont or liberatory maneuvers in the elderly because they require some degree of swiftness when bringing the patient from the sitting position to the supine position and therefore may cause more strain on the spine.
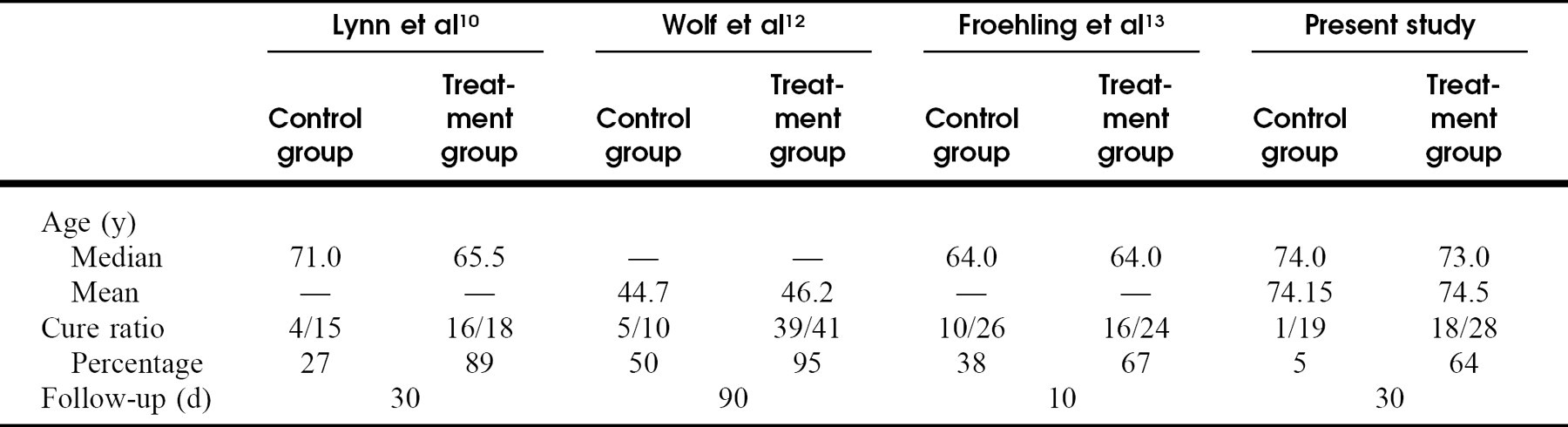
Although our results with CRM are encouraging, they remain modest in comparison to other published series with patients of all ages. When considering only randomized, controlled studies that have used both subjective reporting and Hallpike testing as the method of assessment, the rate of success of CRM (Epley's maneuver) ranges from 67% to 93.5% 10,12,13 (Table 2). Studies that include patients of all ages have failed to show an influence of age on the outcome. 12,13 The most significant difference between these studies, besides our cohort's higher median age, is our seemingly lower rate of spontaneous recovery. It is possible to argue that we were successful in achieving a statistically significant difference due to the low rate of spontaneous recovery, rather than due to a high rate of success with CRM. This fact does not argue against the beneficial effect of CRM but instead draws attention to other factors that make our cohort different to those from other controlled studies, such as the patient's age.
Randomized, controlled studies of canalith repositioning maneuver for benign positional paroxysmal vertigo that used a posttreatment Dix-Hallpike test as outcome measure.
We do not believe that our technique of CRM could account for the difference in results: our modification to the Epley's maneuver is only subtle (limited neck extension and the use of mastoid oscillation), and with this technique we achieved a relatively high cure rate. One possible explanation for the lower spontaneous recovery observed in our cohort is that older patients have a delayed habituation effect as a result of their expected decrease in vestibular function, multisystem degeneration, and less movement in daily activity. 18,19 Moreover, Zucca et al 18 have put forward an hypothesis for the spontaneous resolution of BPPV. These authors showed that the rate of otoconia dissolution in endolymph is dependent on the calcium content in the endolymph. Despite the fact that the pathogenesis and treatment of canalithiasis have only a physical basis, nonphysical factors such as age-related differences in vestibular habituation and endolymphatic calcium content may tentatively serve as explanations for variations in response to treatment. Further research is needed to understand the role of these and other nonphysical factors in BPPV.
Despite satisfactory results with CRM, there remain a substantial number of patients with persistent symptoms of BPPV. In this series, 18 of 47 patients continued to have vertigo and nystagmus during the Dix-Hallpike test at 1 month after CRM. What to do with patients for whom CRM fails remains a matter of debate. Based on our clinical experience, most patients prefer to try another treatment modality than to wait for spontaneous recovery. At this point, we recommend the performance of electronystagmography and an evaluation by the physical therapist. We aim to identify coexisting conditions that may affect treatment such as peripheral or central vestibular dysfunction, osteoarthritic disease, and poor exercise tolerance. Then, the physical therapist suggests an exercise program (VR) that addresses the particular needs of the patient. This customized program comprises a combination of particle-dispersion maneuvers 6 and habituation exercises 15 to treat BPPV. Particle-dispersion exercises are emphasized in patients with positioning vertigo and nystagmus, and habituation exercises are emphasized in those with motion-provoked dizziness. Adaptation, substitution, and general conditioning exercises are included if needed for patients with other coexisting vestibulopathies and poor exercise tolerance, as well as for the symptoms of imbalance that may persist after CRM. 19
Although the superiority of supervised exercises over home self-guided exercises has not been validated by well-designed, controlled studies, we and others 20 believe that supervision is instrumental in providing both motivation and instruction in the correct execution of the exercises to maximize results. Supervised and customized exercise programs may have even more relevance in the population of elderly patients with BPPV because this group has been found to have relatively high rates of functional disability and depression. 2 In our study, an additional 7 of 13 patients who completed a supervised VR program had a successful result (ie, no vertigo and nystagmus during the Dix-Hallpike test). We observed a dropout rate of 28% (5 of 18 patients) in our VR program; 4 of 5 patients did not complete the program or return to follow-up visits due to other medical problems, which underlies the significance of associated co-morbidities in the elderly.
We propose this step-by-step management approach for BPPV in the elderly, based in our experience and the review of the relevant studies: patients with motion-provoked symptoms suggestive of BPPV undergo a history and physical examination focused not only to diagnose BPPV (Dix-Hallpike test with Frenzel glasses) but also to identify associated vestibular hypofunction, osteaoarthritic spine disease, and cerebrovascular disease. Patients with positive findings other than a positive Dix-Hallpike test undergo further evaluation. After a discussion of the pathogenesis of BPPV and the rationale of the different treatment modalities, patients with a positive Dix-Hallpike test are offered CRM. We perform the modified Epley maneuver with mastoid oscillation, repeat the repositioning maneuver until nystagmus disappears or up to 3 times in 1 session, and provide the patient with postmaneuver instructions. The patient returns in 2 to 4 weeks for repeat Dix-Hallpike testing and, if the test is negative, no further treatment is needed. If the test is positive, we repeat CRM and order electronystagmography. The patient will return again in another 2 to 4 weeks for repeat Dix-Hallpike testing and review of the electronystagmographic results. Symptomatic patients with persistent BPPV and/or vestibular hypofunction on electronystagmography are then enrolled in the customized VR program. Recurrences are managed either with CRM, home-exercise program, or supervised VR depending on the patient's previous experience with those modalities. Continuous surveillance of recalcitrant or recurrent cases is carried out not only to identify possible misdiagnoses or BPPV variants but also to provide support in terms of reassurance, fall prevention, and coping skills for living with “dizziness.” This management approach has proved safe and effective in the majority of our older patients with BPPV.