
Abstract

CASE REPORT
A 35-year-old woman presented with slowly progressive, nonfluctuating asymmetric hearing loss that had begun 12 years earlier. Audiometric testing revealed profound right-sided sensorineural hearing loss with a speech reception threshold of 95 dB and 0% discrimination. A magnetic resonance image was obtained that showed an incidental Chiari's malformation type I and abnormal enhancement of the labyrinth, which was initially attributed to acute labyrinthitis (Fig 1). She was referred to a neurosurgeon for evaluation of the Chiari's malformation type I and was subsequently lost to follow-up.
The patient re-presented 2 1/2 years later with a report of 5 weeks of intermittent vertigo. Electronystagmography revealed a 100% right reduced vestibular response (RVR) on bithermal testing and a 60% RVR on ice caloric testing. Repeat MRI again revealed hyperintensity on T1-weighted images with enhancement of the right otic capsule, suggestive of a schwannoma. Because of the degree of the symptoms, the patient opted to undergo a transcanal labyrinthectomy. A postauricular incision and wide canalplasty were used for exposure. Intraoperatively, the incus and stapes were removed and the promontory was drilled away. The vestibule and the cochlea were found to be filled with tumor, which was excised completely (Fig 2). The tumor was well circumscribed and exhibited regions of high and low cellularity (Antoni A and B areas, respectively) consistent with schwannoma.
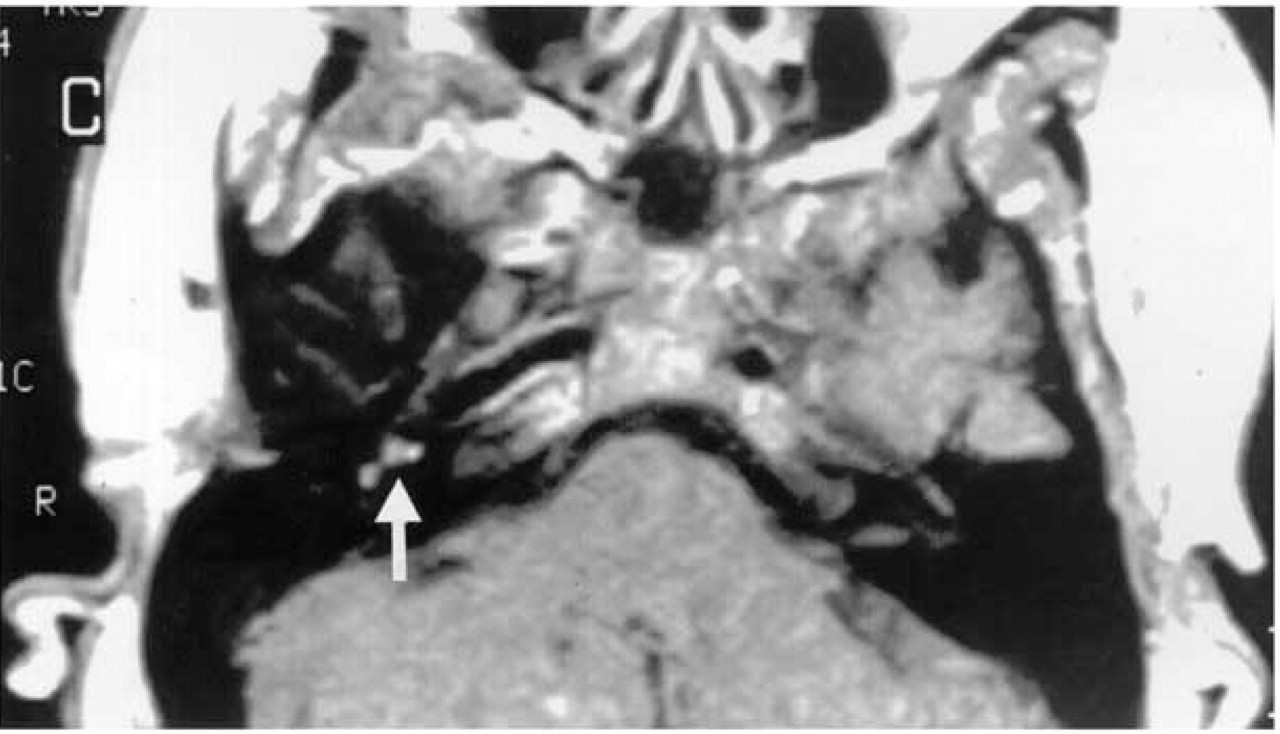
T1-weighted magnetic resonance image demonstrating post-contrast enhancement of the right otic capsule.
DISCUSSION
Historically, IS has typically been diagnosed during otologic surgery (eg, labyrinthectomy and middle ear exploration) or on autopsy, contributing to the relatively low number of reported cases. 2 Since the advent of more sensitive imaging techniques, the frequency of diagnosis has rapidly increased, raising the question of whether IS is a more common condition than currently appreciated.
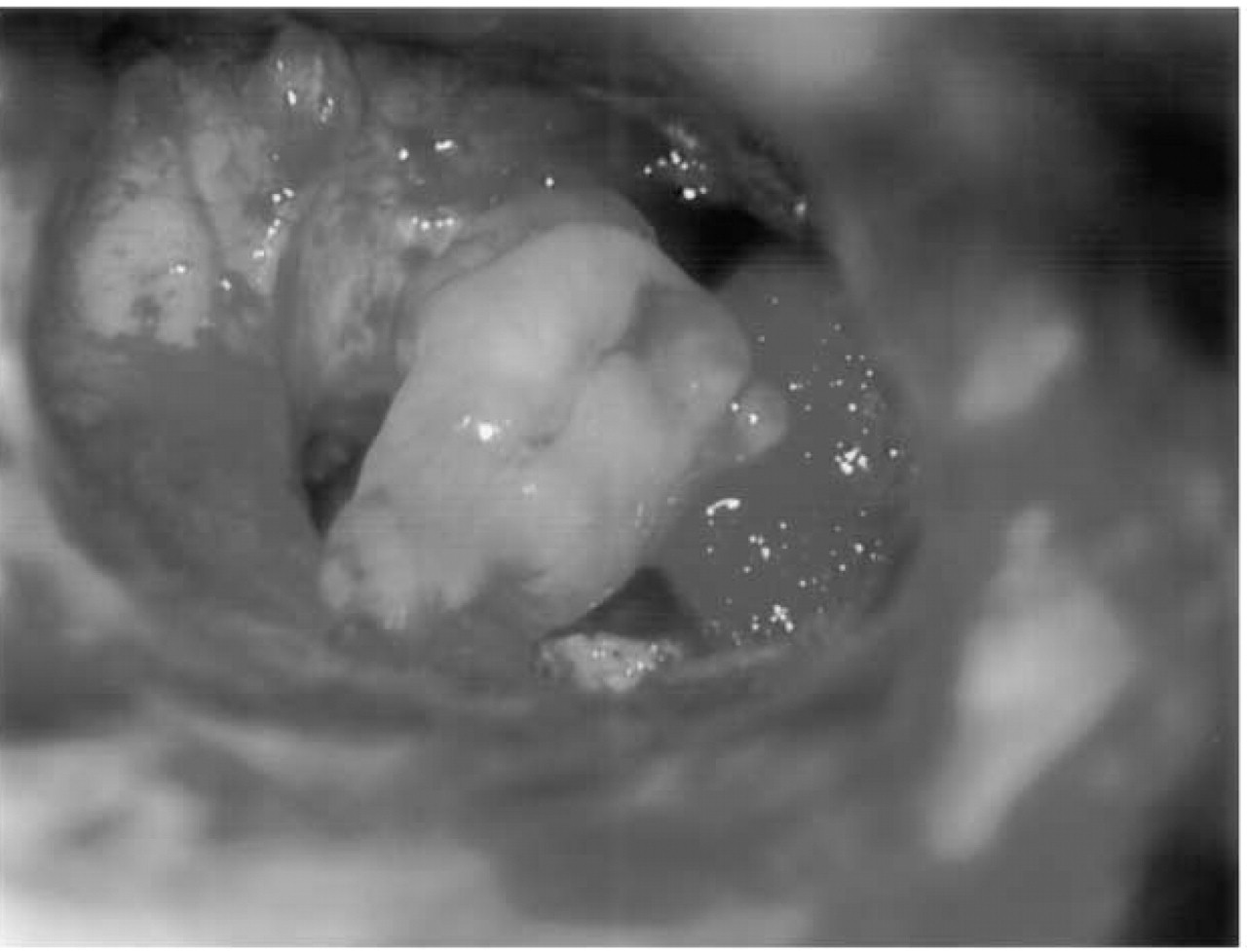
Operative photograph of the tumor being removed from the vestibule and cochlea by a transcanal approach after removal of the incus, stapes, and promontory.
The presenting symptoms of IS include unilateral hearing loss, vertigo, tinnitus, and aural fullness, which occur with variable frequency. Not surprisingly, the diagnosis of Meniere's disease or cochlear hydrops is often given. In a review of the published literature of 22 collective cases, in 1988, Sataloff et al 2 reported sensorineural hearing loss in 19 patients (only 3 were fluctuant) and vertigo in 13 patients. Doyle and Brackmann 1 reported on 8 patients, stating that 7 had hearing loss as their initial report, whereas only 1 presented with vertigo. Three others developed vertigo later in the course of the disease. Fitzgerald et al 3 reported that in 7 patients with IS, all experienced sudden hearing loss as the first noticeable symptom, whereas 4 suffered episodic vertigo that generally was noticed after the hearing loss and resolved well before the time of MRI-confirmed diagnosis. The hearing loss seen in these IS patients was sudden or rapidly progressive, not fluctuating as seen in Meniere's disease. On the basis of the information in these reports, IS generally presents as unilateral sensorineural hearing loss that may or may not be associated with vertigo, which occurs later in the course of the disease when present. Indeed, our patient exhibited progressive unilateral hearing loss, followed by the onset of vertigo more than 2 years after the changes consistent with IS were seen on MRI scans. The nonfluctuant nature of the hearing loss, which well precedes the onset of any associated vertigo, should help in the differentiation among IS and forms of hydropic disease. These symptoms should prompt the clinician to consider additional diagnostic modalities in the form of high-resolution imaging.
Gadolinium-enhanced MRI has greatly improved the ability to diagnose IS. Primary IS appears as a well-defined mass within the cochlea, vestibule, and/or the ampullae of the semicircular canals. It has an intermediate signal on T1-weighted magnetic resonance images, can be missed on T2-weighted images, and demonstrates intense homogenous enhancement on gadolinium-enhanced T1-weighted magnetic resonance images. 4 MRI with gadolinium is now considered the “gold standard” diagnostic test for IS. 5 However, the appearance of IS on magnetic resonance images can be mistaken for other conditions including labyrinthitis, possibly causing a delay in the diagnosis, as observed with our patient.
CONCLUSION
IS exhibits a symptom complex similar to Meniere's disease, but subtle differences such as a lack of fluctuation of a unilateral sudden or progressive sensorineural hearing loss and the delayed onset or complete lack of vertigo should raise the clinical suspicion of IS. When such symptoms are present, prompt gadolinium-enhanced MRI will ensure earlier definitive diagnosis and will help to elucidate an appropriate treatment algorithm for this unusual tumor.