
Abstract
OBJECTIVE: The aim of this study was to investigate the treatment outcome of N3 nodal disease.
STUDY DESIGN: A single institution retrospective nonrandomized study was conducted. A total of 53 patients with primary presentation of squamous cell carcinomas from various head and neck sites from 1980 to 1994 were recruited for this study. Eight patients with nasopharyngeal cancers who underwent treatment with palliative intent were excluded from the study. Treatment options were broadly divided into 4 treatment categories; postoperative radiotherapy; preoperative radiotherapy; surgery alone; and chemotherapy pre- or postoperatively with or without radiotherapy.
RESULTS: Mean age of the participants was 63 years (SD = 8.2); 93% were men. Median follow-up period was 12 months (range, 5 to 184 months). Of the 45 N3 patients, 21 patients had a recurrence in the neck after treatment, with 1 in the contralateral neck. The overall rates of control in the neck at 1, 3, and 5 years were 73.1%, 34.6%, and 26.9%, respectively. The 1, 3, and 5-year neck control rates for each main group were 92.3%, 46.1%, and 46.1% with postoperative radiotherapy; 66.7%, 33.3%, and 11.1% with preoperative radiotherapy and 33.3%, 0%, and 0% with surgery alone. Overall survival rates at 1,3, and 5-years were 52.8%, 25%, and 22.2%. Survival rates in those who received radiotherapy were better than those who only had surgery. The 5-year survival rate was significantly higher for those who had postoperative radiotherapy (38.9%) compared with patients who had preoperative radiotherapy (9.1%) and surgery alone (0%).
CONCLUSION: Our treatment outcomes, particularly those in the group receiving postoperative radiotherapy, were similar to other studies. The prognosis of N3 neck disease was poor but improved with radiotherapy, particularly postoperative radiotherapy. The role of definitive chemotherapy and/or radiotherapy and salvage surgery is difficult to evaluate as the results are inconsistent and the available data are limited. Future studies in particular with quality of life assessment are needed to evaluate the management of N3 head and neck cancer.
The purpose of this study was to evaluate the treatment outcome in patients with N3 nodal disease in a single tertiary institution.
PATIENTS AND METHODS
A retrospective review was conducted on all patients with primary presentation of stage N3 neck disease from head and neck squamous cancer at the Royal Melbourne Hospital, Victoria, Australia, between 1980 and 1994. All patients with clinically palpable neck nodes of at least 6 cm in diameter were recruited for this study. A total of 53 patients were eligible for this study. Two patients with nasopharyngeal carcinoma and 6 patients treated with palliative intent were excluded from this study.
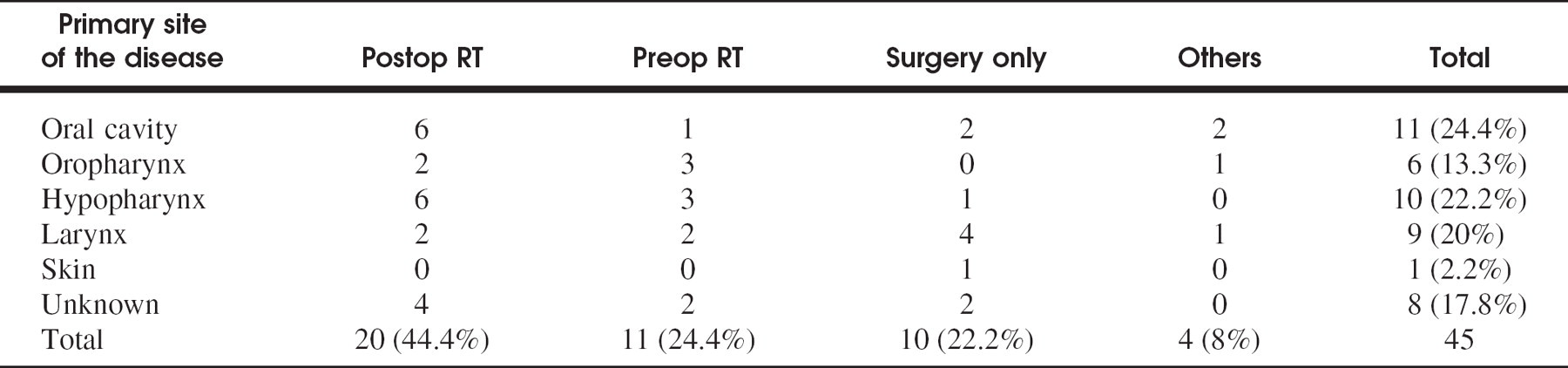
Distribution of primary site of the disease
The patients were classified into 4 groups based on the treatment received; those treated with neck dissection followed by radiotherapy on a daily basis at 1.8 or 2.0 Gy/fraction to a total of 45 to 50 Gy over a period of 4 to 6 weeks (Postop RT); those who had a preoperative radiotherapy of 1.8 to 2.0 Gy/fraction to a total of 60 to 70 Gy over a period of 6 to 8 weeks followed by planned neck dissection surgery (Preop RT); those who were treated only with neck dissection surgery due to their refusal to have radiotherapy or who died before radiotherapy; and those who had pre- or postoperative chemotherapy with or without radiotherapy.
Chemotherapy consisted of either a 5-Fluorouracil and cisplatin-based regimen or a cisplatin and bleomycin-based regimen. Emphasis was not given to patients who had chemotherapy or chemoradiotherapy because of the smaller number of patients and inconsistent treatment protocol. Neck dissections were performed either as radical or modified radical neck dissections. In general, a level I to V clearance of regional cervical nodes were performed with preservation of the spinal accessory nerve where possible. Tumor-Nodal-Metastasis (TNM) classification 12 of head and neck cancer was used to classify the local stage of the primary disease.
Data were obtained from the records available at the primary hospital and radiotherapy centers in Melbourne. The patients' death was confirmed through the cancer death registry. Data collected included age, gender, site, and T-stage of primary disease, treatment received, histologic clearance, recurrence, and cause and time of death. Patients were evaluated for evidences of recurrence in the primary site, cervical region, or distant sites. In the neck control rates, disease-free survival and overall survival were calculated. Data were analyzed using SPSS statistical software. Kaplan-Meier survival analysis was used to estimate overall survival and disease survival rate. P < 0.05 was considered to be statistically significant.
RESULTS
A total of 45 patients were included in this study with a mean age of 63.1 years (SD = 8.2). Of these, 93% were males. Of the 45 patients, 20 (44.4%) patients had postoperative radiotherapy, 11 (24.4%) patients had preoperative radiotherapy, 10 patients (22.2%) had only surgery, and the remaining 4 (8.8%) patients had chemotherapy either pre- or postoperatively with or without radiotherapy.
Of the 45 patients with N3 disease, the primary site of the disease was found in the oral cavity in 11 (24.4%) patients, oropharynx in 6 (13.3%) patients, hypopharynx in 10 (22.2%) patients, larynx in 9 (20%) patients, and skin in 1 (2.2%) patient. The primary site of the disease was unknown in 8 (17.8%) patients Table 1. Of the 45 patients, 5 (11.1%) patients had T1 stage, 8 (17.8%) patients had T2 stage, 11 (24.5%) patients had T3 stage, and 5 (11.1%) patients had T4 stage. The T-stage of the disease could not be assessed in 16 (35.5%) patients because of inadequate information Table 2.
Of the 45 patients, follow-up data were not available for 6 patients; 2 of these patients had postoperative radiotherapy; 3 patients had only surgery; and 1 patient had postoperative chemoradiotherapy. The median follow-up period was 12 months (range, 5 to 184 months). Of the 39 patients with adequate follow-up data, 25 (64.1%) patients had recurrence. Twenty had recurrent disease in the treated neck, 1 patient had disease in the contralateral untreated neck, 8 patients had distant, and 3 patients had primary recurrences. Of the 20 patients with recurrence in the treated neck, 6 patients had postoperative radiotherapy, 7 patients had preoperative radiotherapy, 4 patients had only surgery, and 3 patients had adjuvant chemotherapy. Of the 11 patients who received preoperative radiotherapy, 3 (27.3%) had no viable tumor present on histopathologic assessment and none of these had documented neck recurrences at a late stage. Patients who had chemotherapy or chemoradiotherapy were not included in the analysis of neck control and survival rates.
Distribution of T-stage of primary site (TNM classification UICC-AJCC 1986)

Neck control rates at 1-, 3- and 5-year

The 1-, 3-, and 5-year neck control rates were 92.3%, 46.1%, and 46.1%, respectively, with postoperative radiotherapy; 66.7%, 33.3%, and 11.1% with preoperative radiotherapy; and 33.3%, 0%, and 0% with surgery alone. The overall neck control rates at 1, 3, and 5 years were 73.1%, 34.6%, and 26.9%, respectively Table 3. The overall survival rates at 1, 3, and 5 years were 52.8%, 25% and 22.2% Figures 1, and the overall disease-free survival rates at 1, 3, and 5 years were 44.4%, 25%, and 22.2% Figures 2. Patients who had adjuvant radiotherapy had more favorable outcomes than those treated only with surgery.
DISCUSSION
Numerous trials have been conducted for improving the outcome of patients with advanced metastasis to the neck using a variety of multi-modality therapy. 1–4,11,13 Recently, there has been a trend toward neoadjuvant therapy, in particular, definitive chemoradiotherapy and neck dissection as a salvage operation for advanced neck disease. 1,3,4 In order to evaluate this trend, we retrospectively reviewed patients who received definitive treatment for N3 nodal disease. There was a male predominance in this study (93%). A similar male predominance was also reported in other studies. 1 The distribution of primary disease in this study was predominantly oral cavity, hypo-pharynx, and larynx. The incidence of primary disease in the oral cavity was similar to the study reported by Byers et al. 13 The distribution of primary disease and T-stage was also similar to that reported in other studies. 1,11
One fifth of the patients had a neck dissection without adjuvant radiotherapy, largely due to their refusal to have further postoperative treatment and early postoperative mortality. Our complete pathological response rate after preoperative radiotherapy (27.3%) was lower than a study reported by Narayan et al. 11 This was not surprising as Narayan et al 11 included patients with less advanced nodal metastasis (N1, N2, and N3) and reported a 54% complete pathological response rate. Interestingly, Ahmed et al 1 reported a 74% complete pathological response rate in partial responded to cisplatin-based chemoradiotherapy in patients with N3 disease. This seems to be an impressive increase with the addition of chemotherapy to radiotherapy.
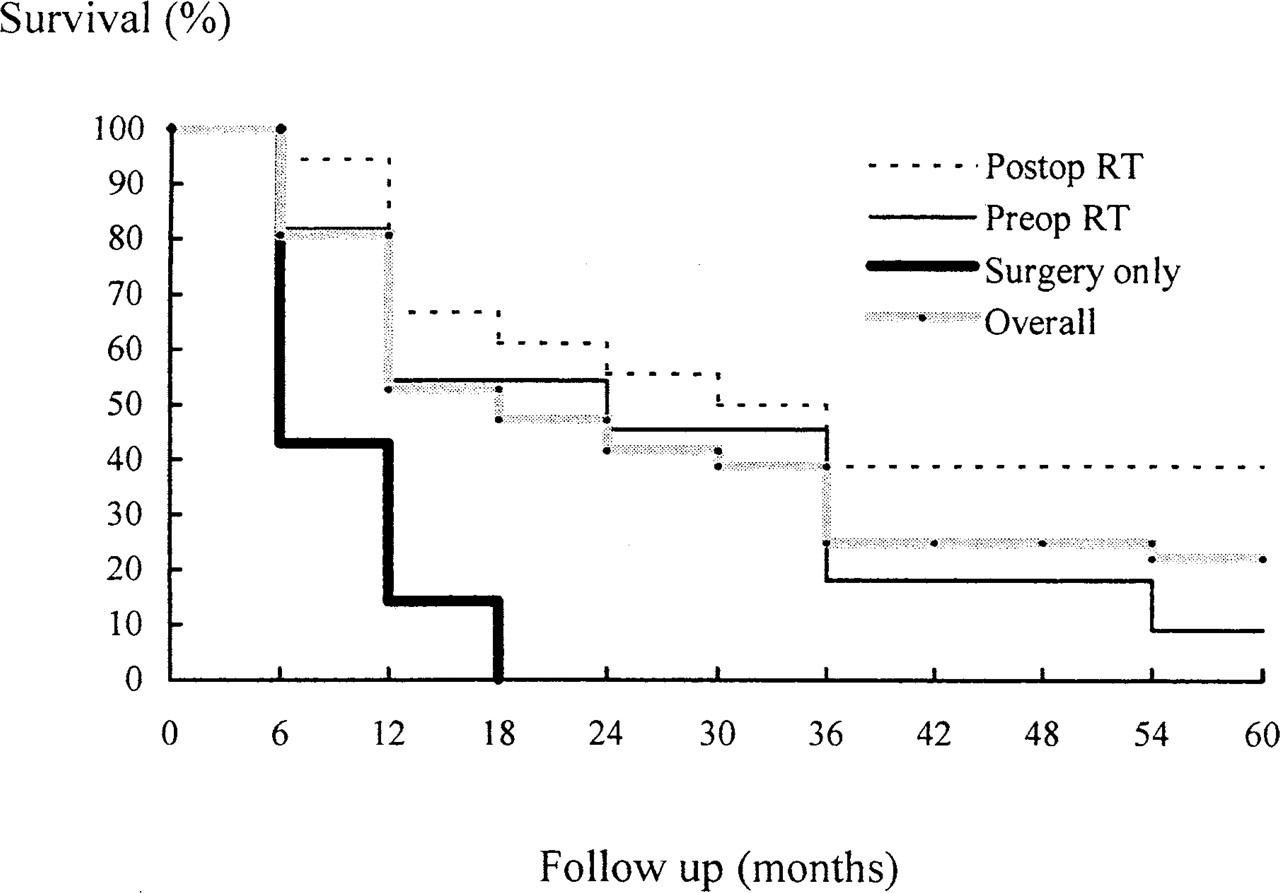
Survival curves.
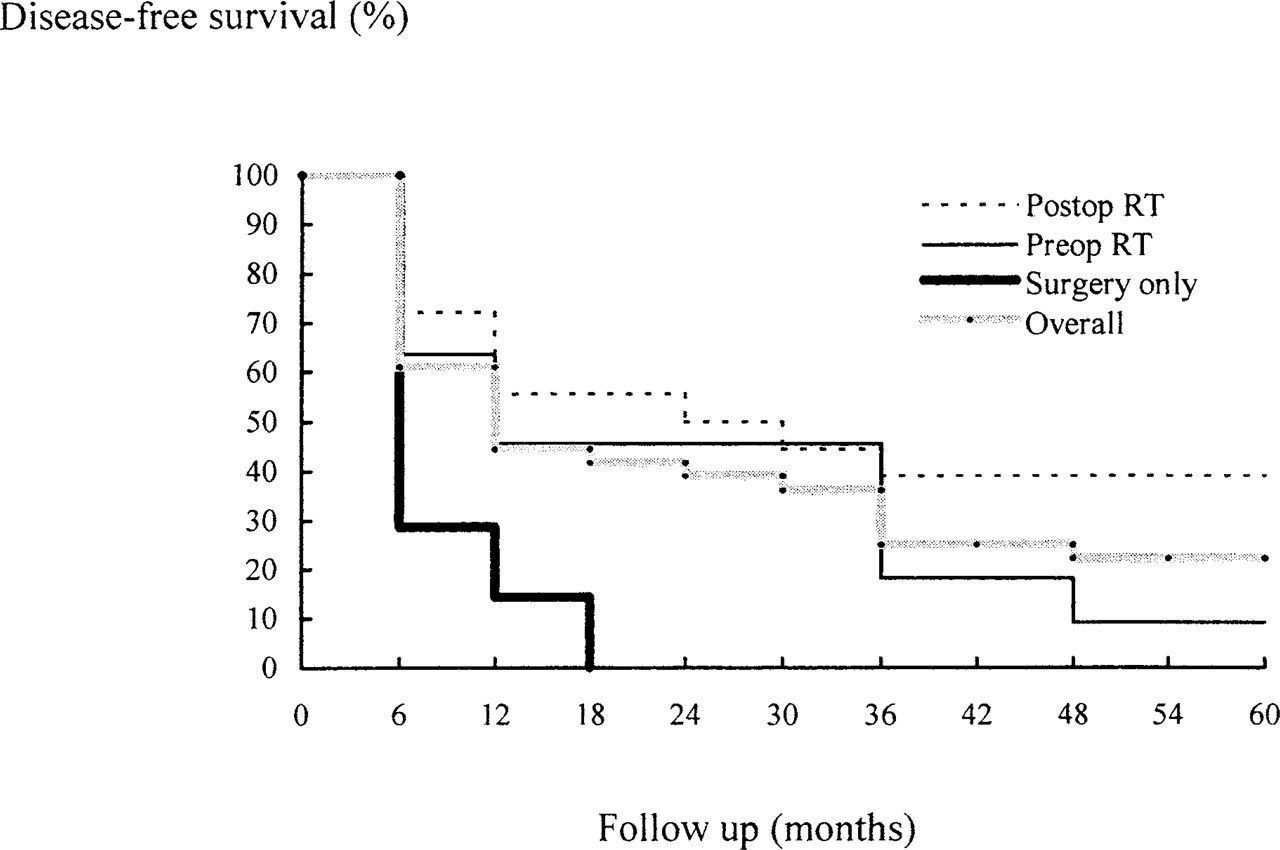
Disease-free survival curves.
Half of the patients in this study had recurrence in the neck, which is comparable to other studies. 3 The overall control rate in the neck in this study was higher for those who had postoperative radiotherapy when compared with those who had preoperative radiotherapy. The poorer overall control rate in the neck after preoperative radiotherapy could be due to the former having more advanced primary disease although one would suspect that the advanced metastasis to the neck would be the main determinant of this and that the primary staging would not impact on control of the neck in N3 disease.
The overall 3- and 5-year survival rate in this study was 25% and 22%, respectively. The 5-year survival rate was higher in the group of patients receiving postoperative radiotherapy. Moe et al 13 reported an overall 5-year survival of 20% in patients with N3 disease in laryngeal carcinoma after postoperative radiotherapy that was only marginally lower than our study.
Ahmed et al 1 reported that an improved outcome with trimodality therapy using concomitant chemoradiotherapy and surgical salvage for N3 nodal disease. Ahmed et al 1 examined the role of intra-arterial cisplatin over 4 weeks with concomitant 68 to 74 Gy radiotherapy over 7 to 8 weeks and surgical salvage in patients with N3 neck disease. Complete clinical response was achieved in 13% and a partial response in 68%. No neck recurrence was reported. The 3-year overall survival rate of 41% was similar to our 3-year survival rates of 38.9% with postoperative radiotherapy. Significantly, in another series, Sanguined et al 3 had a 0% 2-year neck control probability with 60 Gy of radiation alternated with 4 cycles of cisplatin and 5-FU.
Other treatment alternatives included adjuvant radiotherapy or definitive high dose radiotherapy. Byers et al 13 treated 35 patients with N2 and N3 neck disease with definitive postoperative radiotherapy had an 11% local neck failure rate and an overall 5-year survival rate of 55%. Boyd et al 2 achieved a better 1- and 2-year neck control of 100% and 93%, respectively, after planned postradiotherapy neck dissection in 25 patients with N1, N2, and N3 neck disease. However, it is difficult to extrapolate the results of these studies to N3 neck disease.
Bataini et al 15 reported an improved nodal response rate with high dose radiotherapy alone when compared with chemoradiotherapy, which may suggest that radiotherapy may be the more important factor in locoregional control. In another study using high dose definitive radiotherapy, Narayan et al 11 reported a surprisingly high 5-year actuarial in-field neck control of 86% with N3 neck disease.
Based on our results and those of other studies, 2,4,14,15 the combination of radiotherapy and surgery could improve the outcome of advanced neck disease. Indeed, large volume lymph node metastasis is unlikely to be cured by radiotherapy or by chemoradiotherapy alone. 4,5 Wolf et al 4 used induction chemotherapy and definitive radiotherapy for patients with N2 and N3 neck metastasis who responded well to chemotherapy and compared these with conventional treatment of surgery and postoperative radiotherapy. In the former group, a 50% rate of salvage neck dissection was reported. Wolf et al 4 also reported that complete responders had a better survival rate and required less salvage neck dissection and that partial responders had a poorer survival rate with death from uncontrolled neck disease, both in those undergoing salvage dissection and those not undergoing surgery. A 33% complete response rate was reported in those with N3 disease after chemotherapy and radiotherapy. Similar overall survival rates were reported in N2 and N3 diseases in the former group when compared with surgery and postoperative radiotherapy. 4 However, there was no N-stage stratification of results to determine survival or recurrence rates for the N3 disease subgroup. Recondo et al 5 treated 21 patients with N3 disease with neoadjuvant cisplatin, bleomycin, and 5-fluorouracil chemotherapy and reported a complete response rate of only 2% and overall response rate of 12%. In addition, with a median follow-up period of 38 months, their disease-free survival rate was 0%. 5
Although there is increasing enthusiasm for chemoradiation protocols to treat advanced cancer of the head and neck, there are conflicting data about treatment outcomes. 1,3 Potential morbidity is a major concern with many chemoradiation protocols. 6–8 A meta-analysis by Stell and Rawson 9 failed to show any benefit with adjuvant chemotherapy that may in fact increase overall mortality. Another meta-analysis by El-Sayed and Nelson 10 also reported a significantly increased morbidity with the addition of adjuvant chemotherapy but, conversely, an improved chance of local control. Recondo et al 5 reported tolerable and mild chemotoxicity. Insufficient data and the retrospective nature of our study made the assessment of quality of life and treatment morbidity impossible in our series.
We would emphasize that in our series, postoperative radiotherapy had a better outcome compared with preoperative radiotherapy, with better 3- and 5-year disease-free survival and overall survival. The decision to undertake surgery with postoperative radiotherapy or radiotherapy with planned postoperative surgery was not made according to any protocol. We were aware that this was a retrospective nonrandomized study with limitations and potential biases in the selection of patients into each group. Inadequate data recording and patients lost to follow-up are particular limitations of all retrospective studies. Patient numbers were small reflecting the lower incidence of N3 metastasis in the head and neck population, but our numbers were comparable to other N3 series. Based on our findings, postoperative radiotherapy could improve the outcome of patients with N3 nodal metastasis when compared with preoperative radiotherapy. Verschuur et al 16 also reached a similar conclusion. Furthermore, the nonirradiated neck specimen provides accurate and valuable prognostic information while avoiding the potentially higher wound complication rate with surgery after radiotherapy. For example, Narayan et al 11 reported a 17.3% significant complication rate with planned neck dissection after radiotherapy.
In addition, our results suggest that in N3 neck metastasis, neck dissection should be planned regardless of tumor response if radiotherapy is offered preoperatively. This view was shared by Sanguineti et al. 3 Given our results we would also question the increasing trend for chemoradiation as definitive treatment in N3 neck disease. From the 4 patients in this study who received adjuvant chemotherapy with or without radiotherapy (pre-or postoperatively), the results were poor with the longest survival being only 16 months.
In conclusion, N3 nodal metastasis is a very poor prognostic indicator as demonstrated in this study. However, combined modalty treatment offers improved locoregional control as well as an improved survival. The trend toward definitive chemoradiotherapy to treat N3 nodal metastasis needs to be carefully evaluated particularly with respect to the effect on quality of life. Above all, it is not clear that definitive chemoradiotherapy improves locoregional control.
We thank Ms Celene McMullan for her assistance.