
Abstract

CASE REPORT
A previously healthy 14-year-old girl presented with a 3-month history of left purulent rhinorrhea, progressive nasal obstruction, and intermittent epistaxis, unresponsive to oral antibiotics. Fiberoptic examination revealed a large vascular polypoid mass completely filling the left nasal cavity. A computed tomography (CT) scan of the sinuses revealed a large mass that appeared to be originating from the left anterior ethmoid complex. There was no bony erosion or contiguous spread, and the remaining sinuses, orbit, and cranial fossa were uninvolved (Fig 1A).
The patient was taken to the operating room and underwent complete removal of the mass via an endoscopic sinus approach. The procedure entailed a left middle meatal antrostomy, complete anterior ethmoidectomy, and partial posterior ethmoidectomy. The mass was large, lobulated, and vascular. It was emanating from the ethmoid complex and coursing through the middle meatus to fill the nasal vault and choana. Based on histologic analysis and confirmatory molecular studies, a diagnosis of EES was made. An extensive metastatic work-up postoperatively was negative; this included CT scans of the sinus, brain, chest, abdomen, and pelvis; magnetic resonance imaging of the brain and sinus; bone scanning; bone marrow aspirate; and biopsy.
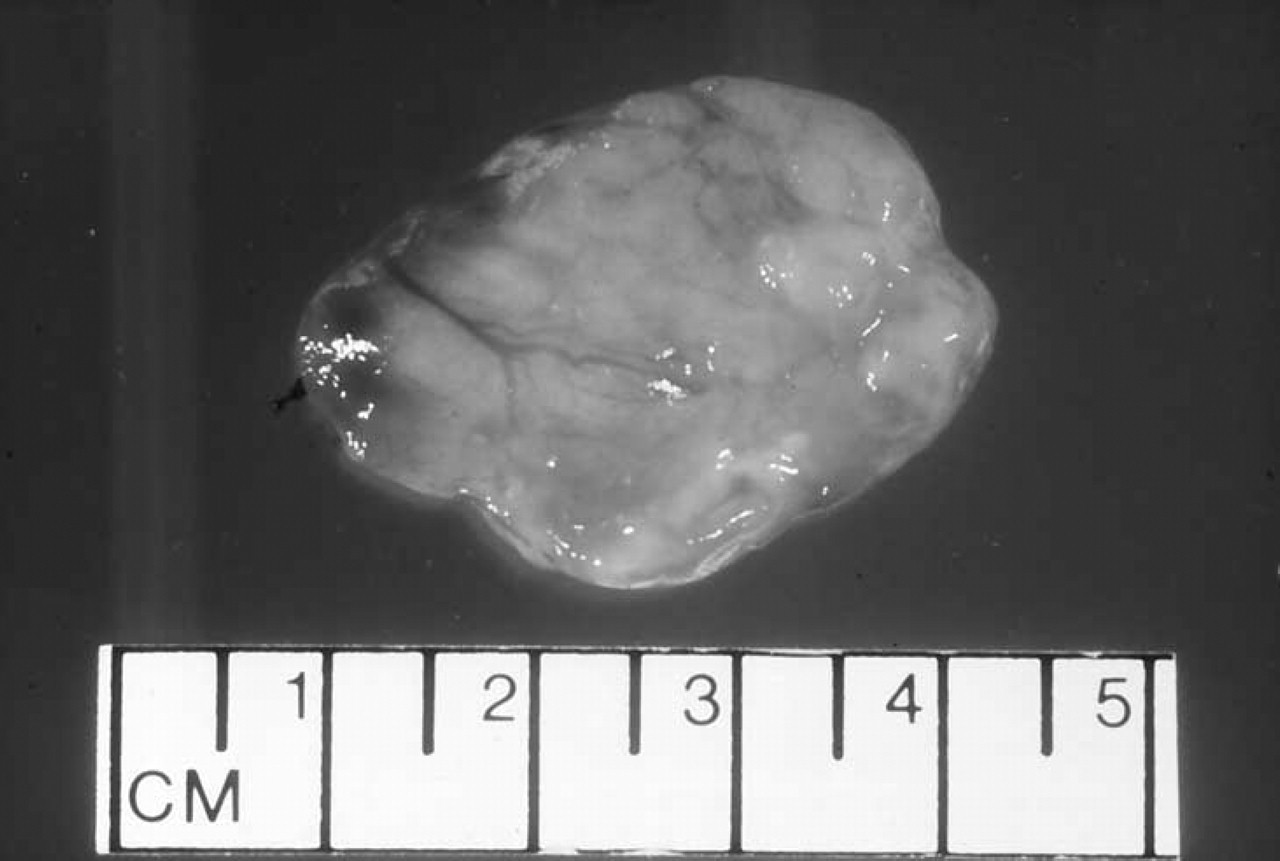
Gross examination of the mass revealed irregularly shaped friable pink-tan tissue measuring 3.5 × 2.5 × 1.5 cm. On sectioning, it had a variegated red-tan color and a soft consistency (Fig 2). Microscopic analysis revealed an undifferentiated tumor consisting of a solid sheet of small, round blue cells. Mitotic figures are present as well as individual cell necrosis (Fig 3A). Multiple stains of the specimen were performed. Of these stains, the most diagnostic was the CD99 stain, which was strongly positive (Fig 3B). Molecular studies using polymerase chair reaction (PCR) analysis confirmed the chromosomal translocation characteristic of ES.
The patient was treated with combined chemotherapy/radiotherapy. The adjuvant chemotherapy followed the Children's Cancer Group protocol 7942, regimen A, which consisted of treatment every 3 weeks with vincristine, doxorubicin, cyclophosphamide alternating with ifosfamide and etoposide through week 33 (12 cycles total). At week 12, the patient received radiation therapy for local control (total dose of 5040 cGy in 28 fractions). Small-field radiation therapy was administered to the ethmoid sinus region with minimal radiation of the orbit and brain. Treatment was completed on September 5, 2000, and the patient has done well without evidence of recurrence or metastasis (Fig 1B).
DISCUSSION
ES is part of a class of poorly differentiated malignancies known as the peripheral primitive neuroectodermal tumors (pPNETs). These occur most commonly in young adults and include ES, peripheral neuroepithelioma, and Askin tumor. EES shares histologic, immunohistochemical, and molecular findings with ES of bone. The CD99/ MIC2 identified by the 013 antibody is a useful immunohistochemical marker for EES. CD99/ MIC2 is a cell surface glycoprotein found in virtually all ES and pPNETs, and is detected by the antibody 013. Immunoreactivity to 013 has been shown in up to 98% of ES/pPNETs (no cases of neuroblastoma were positive in this series). 5,6 More than 95% of pPNETs show the characteristic translocationt(11;22)(q24;q12) or the variantt(21; 22)(q22;q12). These translocations fuse the 5' portion of the EWS gene on chromosome 22ql2 to either FLI1 on 11q24 or ERG on 21q22. The resultant fusion genes (EWS/FLI1 or EWS/ERG) express chimeric proteins that are capable of cell transformation and act as aberrant transcription factors. Identification of the fusion transcripts EWS/FLI1 or EWS/ERG by PCR analysis serves as a sensitive and specific diagnostic test for pPNETs. 7
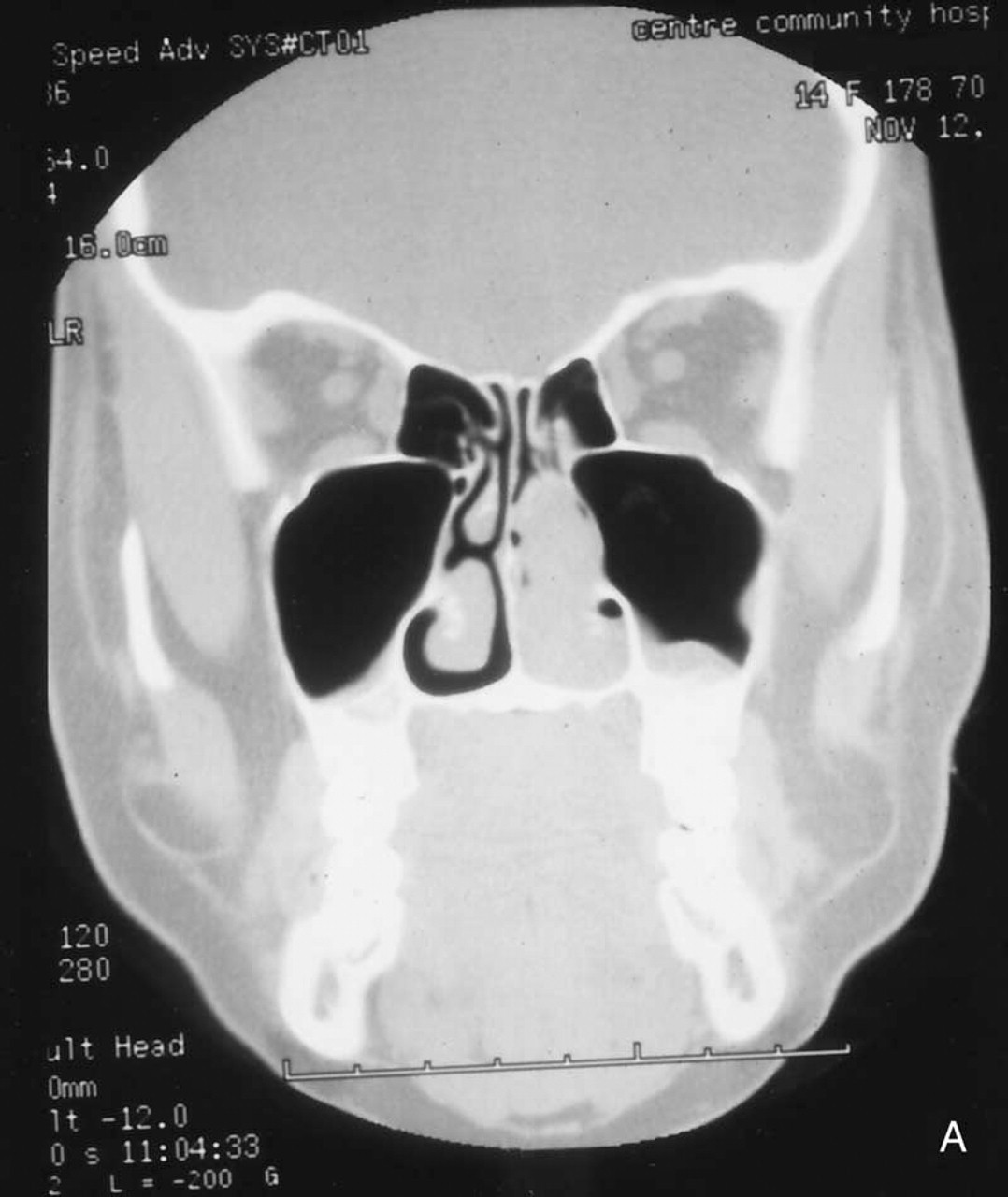
Coronal CT of sinuses revealing left nasal mass. Mass is emanating from anterior ethmoid cells. No bony destruction is noted.
EES is a rare tumor most frequently involving the soft tissue of the lower extremity and the paravertebral region. The head and neck region is involved in 2% to 3% of all ESs. The majority of these cases occur in the mandible or maxilla. A review of the world literature reveals a total of 5 cases of ES involving the nasal cavity and/or sinuses.
Howard and Daniels 1 reported 2 cases of ES of the nose. The first occurred in a 14-year-old boy with bilateral sinus involvement and extension to the anterior fossa dura. He was treated with surgical resection followed by chemotherapy/radiotherapy. The patient was without disease at 5-year follow-up. The second case was that of a 28-year-old Asian woman who presented with a recurrence of a previously excised mass of the nasal tip. This was an ES of the nasal soft tissue and was treated with partial rhinectomy (patient refused postoperative chemotherapy/radiotherapy). The patient was disease free at 4-year follow-up.
Coronal CT of sinuses performed 1 year after surgery. Note the good sinus aeration and absence of any tumor.
Gross examination of the 3.5 × 2.5 × 1.5-cm nasal mass reveals pink-tan tissue and a soft consistency.
Lane and Ironside 2 reported a case of EES of the ethmoid sinus with orbital invasion in a 7-year-old boy. This patient received chemother- apy after undergoing a partial ethmoidectomy for biopsy. The patient underwent craniofacial resection after chemotherapy. No follow-up was described in this article. Pontius and Sebek 3 described a 39-year-old man who was noted to have an ES of the left nasal cavity and sinuses without bony erosion or metastasis. The patient was treated with craniofacial resection followed by radiation therapy, without evidence of recurrence at 2-years follow-up. Boor et al 4 presented the case of a 20-year-old woman with EES of the nose. Surgical excision followed by chemotherapy/radiotherapy resulted in no disease at 1-year follow-up.
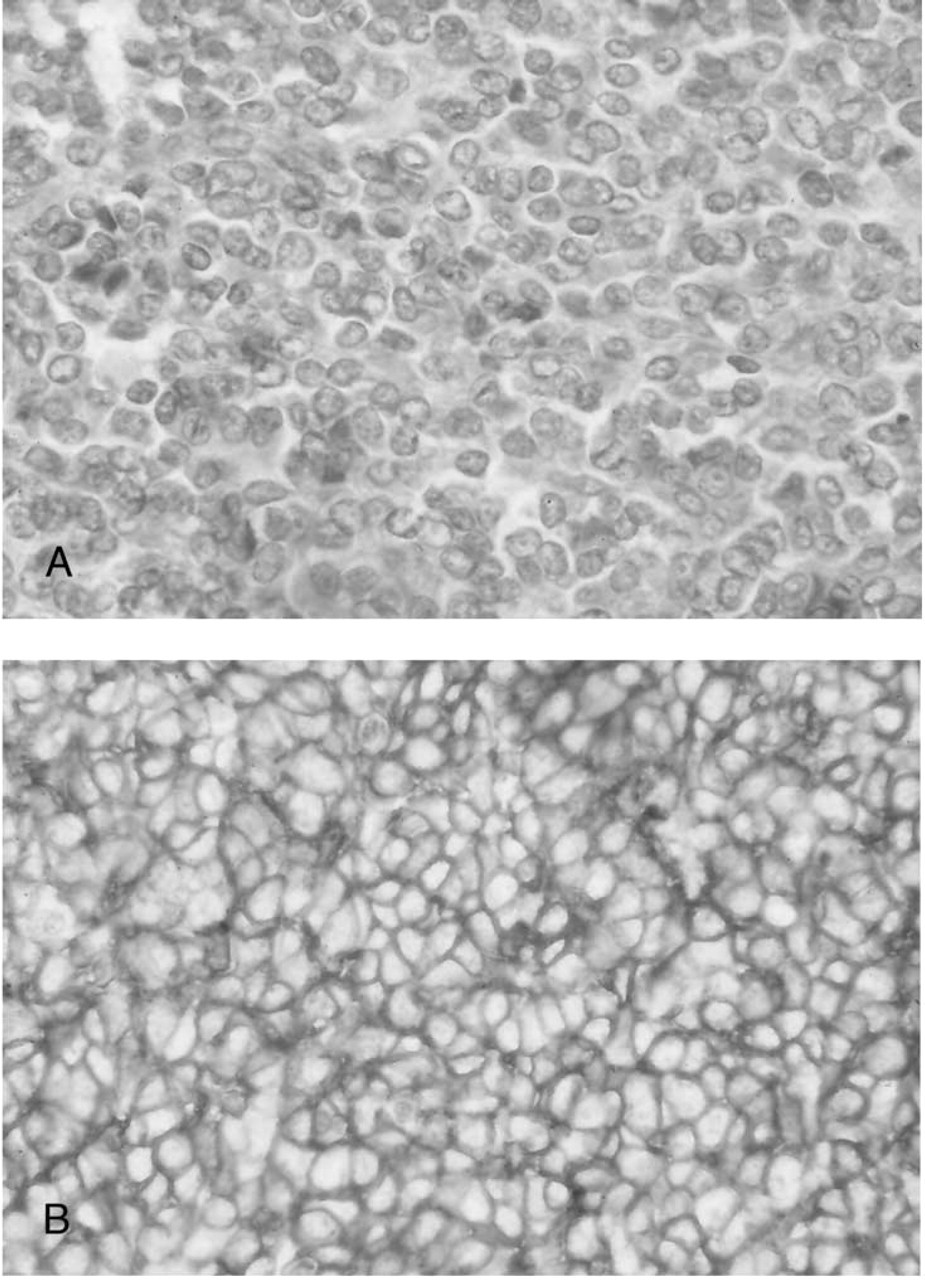
Solid sheet of small blue cells. Occasional mitotic figure and individual cell necrosis is seen (hematoxylin-eosin stain; original magnification, x 1000).
In the past, distinguishing ES from other small round cell neoplasms was difficult. The differential diagnosis of small round blue cell tumors includes malignant lymphoma, rhabdomyosarcoma, olfactory neuroblastoma, ES, reticulum cell sarcoma, acute leukemia, and others. 1,2 Modern diagnostic studies including CD99/O13 immunostaining and molecular studies using PCR to detect characteristic chromosomal translocations (EWS/FLI1 or EWS/ERG) are truly definitive for ES. Combined surgical excision of gross disease and chemotherapy/ radiotherapy appears to be the most effective treatment plan.