
Abstract

We report the case of a patient who had undergone a laryngectomy and repeatedly aspirated the spray covers of pharmaceutical mucofluidificant solutions during the care of his stoma.
CASE REPORT
A 57-year-old man was admitted to the emergency ward of our department in August 2001 with a 2-day history of progressive worsening dyspnea and mental confusion. The patient had undergone total laryngectomy for cancer of the larynx 4 years earlier and was regularly followed without any respiratory or neurologic symptoms. On physical examination, the patient was cyanotic, afebrile, confused, and agitated, with a respiratory rate of 20/min and heart rate of 115 beats/min. His blood pressure was 95/60 mm Hg. Respiratory sounds were reduced bilaterally. An electrocardiograph showed sinus tachycardia. Arterial blood gases on ambient air revealed respiratory acidosis (PAo2 = 6.13 kPa (46 mm Hg), PACO2 = 9.3 kPa (70 mm Hg), pH 7.30, and HCO3 = 30 mmol/L). The chest radiograph revealed left lower lung opacization and slight enlargement of the right lung. Despite prompt airway aspiration and oxygenation through the stoma, the clinical picture deteriorated and mechanical ventilation was started. Next, fiberoptic bronchoscopy was performed. During the examination, a first transparent foreign body was detected in the right main bronchus (Fig 1a); a second transparent foreign body was seen in the left main bronchus (Fig 1b). Once the 2 foreign bodies were removed with the aid of a rigid bronchoscope and an alligator forceps, a third similar foreign body appeared at the level of the intermediate bronchus (Fig 1c). All 3 foreign bodies were identified as the plastic spray covers of a pharmaceutical mucofluidificant solution (Acqua di Sirmione, Byk Gulden, Italy), each cover marketed as a disposable piece contained in a 6-vial box (Fig 1d). After the removal of foreign bodies, the patient's condition rapidly improved with normalization of arterial blood gases within 24 hours. Mechanical ventilation was discontinued. A second bronchoscopy was performed to aspirate some bloody mucus occurring thereafter. On direct questioning to patient's kin, his wife stated that 2 months earlier, after a quarrel, the patient began taking care of his tracheostomy using the spraying solution 3 times a day every day. When clinically stable, the patient said he was unaware of the presence of the spray cover, having regularly used and completely consumed 12 vials during the past 2 months.
DISCUSSION
This patient could have repeatedly aspirated 3 transparent spray covers while taking care of his stoma. So far in the English-language literature, only 4 cases of single aspirated foreign body (a brush, 2 a button, 3 a piece of wire, 4 and a safety pin 5 ) in patients with a permanent tracheal stoma have been reported, easily recognized, and regarded as exceptional circumstances. Spraying solution in the stoma is commonly recommended in laryngectomy patients to prevent hypersecretion and crusting in the stoma or cannula. 6 Noticeably, this type of spray cover is identical to other spray mucofluidificant solutions used in Italy.
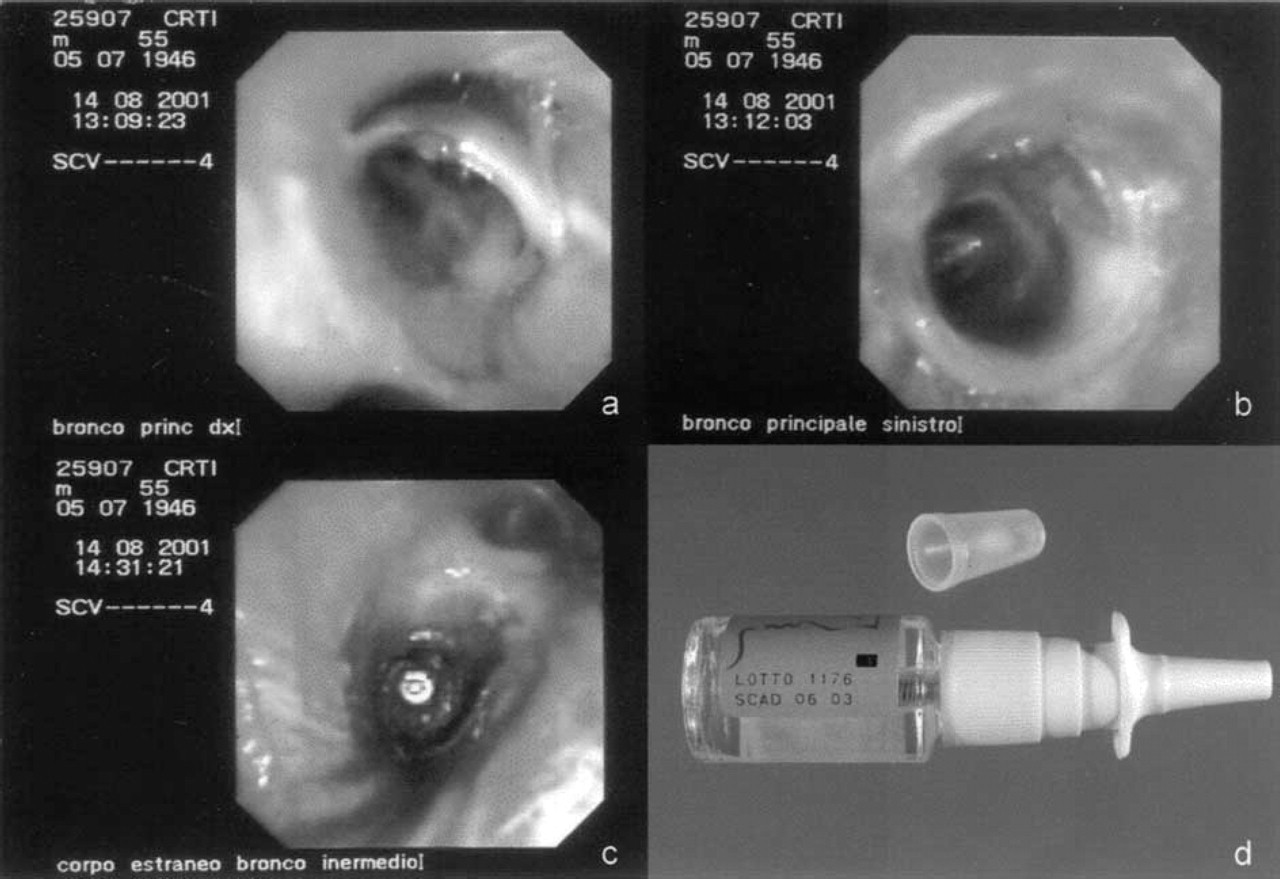
Endoscopic images of 3 spray covers aspirated through the tracheal stoma by the laryngectomized patient into right main bronchus (
Remarkably, in the patients with tracheostomy or laryngectomy, a vacuum effect may be generated when deep breathing or a paroxysm of cough generates a negative pressure gradient. This may facilitate the aspiration of an object held loosely around the stoma, such as the spray cover in this case.
Besides the free access to the lower airways, foreign body aspiration in laryngectomy patients poses additional problems in management. The larger size or sharp borders of the foreign body requires the use of rigid bronchoscopy to remove it. Half of laryngectomy patients are said to require thoracothomy after the failure of endoscopic procedures. Furthermore, the passage of the scope through the stoma itself could be difficult in laryngectomy patients because of the interference of the chin, even when the neck is hyperextended. In our patient, flexible bronchoscopy was very useful in locating foreign bodies along the tracheobronchial tree, while rigid bronchoscopy resulted mandatory both to maintain an airway for ventilation during the procedure and to use the extraction instruments.
In conclusion, the presence of a tracheal stoma could be a predisposing condition to potentially life-threatening foreign body inhalation in laryngectomy patients. The education of the patient in proper care of the stoma should be advised, including the risk of daily spraying maneuvers close to the stoma.