
Abstract
OBJECTIVE: We sought to reintroduce a historical procedure—intracapsular tonsillar reduction (partial tonsillectomy or tonsillotomy)—for tonsillar hypertrophy causing obstructive sleep disordered breathing (OSDB) in children, as well as to determine whether partial tonsillectomy, compared with conventional (total) tonsillectomy when performed by more than one surgeon, is equally effective for the relief of OSDB while resulting in less pain and more rapid recovery.
STUDY DESIGN: We conducted a retrospective case series at a tertiary children's hospital. The charts of children who underwent partial tonsillectomy and total tonsillectomy (1998 through 2002) for postoperative complications were reviewed. The caregivers were surveyed to assess postoperative pain, rapidity of recovery, and effectiveness of surgery for relieving symptoms of OSDB.
RESULTS: Two hundred forty-three children underwent partial tonsillectomy and 107 children underwent total tonsillectomy. There were no significant differences in immediate and delayed complications between the groups. Both operations were equally effective in relieving OSDB. Children who had partial tonsillectomy had significantly less postoperative pain and significantly more rapid recovery.
CONCLUSION: Intracapsular tonsillar reduction with an endoscopic microdebrider relieves OSDB as effectively as conventional tonsillectomy, but results in less postoperative pain and a more rapid recovery.
In a search for a less invasive but equally effective technique, we revisited an old procedure—tonsillotomy, or partial tonsillectomy, but performed with contemporary technology. We perform a purposeful reduction in the tonsil size, partially shaving them away using an endoscopic microdebrider. 1 The goal of this procedure is to eliminate the obstructive portion of the tonsil while preserving the tonsillar capsule. By maintaining the integrity of the capsule, a natural biologic dressing is left in place over the pharyngeal muscles, preventing them from sustaining injury, inflammation, and infection. This results in less postoperative pain, a more rapid recovery, and perhaps fewer delayed complications. 1
The goal of this study was to demonstrate the historical context of our procedure and to assess whether partial tonsillectomy compared to (total) conventional tonsillectomy, when performed by several surgeons in a larger cohort of patients, is equally effective for the relief of OSDB while resulting in less pain and a more rapid recovery.
PATIENTS AND METHODS
Patients
We reviewed the outpatient and inpatient medical records of all children (n = 243, partial tonsillectomy group) who underwent intracapsular tonsillectomy for tonsillar hypertrophy causing OSDB performed by 1 of 3 surgeons (P.J.K., K.H., or T.I.A.) at the Children's Hospital at the Cleveland Clinic between October 1998 and June 2002. The diagnosis of OSDB was based on the history provided by the child's caregiver (snoring, gasping, apnea, restless sleep, frequent awakenings, bet wetting, and daytime somnolence). For comparison, we reviewed the outpatient and inpatient records of all children (n = 107, total tonsillectomy group) who underwent standard tonsillectomy for tonsillar hypertrophy causing OSDB (ascertained by history) performed by the same surgeons during the same period at the same hospital. We also conducted a telephone survey of the primary caregivers of the children (211 [87% of caregivers] in the partial tonsillectomy group 1 and 90 [84%] in the total tonsillectomy group) by using a questionnaire that elicited their assessment of their children's postoperative recovery and relief of the symptoms of OSDB.
The choice of whether a child had a partial or total tonsillectomy was made preoperatively by the caregivers. Caregivers were told during the preoperative consultation that children who have partial tonsillectomy may have less postoperative discomfort compared with total tonsillectomy. They were also told that there was a risk of tonsillar regrowth after partial resection.
Data collected from the outpatient records were the patient's age, gender, and history of symptoms of OSDB. Data collected from the inpatient records were the amount of intraoperative blood loss and the occurrence of intraoperative complications, and immediate and delayed postoperative complications (dehydration and hemorrhage). Data obtained by the caregiver telephone survey included the caregiver's subjective assessment of the child's postoperative pain as being none, mild, moderate, or severe during recovery (on postoperative days 1 to 3, 4 to 6, and 7 to 9; after day 9; and globally); number of days until return to normal activity; number of days until return to normal diet; number of days of analgesic use; and relief of the symptoms of OSDB. The telephone surveys were conducted by one of the authors (C.A.S.) retrospectively and in an unblinded way, from 1 month up to 12 months after the surgery.
This study was approved by the Cleveland Clinic Foundation Institutional Review Board.
Surgical Technique
Orotracheal intubation is performed with the child in the Rose position. A mouth gag is used to retract the jaw. The soft palate is retracted with catheters in anticipation of a concurrent adenoidectomy; this stabilizes the tonsil and pulls the uvula out of the way. Resection begins with the left-side tonsil, with the microdebrider (set to 1500 rpm in oscillating mode) held in the right hand, and moves from the inferior to the superior pole, starting medially and proceeding laterally. When the plane of the pillars has been reached, a Hurd elevator is used to retract the anterior pillar, medialize the remaining tonsil, and allow deeper portions of the tonsillar tissue to be shaved. Care is taken to leave a thin rim of lymphoid tissue on the tonsillar capsule. After resection has been completed, suction cautery is used to control the bleeding from the left-side tonsillar bed. The right-side tonsil is then similarly resected with the microdebrider held in the left hand. Power-assisted adenoidectomy 2 is performed in conjunction with most cases after the intracapsular tonsillectomy.
The conventional (total) tonsillectomies were performed using the handheld electocautery wand at a setting of 10 to 15 W in a standard fashion by all 3 surgeons.
Statistical Methods
Descriptive statistics are given as median and quartiles (25th and 75th percentiles) for ordinal and nonnormally distributed continuous data and as frequency and percent for categorical data.
The significance level for each hypothesis was 0.05. SAS statistical software (Cary, NC) was used for all analyses.
Univariable Methods
Treatment techniques were compared on the ordinal outcomes (pain during recovery and postoperative quality of life improved), nonnormally distributed continuous outcomes (days to normal activity, days to normal diet, days of analgesic, and blood loss), and baseline predictors using the nonparametric Wilcoxon rank sum test. Techniques were compared on categorical predictors and outcomes with X 2 tests.
Multivariable Methods
Because this was not a randomized study, it was important to adjust for any preoperative factors that might affect the outcome, especially factors that might be different between the technique groups. We considered age at surgery, gender, preoperative life affected, inpatient/outpatient status, tonsillar hypertrophy, adenoidal hypertrophy, OSDB symptoms, snoring, sinusitis, peritonsillar abcess, recurrent otitis, sleep problems, and apnea as potential covariates in multivariable analyses assessing the relationship between technique and the various outcomes. We also compared the technique groups on these variables.
Cumulative logit regression models were used to compare the treatment techniques on pain during recovery and postoperative quality of life improved adjusting for covariates significant at the 0.05 level using backwards variable selection. To satisfy the proportional odds assumption, the moderate and severe pain categories were sometimes combined. An odds ratio and 95% confidence interval (CI) are reported for each factor. The odds ratio indicates the odds of getting a worse outcome in the total versus the partial tonsillectomy.
Cox proportional hazards regression models were used to compare the treatment techniques on the time-to-event outcomes (days to normal activity, days to normal diet, days of analgesic) adjusting for covariates significant at the 0.05 level using backwards selection.
Regression models were used to compare the treatment techniques on the ranks of the continuous variables (blood loss and fluid infusion).
The proportions with resolution (and 95% confidence interval [CI]) for those who had the symptoms before surgery are given.
RESULTS
The Data
We compared the total tonsillectomy and partial tonsillectomy groups on the interested outcomes for the children with tonsillar hypertrophy with OSDB.
Demographic variable by technique
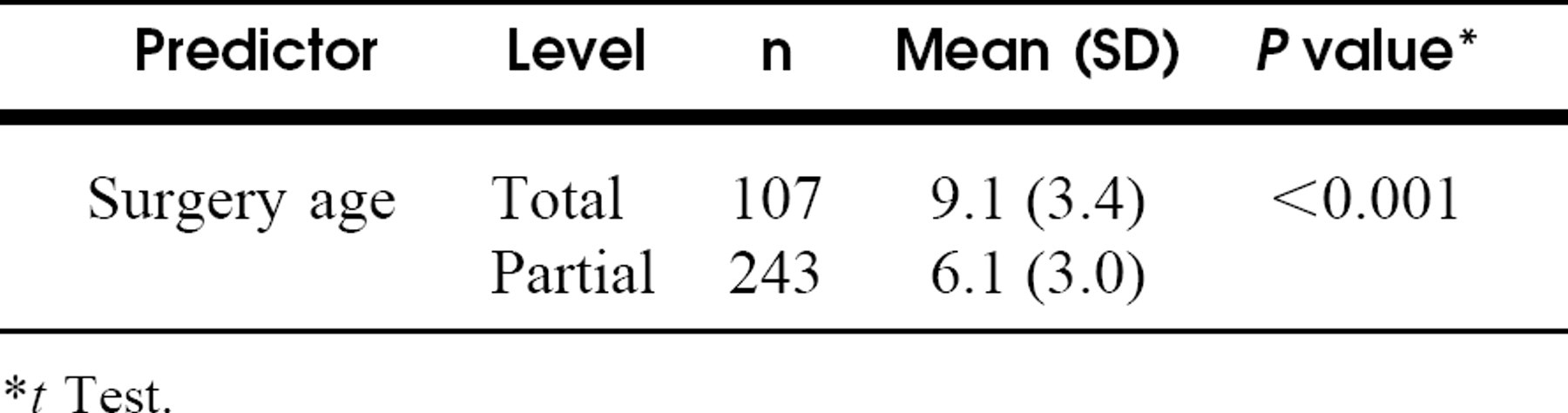
* t Test.
Significant associations between baseline predictors and treatment for the data are as follows: sleep problem (P = 0.002), apnea (P = 0.007), and surgery age (P < 0.001).
Tables 1 to 5 summarize the comparison of the partial tonsillectomy and total tonsillectomy on the main outcomes for our data.
Univariable Results
Partial tonsillectomy was significantly better than total tonsillectomy with less pain during recovery on day 1 to 3, day 4 to 6, day 7 to 9, day 9+, global pain, days to normal activity, days to normal diet, and days of analgesic. We did not detect a significant difference between techniques on the blood loss or postoperative life improved.
Multivariable Results
After adjusting for significant covariates (Tables 3 and 4), partial tonsillectomy was significantly better than total tonsillectomy with less pain during recovery on days 1 to 3, days 4 to 6, days 7 to 9, day 9+; global pain; days to normal activity; days to normal diet; and days of analgesic. Multivariable cumulative logit regression on the quartiles of blood loss indicated that total patients were significantly less likely to have greater blood loss compared to the partial tonsillectomy patients (estimated odds ratio [CI] 0.42 [0.25, 0.71]) after adjusting for significant predictors sinusitis with OR (CI) 2.0 (1.02, 3.8) and age at surgery with OR (CI) 1.3 (1.2, 1.4) (Table 4). Due mainly to the partial patients being younger (Table 1) and the strong positive correlation between surgery age and blood loss, the age-adjusted analysis shows partial patients to have higher blood loss than total patients. Almost identical results were derived using quintiles of blood loss as the outcome.
Other baseline variables by technique
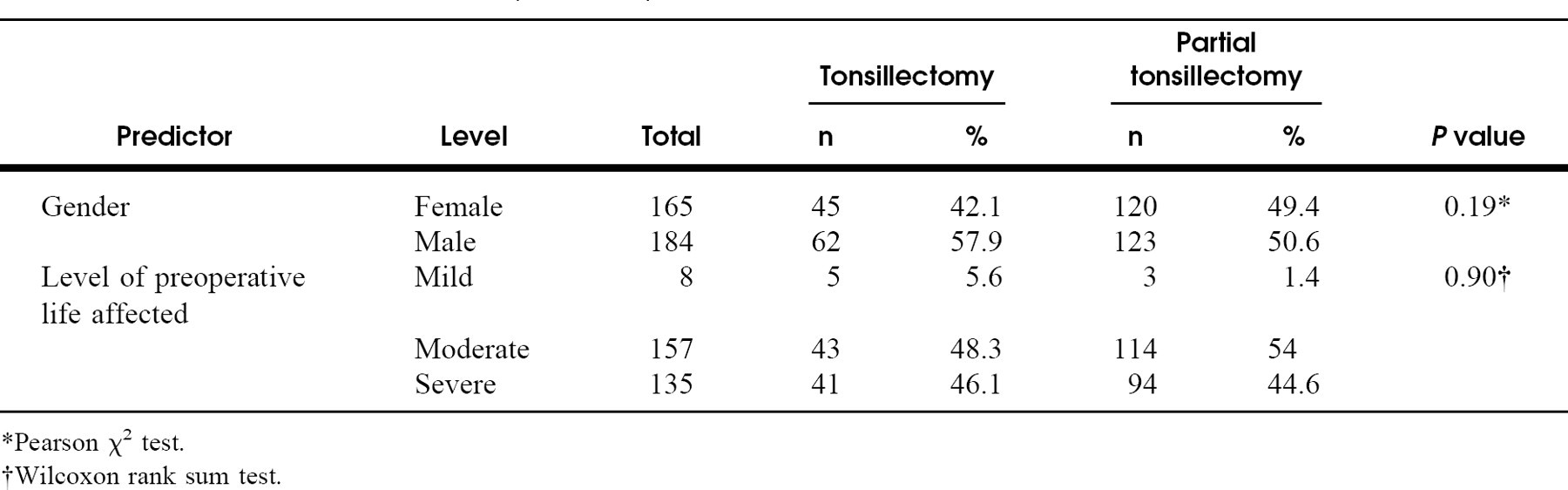
*Pearson χ 2 test.
†Wilcoxon rank sum test.
Comparison of 2 techniques on ordinal follow-up outcomes
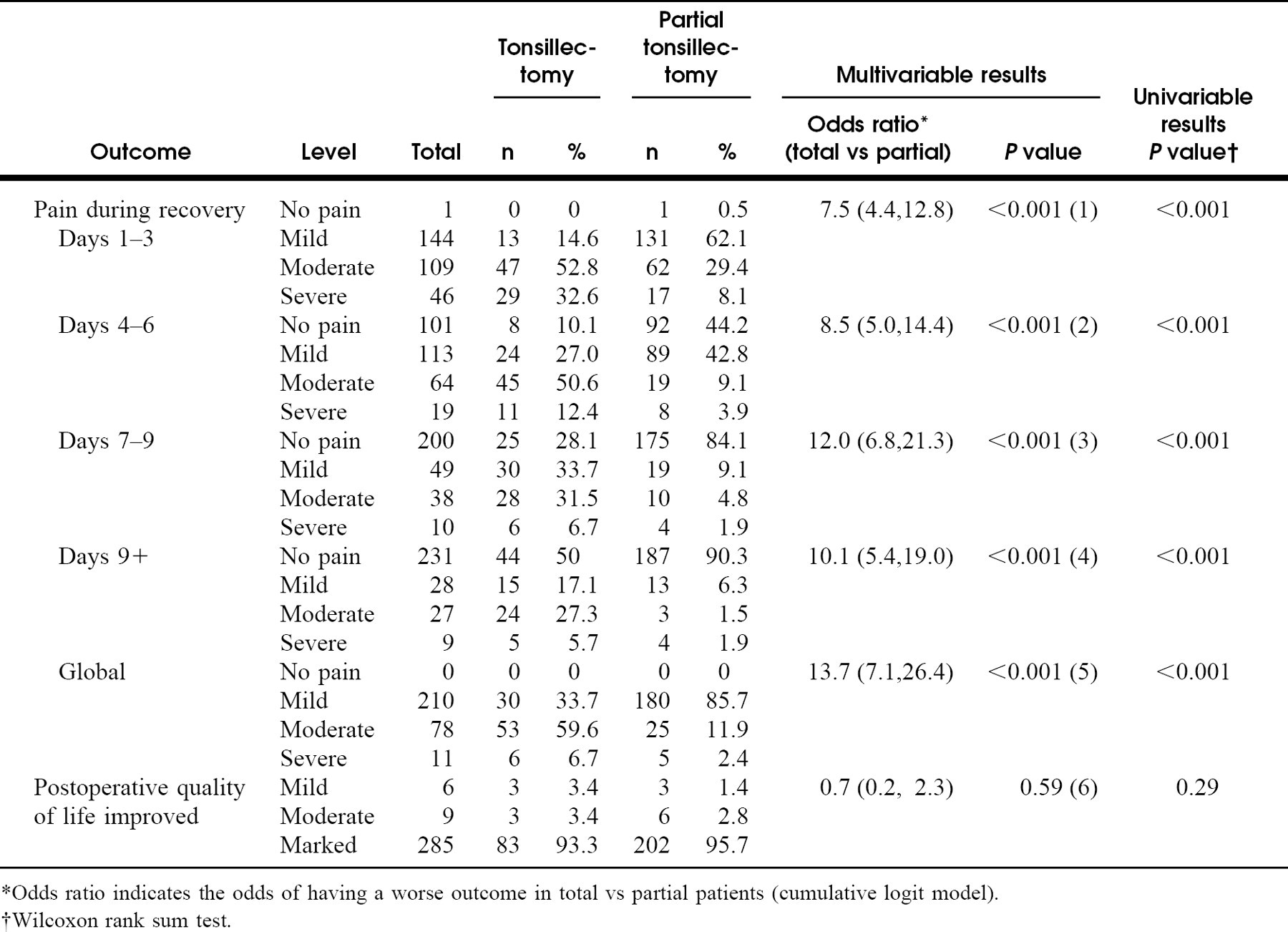
*Odds ratio indicates the odds of having a worse outcome in total vs partial patients (cumulative logit model).
†Wilcoxon rank sum test.
We did not detect a significant difference between techniques on improvement of postoperative quality of life. No differences were found between the groups on the incidence of delayed complications (Table 5).
The variability of the numbers in the various categories (Tables 1 to 5) reflect missing data points in the medical records, inability to contact caregivers, or the lack of recall of specific information by the caregivers during the telephone survey.
DISCUSSION
There have been changes in the methods used in tonsil surgery since the first description from the first century AD by Celsus, who used a finger to remove the tonsil and when that method was ineffective, recommended a scalpel. 3 Philip Physick of Philadelphia invented the first major advance in tonsil surgery when he described the tonsillotome or tonsil guillotine in 1828. 4 With this instrument, tonsil surgery came to be performed with an increasing frequency. Contemporary tonsillectomy, a complete removal of the entire tonsil by anatomic dissection, was conceived and described by American otolaryngologists in the early 1900s in response to persistent symptoms that some patients complained of and which were attributed to retained tonsillar tissue after tonsillotomy. 5 G. Hudson Mauken of Philadelphia first made the distinction between an “intracapsular” and an “extracapsular” tonsillectomy. 6 In 1910, Sluder 7 and Whillis and Pybus 8 independently published their techniques of tonsillectomy with a guillotine in which they were able to remove the tonsil in its entirety with the capsule intact. As a result, tonsillotomy fell into disrepute and was not read-dressed in a meaningful way again for another 80 years. 9,10
Comparison of 2 techniques on continuous outcomes
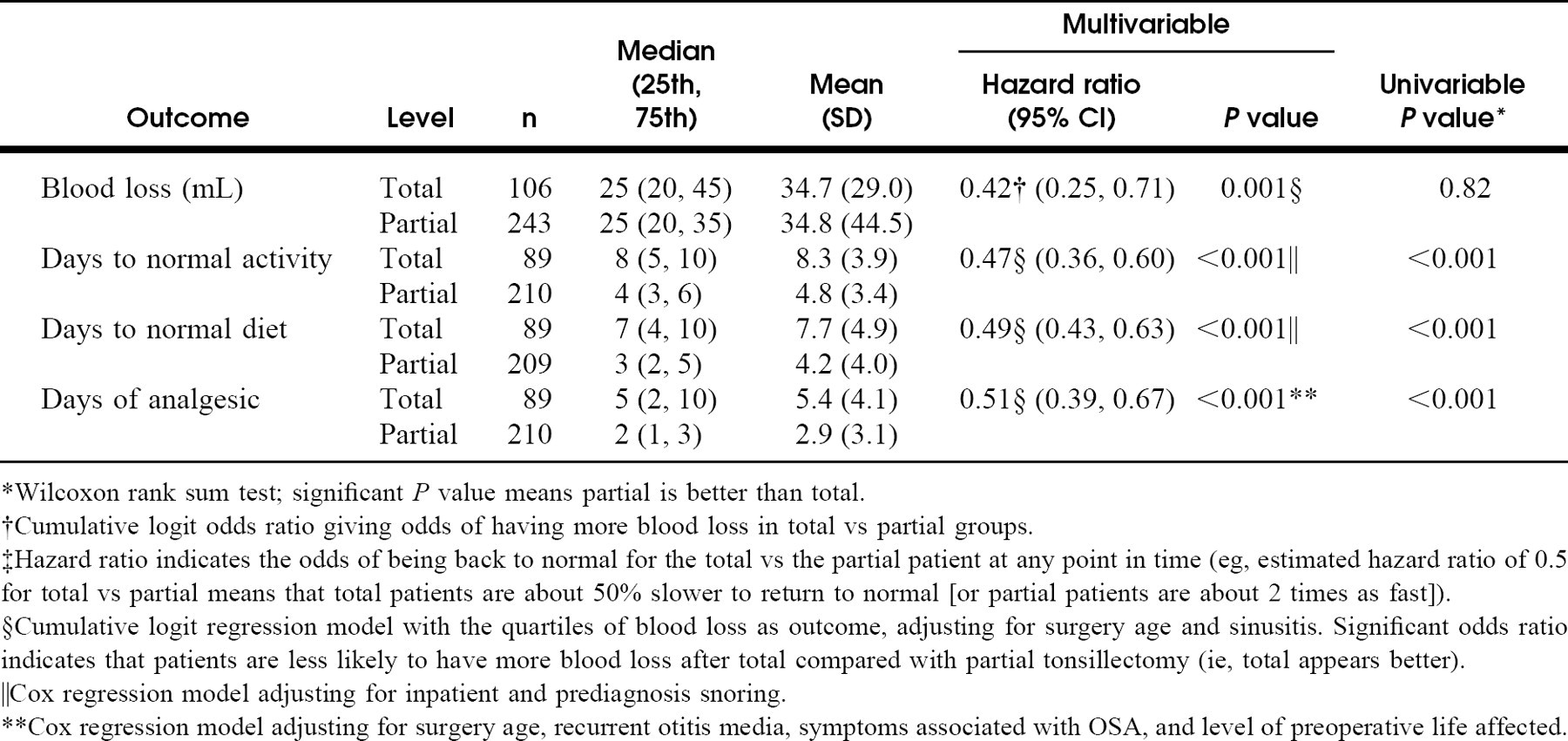
*Wilcoxon rank sum test; significant P value means partial is better than total.
†RCumulative logit odds ratio giving odds of having more blood loss in total vs partial groups.
‡Hazard ratio indicates the odds of being back to normal for the total vs the partial patient at any point in time (eg, estimated hazard ratio of 0.5 for total vs partial means that total patients are about 50% slower to return to normal [or partial patients are about 2 times as fast]).
§Cumulative logit regression model with the quartiles of blood loss as outcome, adjusting for surgery age and sinusitis. Significant odds ratio indicates that patients are less likely to have more blood loss after total compared with partial tonsillectomy (ie, total appears better).
‖Cox regression model adjusting for inpatient and prediagnosis snoring.
**Cox regression model adjusting for surgery age, recurrent otitis media, symptoms associated with OSA, and level of preoperative life affected.
Comparison of 2 techniques on delayed complications
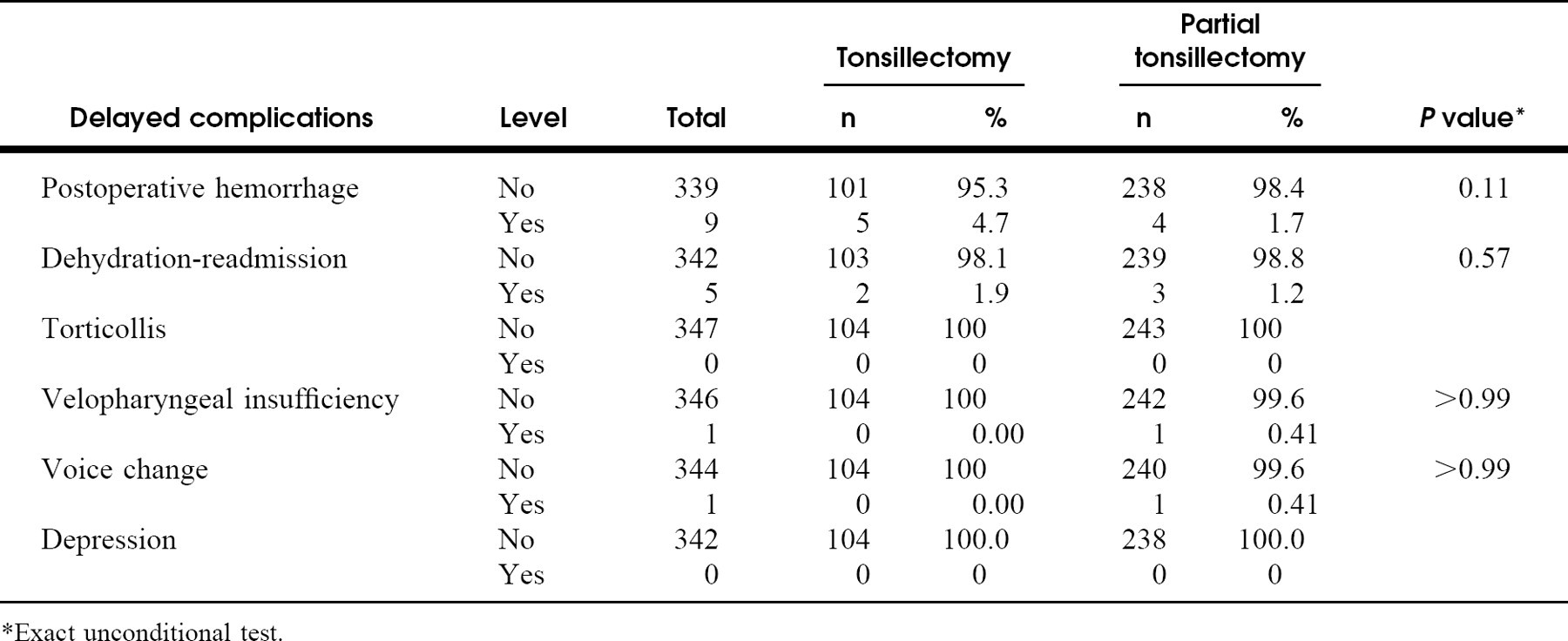
*Exact unconditional test.
By the 1950s, the morbidity of conventional adenotonsillectomy came to be better understood and attention to hemostasis was intensified. 11 Electrocautery for control of tonsillar hemostasis for tonsillar bleeding is first mentioned in 1962 12 and was initially used in conjunction with suction for controlling bleeding after cold dissection. By the 1980s, many surgeons had worked out a technique using the guarded blunt electrocautery tip as the primary instrument for the entire dissection. With the advantage of short operative time and minimal blood loss, the electrocautery dissection technique is probably the most common method of tonsillectomy in the United States today. However, postoperative pain, which is thought to be intensified by the thermal trauma of electrocautery, and delayed postoperative hemorrhage remain a problem, and the quest for improved techniques of total tonsillectomy continue. 13,14
Concurrent with the technical changes that have occurred over the past 100 years of tonsillectomy have been the changing indications. Although much of the historical literature addresses the problem of recurrent tonsillar infection, much of the current concern revolves around the problem of tonsillar hypertrophy resulting in obstructed breathing during sleep. This raises the question about the necessity of removing all of the tonsils when only part of them is causing the obstruction. Our experience and results suggest that the answer to this question is no.
Clarification regarding the appropriate nomenclature of our procedure requires some comment. A guillotine tonsillotome performs a tonsillotomy, which literally means a “hole or incision” in the tonsil. We are doing something much more anatomic and purposeful. Intracapsular tonsillar reduction (we like the descriptive term “partial ton-sillectomy”) specifically addresses the source of pharyngeal obstruction. At the same time, the operation maintains some of the native tissues as a surgical barrier and reduces the postoperative inflammation in the pharyngeal muscles, resulting in significantly less postoperative pain and a more rapid recovery.
Another important aspect of partial tonsillectomy is concern about tonsillar regrowth and subsequent infection of the tonsillar remnant. Although this has not so far been observed in this group of patients, historical evidence suggests that eventually this will happen in some percentage of cases. 15 Our concern is not trivial and has been the primary reason for considering chronic tonsillitis, and even infrequent tonsillitis, as a contraindication to partial tonsillectomy for now. We acknowledge these problems and recognize that they will be a cause of controversy. Nevertheless, today, when most tonsillectomies in children are done for hypertrophy, partial tonsillectomy relieves OSDB as effectively as total tonsillectomy but with less pain and perhaps a greater margin of safety.
We have continued to use the endoscopic microdebrider, and thus far it seems to be the most useful device for partial tonsillectomy, although it is not ideal. None of the other techniques we have tried, including the guillotine, 16 electrocautery, 17 CO2 laser, 9,10 coblation, 18 radiofrequency ablation, 19 and the harmonic scalpel, 14 provide nearly as rapid, complete yet precise control in resecting the tonsil without violating the capsule. One disadvantage of the microdebrider is that it increases the intraoperative blood loss, which can obscure tissue specificity, especially in the deeper sections of the tonsillar excavation, risking injury of the pharyngeal musculature. This is preventable by maintaining visual contact with the cutting tip of the shaver blade, performing a layered resection and intermittently using the suction cautery to control excessive bleeders.
Other negative considerations include the cost of the shaver blade, around $80, which increases the expense of the procedure. On the other hand, the same shaver blade may be used for both partial tonsillectomy and power-assisted adenoidectomy. Finally, microdebrider partial tonsillectomy takes a few minutes longer to perform than total electrocautery tonsillectomy, although the average difference in an informal survey of 20 conservative cases was only 3 minutes.
As with any retrospective study, we attempted to control for factors other than surgical technique that might have an impact on patient outcome. However, our methodology using retrospective chart reviews and unblinded telephone surveys renders our results vulnerable to both recall bias and survey bias. Moreover, our preoperative explanation about the diminished postoperative pain expected with partial tonsillectomy introduces information bias, which weakens the power of our results. A randomized trial will be an important step in clarifying the superiority of partial versus total tonsillectomy in all outcomes of interest.
CONCLUSION
We have revived an old style of tonsillar surgery, partial tonsillectomy, using contemporary technology in the form of an endoscopic microdebrider for the management of tonsillar hypertrophy causing OSDB in children. We have found the technique safe and reliable and have shown that it effectively relieves OSDB, but results in significantly less postoperative pain and a more rapid recovery compared with electrocautery dissection total tonsillectomy. We have not had a problem of tonsillar regrowth or subsequent chronic infection of the tonsil remnants in any of the children thus far treated.
The authors would like to acknowledge the assistance of Scott Beam in preparation of the manuscript.