
Abstract
OBJECTIVE: We sought to demonstrate the feasibility of using iontophoresis to deliver pharmaceutical agents into the middle and inner ear for the treatment of middle and inner ear diseases, which is proved in this study by the successful iontophoresis of the ferromagnetic contrast agent gadopentetate dimeglumine.
STUDY DESIGN AND SETTING: Eight rabbits were iontophoresed using gadopentetate dimeglumine solution 469 mg/mL. Then, all rabbits underwent magnetic resonance imaging for the detection of gadopentetate dimeglumine in the middle and inner ear structures. The study was conducted in the tertiary referral center the University Hospital of Crete.
RESULTS: The high signal intensity of the gadopentetate dimeglumine solution was demonstrated within the middle ear cavity and inner ear structures of all iontophoresed ears and in none of the non-iontophoresed ones.
CONCLUSIONS: Transtympanic iontophoresis could be an effective method for the passage of pharmaceutical agents into the middle and inner ear for the treatment of middle and inner ear diseases. (Otolaryngol Head Neck Surg 2003;129:408–13.)
Sato et al 2 used iontophoresis of an anti-inflammatory agent (corticosteroid) and antibiotic for the treatment of otitis media with effusion in children, and their results showed that this treatment was useful in controlling the inflammation and infection in the middle ear that are considered to be important pathogenetic factors.
Gillespie et al 3 iontophoresed with lidocaine 8 rabbits, followed by diagnostic vestibulotomies. Significant amounts of perilymph lidocaine were found in both the intact and perforated tympanic membrane groups. In the perforated tympanic membrane group, the perilymph lidocaine level was 8 times that of the intact tympanic membrane group.
Iontophoresis has been also used to introduce lidocaine ions into the inner ear for the treatment of tinnitus. 4 The initial results indicated that approximately 60% of patients reported a reduction in tinnitus intensity. 5 Succeeding studies demonstrated that a few patients experienced slight improvement, although the tinnitus persisted in its annoyance and the majority did not notice any difference in their tinnitus during and/or after treatment. 6,7
In the present study, we sought to demonstrate the middle ear cavity and the inner ear structures by means of transtympanic iontophoresis of the ferromagnetic contrast agent gadopentetate dimeglumine.
MATERIALS AND METHODS
After the approval of the University Hospital of Crete animal review committee, 8 rabbits, weighing 1.4 to 1.8 kg, were anesthetized with subcutaneous injection of ketamine HCl 30 mg/kg and promazine HCl 50 mg/kg. All external auditory canals were thoroughly cleaned for better visualization and then filled with the iontophoretic solution. All tympanic membranes were intact. One ear of each rabbit was used for the iontophoresis, and the other was used as a control. We used an iontophoretic applicator (Iontophor-PM model 6111; Life-Tech, Inc, Stafford, TX).
The ferromagnetic contrast agent used was gadopentetate dimeglumine solution 469 mg/mL. The signal intensity of the undiluted contrast agent is low on T1-weighted images used in this study and thus not appropriate for our application. Twelve different dilutions of contrast agent with normal saline were tested to select the one rendering the highest signal intensity on the T1-weighted image parameters used in the present study. The different dilutions within 12 vials were positioned in the magnet. The highest signal was shown by dilution of 6 mL in 1000 mL of normal saline (ie, 2.81 mg/mL), and this dilution was used in the present study.
The 8 rabbits were randomly divided into 2 groups of 4 rabbits each. One external auditory canal of each rabbit was filled with the final dilution of gadopentetate dimeglumine. The anode (positive electrode) was placed into the external auditory canal, coming into contact with the dilution of gadopentetate dimeglumine and without touching the skin, and the cathode (negative electrode) was placed in the contralateral area of the neck. In the first group the direct current (1 mA) was applied for 15 minutes, whereas in the second group the direct current (1 mA) was applied for 20 minutes. The contralateral (control) ear of each rabbit remained filled with the final dilution of gadopentetate dimeglumine, for the same time, without being iontophoresed. At the end of the procedure, all external auditory canals were irrigated with 50 mL normal saline to wash out the solution, and the rabbits underwent magnetic resonance imaging (MRI).
The 8 rabbits were scanned using a 1.5-T whole body superconducting imager (MAGNETOM Vision Plus, Siemens). Standard quadrature radiofrequency (RF) body coil (64-cm diameter) was used for signal excitation, and a small circular loop RF coil (3 cm diameter) operating only as receiver was used for signal detection. Appropriate coil loading for RF transmission was ensured for body coil in each experiment using a Plexiglas tube (body coil phantom loader) filled with conductive paramagnetic solution and positioned around each rabbit.
During the experiment, the rabbits were placed in the prone position with their longest anatomic axis (head-feet axis) parallel to the magnet's principal axis and their heads overextending toward the coronal plane. A small circular loop coil was positioned above the rabbit's head with its principal axis parallel to rabbit's transverse anatomic direction. Using this configuration, axial T1-weighted images were obtained to demonstrate the overall anatomy using a single-echo multislice gradient echo (GE) 2-dimensional flash sequence (TR, 15 milliseconds; TE, 6 milliseconds; flip angle, 70°; 5 slices; slice thickness, 8 mm; inter-slice gap, 2 mm; field-of-view [FOV], 150 × 150 mm2; reconstruction matrix, 128 × 256 pixels; and 1 excitation).
Consequently, 3 series of images were acquired, with each depicting different details of the anatomic structures. The first series of images consisted of 9 coronal 2-mm slices obtained using a T1-weighted single-echo multislice spin echo (SE) 2-dimensional standard sequence (TR, 400 milliseconds; TE, 14 milliseconds; flip angle, 90°). Slices were almost parallel to rabbit's external ear canals, thus depicting anatomy of outer, middle, and inner ear structures. Gradient strength used in this sequence (23 mT/m) was compromising for a thin slice (2 mm) and a rectangular FOV (RFOV) covering an area of 53 × 70 mm2. The image reconstruction matrix was 192 × 256 pixels, respectively, to the RFOV dimensions, compromising for a pixel matrix dimensions of 0.27 × 0.27 mm. Two signal averages (excitations) and a small receiver bandwidth (89 Hz/pixel) were used to improve the signal-to-noise ratio.
The second and third series of images comprised 2-mm axial and axial oblique T1-weighted images obtained using the previously described single-echo multislice SE sequence applied at planes vertical to rabbit's external ear and along the inner auditory canal of the ear undergoing iontophoresis, respectively.
RESULTS
The high signal of the gadopentetate dimeglumine solution was recognized in the middle ear cavity of the 8 iontophoresed ears (Fig 1). The contralateral middle ear cavities showed signal void consistent with the presence of air (Fig 1). There was no appreciable difference in signal intensity within the middle ear cavity between the 2 groups of iontophoresed ears, namely those undergoing iontophoresis for 15 and 20 minutes, respectively.
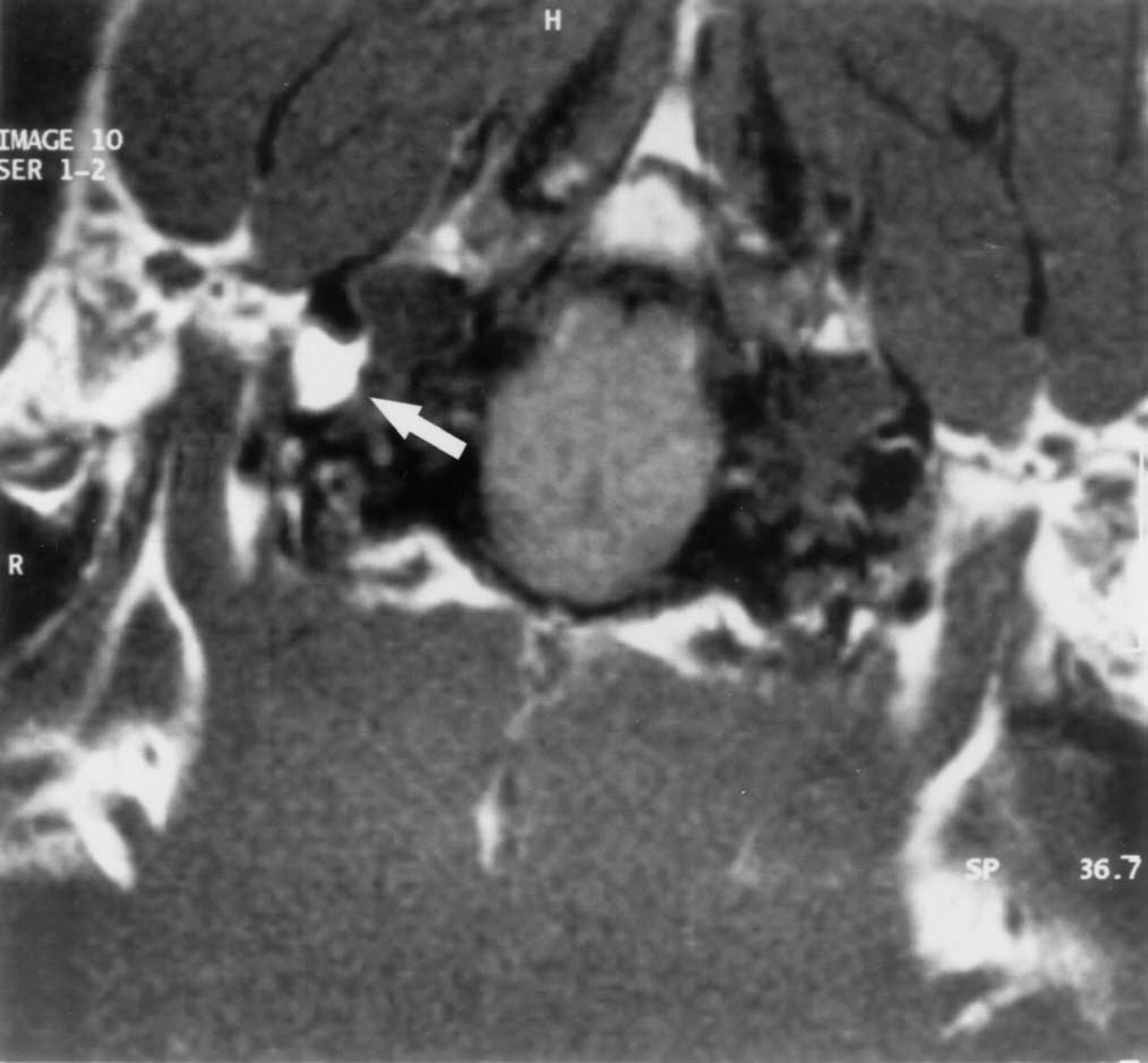
T1-weighted (TR, 400.0; TE, 14.0/1) coronal MR image with 2-mm slice thickness. High signal intensity fluid in the middle ear cavity of the right iontophoresed ear. The contralateral middle ear cavity shows low signal due to the presence of air.
The vestibule and at least 1 semicircular canal of all iontophoresed ears were filled with the high signal solution of gadopentetate dimeglumine (Fig 2), whereas the control ears did not show high signal in the inner ear. The signal intensity did not present any appreciable difference in the inner ears of the 2 groups of iontophoresed ears or between the vestibules and the middle ear cavities of iontophoresed ears.
The high signal intensity of the contrast agent was demonstrated within the middle ear cavity and inner ear structures of all iontophoresed ears and in none of the noniontophoresed ones. This high signal intensity, apart from contrast media, can be rendered by fatty tissue or blood on T1-weighted images. However, inspection of tympanic membrane with a surgical microscope did not reveal the presence of blood.
DISCUSSION
Iontophoresis was introduced as early as the 1740s by Pivati to treat arthritis. 8,9 Not until 1879, however, did Munch truly demonstrate the ability to deliver ions, by delivering strychnine into a rabbit with an electric current. 8 LeDuc 10 performed the first scientific experiments relating to the mechanism of iontophoresis in 1908. Using 2 rabbits placed in series, he introduced strychnine into one and cyanide into other, each depending to the polarity. He was able to determine which ions were introduced by observing the signs preceding death.
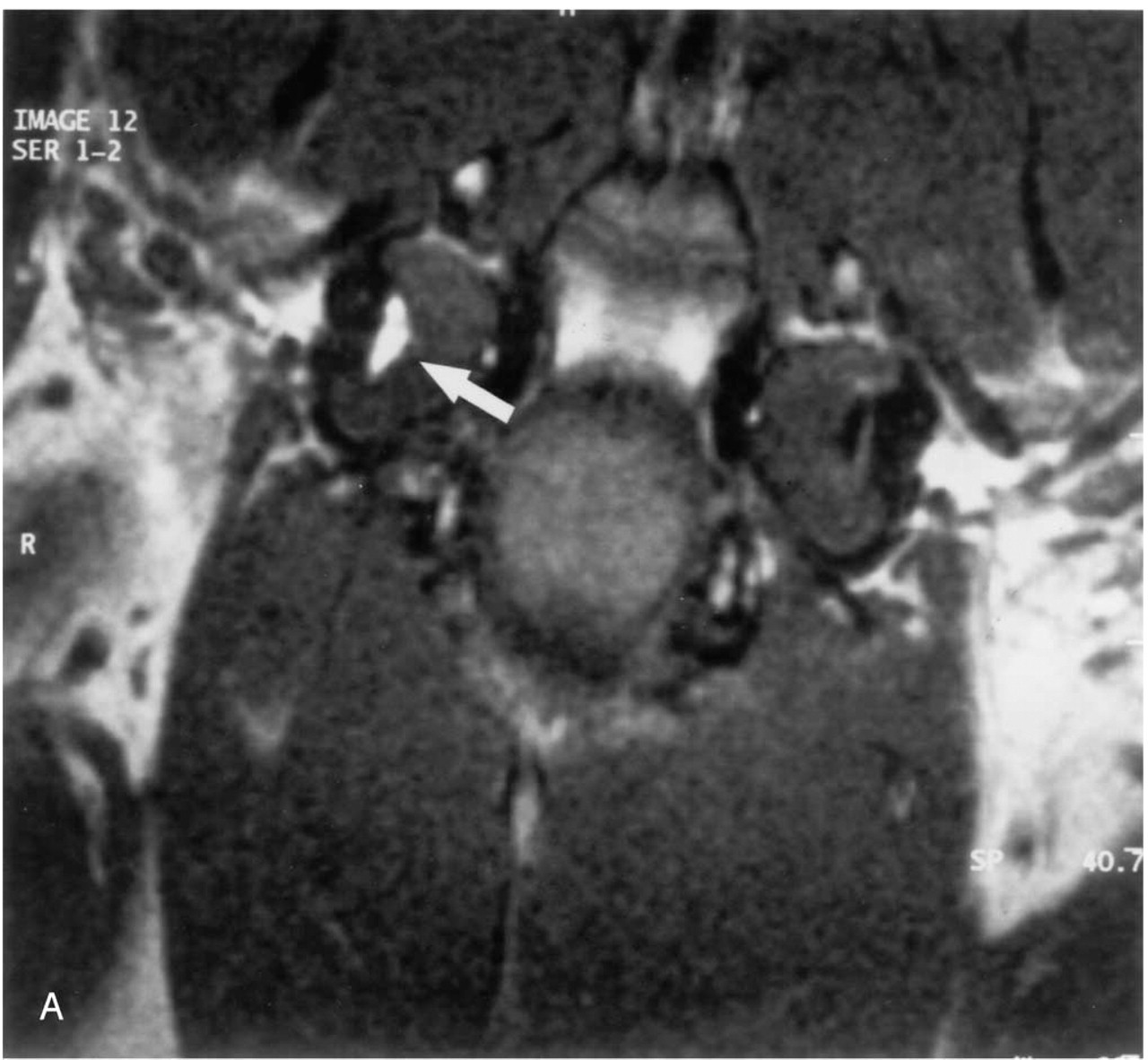
T1-weighted (TR, 400.0; TE, 14.0/1) coronal

Continued.
In summary, the increased penetration across a membrane of an ionic species under the applied electric field can, thus, be due to (1) the electrochemical potential gradient across the membrane, (2) the increased membrane permeability under applied electric field, and (3) the current-induced water transport effect (electro-osmosis or convective transport or iontohydrokinesis). Iontohydrokinesis is another primary means by which ions and other substances, such proteins and peptides, traverse a membrane. 11
According to Chien et al, 12 there are several advantages of an effective, controlled percutaneous drug delivery system such as iontophoresis: (1) it avoids the risks and inconveniences of parenteral (injection/intravenous) therapy; (2) it prevents the variation in the absorption and metabolism seen with oral administration; (3) it increases therapeutic efficacy by bypassing hepatic “first-pass” elimination—the reduction in the amount of the drug entering the systemic circulation due to metabolism by the liver as the drug passes through the hepatic circulation after absorption from the gastrointestinal tract; (4) it reduces the chance of overdosing or underdosing by providing continuous delivery of the drug, programmed at the required therapeutic rate; (5) it permits the use of a drug with short biologic half-life because the drug is delivered directly to the target organ without the need to circulate and recirculate in the blood or the drug flows directly into the bloodstream without delays due to absorption through the gastrointestinal tract; (6) it provides a simplified therapeutic regiment, leading to better patient compliance; and (7) it permits a rapid termination of medication administration, if needed, by simply turning off the iontophoretic delivery system.
In the present study, by means of transtympanic iontophoresis of the ferromagnetic contrast agent gadopentetate dimeglumine, we achieved introduction of the contrast agent in the middle ear cavity and the inner ear structures. For the first time using radiographic evidence, the results of previous studies suggesting that transtympanic passage of pharmaceutical agents in the middle ear cavity and inner ear is feasible were confirmed. The high signal intensity of the contrast agent was demonstrated within the middle ear cavity and inner ear structures of all iontophoresed ears and in none of the noniontophoresed ones. This high signal intensity, apart from contrast media, can be rendered by fatty tissue or blood on T1-weighted images. However, inspection of tympanic membrane with a surgical microscope did not reveal the presence of blood.
Delineation of middle ear cavity, vestibule, and semicircular canals by contrast agent after iontophoresis may be helpful in MRI of the temporal bone in humans. Regularly, these spaces are of low signal on T1-weighted images. By filling these spaces with contrast media, one could expect better delineation of the anatomy and demonstration of anatomic details, in a manner similar to MR arthrography. Additionally, the high contrast between the high signal fluid within the middle and inner ear structures and the low signal walls of cavities and surrounding elements of temporal bones can provide the ideal basis for the application of virtual endoscopy in the middle and inner ear on MRI.
Possible clinical applications that we have started to work on, based on the results of the present study, are to use transtympanic iontophoresis of gentamicin for the treatment of Ménière's disease and corticosteroids for the management of sudden hearing loss and autoimmune inner ear diseases.
Schuknecht 13 first introduced the intratympanic injection of gentamicin in 1957. The technique has evolved with a trend toward lower doses and greater time intervals between doses. 14 A wide variety of techniques with intratympanic gentamicin is successfully used in treating Ménière's disease. 15-17 Proposed treatment procedures have included the placement of polyethylene tubes or catheters, hospitalization, and repeated injections until evidence of vestibular toxicity is manifested. 18 No particular method can be recommended as the most effective based on the literature, and iontophoresis could be a good alternative technique for this application. Medical and nonmedical factors such as patient safety, patient convenience, less atraumatic technique, and cost may play a role in selection of the technique used. 19
In a recent report, Parnes et al 20 investigated the effects of intratympanic injection of corticosteroids for the treatment of hearing loss in inner ear disorders. They established cochlear fluid pharmacokinetic profiles of hydrocortisone, methylprednisolone, and dexamethasone in the guinea pig after oral, intravenous, and topical (intratympanic) administration. Their findings demonstrated a much higher penetration of all 3 drugs into the cochlear fluids after topical (intratympanic) application compared with systemic administration. They managed to treat sudden deafness, autoimmune inner ear disease, and Cogan's syndrome through the injection of intratympanic corticosteroids. We assume that iontophoresis, being less traumatic and easy to be performed, might be used for these applications.
Transtympanic iontophoresis could be an effective method for the passage of pharmaceutical agents into the middle and inner ear for the treatment of middle and inner ear diseases. It is a noninvasive method of low cost, which does not seem to compromise patient safety or convenience.