
Abstract
OBJECTIVE: We sought to demonstrate the rate of change in distortion product otoacoustic emission (DPOE) amplitude with age in relation to hearing loss in an unselected adult population.
STUDY DESIGN AND SETTING: We conducted a cross-sectional observation study involving the Framingham Offspring Cohort. Age changes in DPOE amplitude for frequencies of f2 from 1 to 8 kHz adjusted for pure-tone threshold level were assessed by multivariate linear regression.
RESULTS: The women showed a mean hearing threshold-adjusted loss in high-frequency DPOE amplitude of 0.6, 2.1, 2.6, and 1.1 dB/per decade at the f2 frequencies of 1, 2, 4, and 8 kHz, respectively. In contrast, the men showed no effect of age on the DPOE amplitude independent of hearing loss. Emissions were reduced or absent in the noise notch frequencies. The rate of change with age in DPOE amplitude was significantly less than the rate of change in pure-tone thresholds in both the men and the women.
CONCLUSION: Women lose DPOE amplitude from both age and hearing threshold loss. Men lose more DPOE amplitude than do women, and the loss is proportional to the degree of loss of hearing threshold sensitivity. The differential effect whereby age-related hearing loss affects thresholds more than emissions suggests that strial atrophy may be a pathophysiologic factor.
SIGNIFICANCE: The use of DPOE measures for screening and monitoring cochlear status of adult women should take into account the age, pure-tone thresholds, and noise exposure status of the subjects. (Otolaryngol Head Neck Surg 2003;129:382–9.)
Distortion product otoacoustic emissions (DPOEs) are a frequency-specific OAE triggered by stimulating the cochlea with 2 simultaneous pure tones. 2 DPOE testing, in contrast to click-evoked OAE testing, allows assessment of cochlear status at various frequencies (DP-gram) at fixed presentation levels or through frequency-fixed input-output functions at various stimulus levels.
OAEs are generated by the active processes within the cochlea. 8 As such, they have a nonlinear active component that decreases with increasing input and a linear passive component that increases with increasing input. 9 OAEs bear an indirect relationship to hearing threshold sensitivity and may be reduced noticeably before any change in hearing thresholds from, for example, noise exposure is evident. 10 Conversely, with age, behavioral auditory thresholds worsen at a faster rate than does the DPOE input-output function. 11
OAEs are reduced by ototoxic agents known to affect outer hair cell function. Therefore, OAE testing has been proposed as an early detector of ototoxicity from hazardous noise exposure 12 or cis-platinum 13 and aminoglycoside therapy. 14 Although absolute audiometric thresholds cannot be predicted from OAE test results, because of non-linearities and interference from low-frequency noise, changes from baseline appear to be a reliable means of monitoring cochlear function. 15
It is well known that hearing thresholds are poorer in adult men than in adult women and that thresholds worsen with age in both genders. Similarly, DPOE amplitudes have been found to be larger in the young and larger in women than in men. 16 As audiometric thresholds worsen, the amplitude of the DPOE response decreases and ultimately disappears. 17 Reduction in OAEs is known to follow decreased function of the stria vascularis and to follow hair cell loss.
Several groups of investigators have explored the relationship between age and OAE amplitude. Murray and LePage 18 documented an age-related decrease in click-evoked OAE amplitude in a large Australian population ranging in age from birth to 83 years. Many reports indicate that most of these age-related changes are attributable to increases in pure-tone thresholds (PTTs). 19 However, a few reports have noted a small but significant change in DPOE amplitude independent of increasing PTTs. 20,21
The present report describes DPOE amplitude from the DP-gram as a function of age, gender, and presbycusis type in a large adult population in whom presbycusis and noise-induced hearing loss are prevalent. Our long-term goal is to establish a statistical basis for monitoring cochlear function with DPOE in older people. To accomplish this goal, it is important to understand the influences of age, gender, and hearing thresholds on DPOEs. Although DPOEs are well described in normal hearing subjects and in clinical populations with hearing loss, there is a lack of population-based data on which to delineate the separate effect of age on this unique property of the cochlea.
METHODS
Subjects
The subjects were volunteer members of the Framingham Offspring cohort tested during Offspring Examination 6, which was conducted in 1995 through 1999. This cohort consists of the children of the original Framingham Heart Study cohort and their spouses. As such, this is not a random population sample, although the group is representative of the original cohort, which was largely of western and central European background. 22 Because the reflectance measures were made separately from the routine audiometry, not all potential subjects were able to return to the study center on another day due to timing or travel considerations. Five subjects were excluded because of abnormal tympanometric findings.
Specific Auditory Test Procedures
Behavioral Tests.
PTTs at 0.5, 1, 2, 4, 6, and 8 kHz were obtained by the standard Hughson-Westlake method using spaces and equipment that meet ANSI standards. Speech reception thresholds were obtained as a reliability check against the PTT procedures.
Tympanometry.
Tympanometry was performed using a Grason-Stadler model 37 device. The probe tone was 226 Hz, and pressures ranged from −400 to +200 daPA. Ears with a flat tympanogram (possible fluid) were excluded. Two ears were excluded for tympanogram gradients less than.25; and 3 ears were excluded due to pressures of less than −200 daPA. There were no exclusions based on low compliance (cutoff of 0.3) or large volume.
DPOE.
Because of limited test time, only one ear of each subject was tested; the test ear was selected randomly. DPOEs were measured using the EMAV software developed at Boys Town National Research Hospital with a custom system consisting of an Ariel DSP board and an ER-10C microphone. The so-called DP-gram was obtained at presentation levels of L1 of 65 dB and L2 of 50 dB SPL, using a f2/f1 ratio of 1.22 with f2 frequencies of 0.5, 0.75, 1, 1.5, 2, 3, 4, 6, and 8 kHz. The subjects were also tested with L1 of 75 and L2 of 65 dB SPL using the same f2/f1 ratio and frequencies. The latter data are not included in this report as they paralleled the findings at the lower stimulus levels but with greater variance.
The amplitude of the DPOE responses in relation to the noise floor was noted for each of the 9 test frequencies; those with a 3-dB signal-to-noise ratio were accepted as valid DPOEs. The proportion of valid DPOEs was 0.29, 0.76, 0.93, 0.95, and 0.83 at f2s of 0.5, 1, 2, 4, and 8 kHz respectively. Therefore only data from the test frequencies of 1–8 kHz are included in this report.
Noise Notch Identification.
Because of the deleterious effect of noise on DPOE, each subject's audiogram was characterized as showing a “noise” notch using an automated method that has been described previously. 23 Each audiogram was characterized as to the presence of a notch at 4 to 6 kHz and, further, the notch was quantified according to depth of the notch (in dB). Notches were categorized as being absent (N0, depth of 15 dB or less), mild (N1, depth of 16 to 35 dB), and severe (N2, depth of >35 dB). Preliminary analysis of variance (data not shown) indicated that the DPOE thresholds at 2, 4, and 6 kHz were significantly poorer in those 40 cases (1 woman, 39 men) with a deep notch (N2). Therefore, the DPOE data at 2, 4, and 6 kHz were omitted for these 40 cases in the age analyses.
Statistical Analysis.
Analyses were done with STATA (version 7.0). Output from this package was exported into Microsoft Excel and SPLUS for graphical display. The data were first summarized and examined for outliers and consistency. Univariate analyses were done separately for men and women using DPOE amplitude as the dependent variable and age as the independent (predictor) variable. Multivariate linear regression was then done separately for the men and the women by adding PTT as a second predictor variable and the interaction term (ie, PTT X age). Because there were no significant interactions between the predictor variables, the interaction term was dropped from the final model. The final regression model can then be written as:

The DPOE amplitudes were normally distributed for frequencies up to f2 = 4 kHz. At frequencies above 4 kHz, the data were significantly skewed toward lower amplitudes. These deviations, however, were minor at all frequencies, and the diagnostic tests for normalcy and heterogeneity after regression were satisfactory.
To describe the frequency specificity of the DPOE, each test DPOE frequency was analyzed separately in relation the corresponding audiometric test frequency. A value of P < 0.05 was set as the level of statistical significance.
Gender and age
The standardized slopes of the rate of change of DPOE with age were directly compared with the standardized slopes of the rate of change of PTT for each of the test frequencies separately for men and women using the “corcor” command in STATA.
RESULTS
Descriptive Statistics
Table 1 shows the demographic characteristics of the subjects. Two hundred seventy-seven women and 209 men had audiometric and DPOE test results (total, 486). The mean age of the women was 59.3 ± 9.6 years (range, 31 to 80 years), and the mean age of the men was 57.8 ± 9.2 years (range, 36 to 82 years); the age difference was not significant (t = 1.83, P = 0.068).
Table 2 shows the mean PTTs and mean DPOE amplitudes across the audiometric test frequencies. Forty-four percent of the subjects (53% of the women, 33% of the men) had normal PTTs (ie, ≤25 dB) at all audiometric test frequencies and 25% had normal thresholds except for 8 kHz. Men had significantly poorer mean PTTs than the women at 4 kHz and above and significantly lower mean DPOE amplitudes than the women. The gender difference in DPOE amplitude at 4 kHz and above remained significant even when the noise notch cases were excluded.
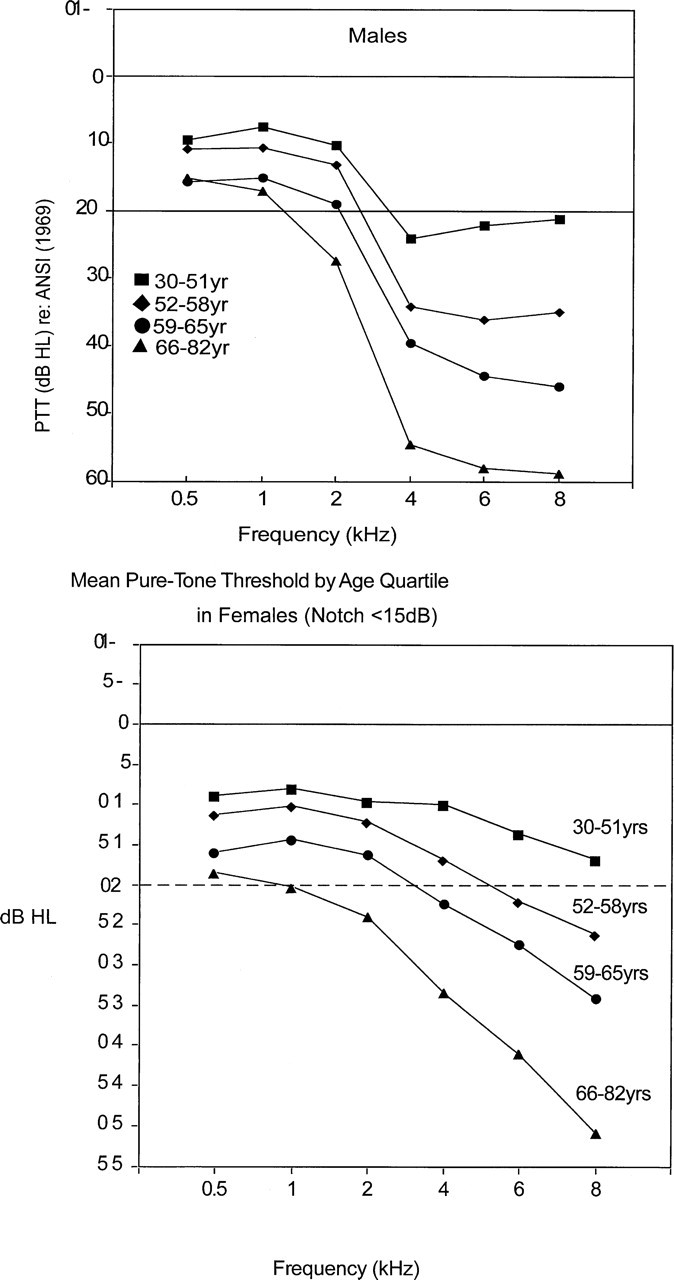
Figure 1 displays the change in PTTs and DPOE for the women and men by age group. For this display, the subjects were divided into 4 equal frequency groups based on age. There is a clear worsening of thresholds and DPOE amplitude for both genders across the age groups.
Effect of Age on DPOE and Hearing Thresholds
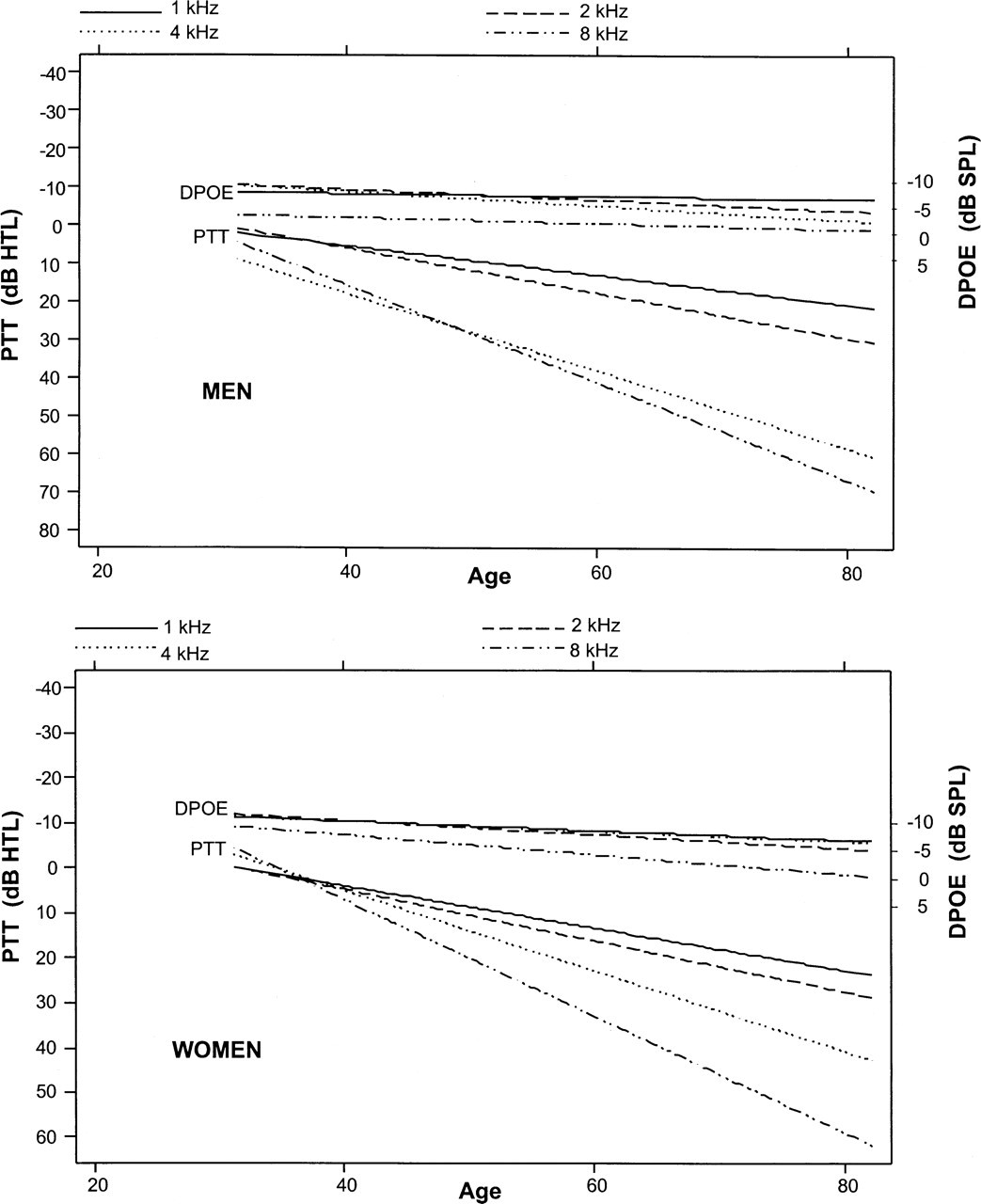
The slopes of the mean rates of change with age in the DPOE amplitudes and PTTs are displayed separately for the men and women in Figure 2. These slopes represent the ordinary least-squares mean for each age level. As expected, the slopes of the pure-tone—age functions increased with increasing frequency. In contrast, the slopes of the DPOE age functions varied only slightly by frequency and the rate of change with age was much less. The rate of change with age in the DPOE amplitudes was compared with the rate of change with age in PTTs separately for men and women using standardized values for each variable. The rate of change of DPOE was significantly less than the rate of change in PTTs at all frequencies. These differences were highly significant (P < 0.001) for all comparisons by frequency within each gender group.
Mean pure-tone and DPOE thresholds by gender and frequency
Multivariate regressions of DPOE amplitude on age adjusted for hearing threshold level were done at each frequency separately for each gender group. There was no effect of age on DPOE amplitude at any test frequency for the men; the decline in DPOE amplitude was attributable to the worsening auditory thresholds. The effect of age was significant for the women at 2 to 8 kHz but not for 1 kHz. The rate of decrease in DPOE amplitude adjusted for hearing level in the women was frequency dependent and ranged between 1.0 and 2.0 dB/decade. Table 3 displays the slope coefficient (β) for each of these multivariate regressions.
DISCUSSION
Measurement of OAEs has provided new insights into cochlear function. OAEs provide indirect evidence of outer hair cell function. However, because of redundancy and compensatory mechanisms, there is not a linear relation of DPOE measures to auditory thresholds. Nonetheless, OAE measurements have an emerging place in the clinical auditory evaluation, a place that is likely to expand as refinements in technique occur.
In this report, we have shown, as have others, 24 that DPOE amplitude, as an objective measure of cochlear function, parallels the decline in high-frequency hearing sensitivity with age in both men and women. Of note, the rate of decline of DPOE amplitude with age was less than the decline in PTTs in both gender groups, which suggests a differential mechanism. 25
In women, age and hearing threshold appear to affect high-frequency DPOE amplitude independently, whereas in men all of the decline in DPOE amplitude was attributable to decline in hearing thresholds at each test frequency. This observation suggests the propriety of an age correction as a normative reference in DPOE testing in women.
We surmised that the difference between genders in the rate of decline of high-frequency DPOE amplitude with age may be due to the effect of extrinsic factors in the men and of genetic factors in the women. This supposition is logical because we have shown previously in this cohort that noise exposure and noise-induced hearing loss were very prevalent in the men 23 and, in addition, that inheritability of age-related hearing loss is high, particularly in women with strial presbycusis. 26 However, the gender difference in the rate of decline of DPOE amplitude persisted in the range of 4 to 8 kHz even in subjects with no noise notches. Therefore, other sources of variance in men's hearing should be explored in future studies. The design of the present study does not permit an analysis by family groups to address the effect of inheritability.
Men, having larger ear canals, may have smaller emissions than women as a function of ear canal volume. In other words, the same acoustic energy dispersed in a larger volume produces a smaller pressure displacement at the recording microphone. However, this factor would not account for the difference in change in emission amplitude with age across the 2 gender groups; therefore, other factors should be considered.
(
(
Slope (β coefficients) and significance (P values) at 1, 2, 4, and 8 kHz for men and women
The observed decline with age supports the concept that emissions, being the result of a nonlinear process within the cochlea, also have nonlinear test attributes. Emissions are thought to be due to basilar membrane disturbances brought about by outer hair cell contraction in response to specific tones. These contractions are in turn held to be the mechanism whereby the cochlea “amplifies” low-intensity tones to facilitate their detection. It appears that emissions, which are known to be very robust in the infant, have considerable reserve and redundancy such that a considerable drop in emission level may occur before there is a notable effect on auditory threshold sensitivity.
The criterion for “acceptance” of a signal as an emission is arbitrary. We used a signal 3 dB above the noise floor as a conservative estimate of the presence of an emission. We also compared criteria of 0 dB and 6 dB in trial analyses and found the major conclusions of the analyses to remain the same (results not shown). We judged 3 dB as an effective criterion because it optimizes the number of analyzable emissions high without increasing skewness that occurs when no criterion is used.
The above data are derived from the DP-gram, in which the DPOEs are elicited at various frequencies at a constant intensity level. An alternative way of administering the DPOE test, is to vary the intensity one frequency at a time, the so-called input-output function of DPOE. We have shown previously that the area under the input-output function of DPOE amplitude changes with age at a lower rate than does the PTT and that this finding was the same for the men and the women. 11 Because DPOE amplitude does not rise linearly with stimulus intensity, the use of multiple stimulus levels appears to be a more robust technique than the single intensity level used in the DP-gram. The input-output function, which takes longer to perform than the single intensity sweep, is not as suitable for infant screening, for example, but may be a more reliable clinical method than the DP-gram. However, these considerations are speculative at the present.
Although the large population tested was not selected except through volunteerism and availability, the results may be generalizable to other people of similar ages, noise-exposure history, and background. These data were derived from a single cross-sectional examination of the subjects in which differences in age groups are summarized. A stronger method to assess aging is to conduct a longitudinal study wherein changes with time are assessed for each individual subject and then summarized. We will make these data available to future hearing researchers who might have the opportunity to retest these subjects.
SUMMARY
1) In women, there is a frequency-dependent loss of DPOE amplitude of about 1 to 2 dB/decade in the 1- to 6-kHz frequencies over the ages of 31 to 80 years that is independent of the age-related loss in hearing threshold. 2) In males, the decline in DPOE amplitude was attributable only to elevation of the PTTs. 3) DPOE amplitude was lower after adjustment for PTT loss in the presbycusis group than in the normal hearing group. 4) The rate of change of PTT with age is greater than the rate of change of DPOE amplitude with age. This suggests that factors other than hair cell loss (eg, strial atrophy) may account for early presbycusis. 5) The results of DPOE testing should take into account gender, age, hearing threshold, and presbycusis type.
Dean Billheimmer, PhD, provided statistical assistance. Michael Gorga, PhD, provided helpful comments. Aimee Verrall performed the data management and assisted in manuscript preparation.