
Abstract
OBJECTIVE: Our goal was to present our experience with the free anterolateral thigh flap for reconstruction of various cutaneous and mucosal defects of the head and neck.
STUDY DESIGN: We conducted a retrospective review of 37 patients who underwent reconstruction between 1994 and 2002. Outcome measures included ethnicity, flap harvest technique, vascular anatomy, flap success, general surgical complications, and donor site morbidity.
RESULTS: The majority of our patients were white (n = 33). The size of the 39 free anterolateral thigh flaps varied from 24 to 252 cm 2 . There was 1 arterial failure and flap loss (2.6%) and 2 venous occlusions that were both salvaged. The donor site was closed primarily in 37 cases and with a split-thickness skin graft in 2 cases.
CONCLUSIONS: This is the first report on using the free anterolateral thigh flap in whites. This free transfer has proved to be a versatile and reliable flap for reconstruction of the head and neck.
This flap has some significant advantages for reconstruction of the head and neck. It can be raised as a subcutaneous flap, a fasciocutaneous flap, or a myocutaneous flap and can resurface large defects in the head and neck. In addition, it has a large and long vascular pedicle, and because of the distance of the donor site from the head and neck, it can easily be harvested with a 2-team approach.
This flap has not gained widespread use in North America largely because the dissection of this flap may be technically difficult due to varying anatomy of the perforating branches of the descending branch of the lateral circumflex femoral artery. 3,7 In addition, the lateral thigh donor site in many white North American patients is considerably thicker than that of the Asian population due to the differential body habitus and incidence of obesity in this population.
The purpose of this study was to report our surgical experience with the use of the anterolateral thigh flap in head and neck reconstruction in a white population. This is the first report to describe the results of the use of the anterolateral thigh free tissue transfer in a North American population.
METHODS
We reviewed the records of 37 consecutive patients undergoing 39 anterolateral thigh free tissue transfers for head and neck cancer surgery defects between 1994 and 2002 at the University Health Network, Toronto, Ontario. Details were collected on the patients' age, gender, ethnicity, pathology of the neoplasm, previous treatment, and comorbidities. The site of reconstruction, flap-harvesting technique, recipient vessels used, flap-related complications, general surgical complications, donor site morbidity, and operative time were noted.
Flap Anatomy
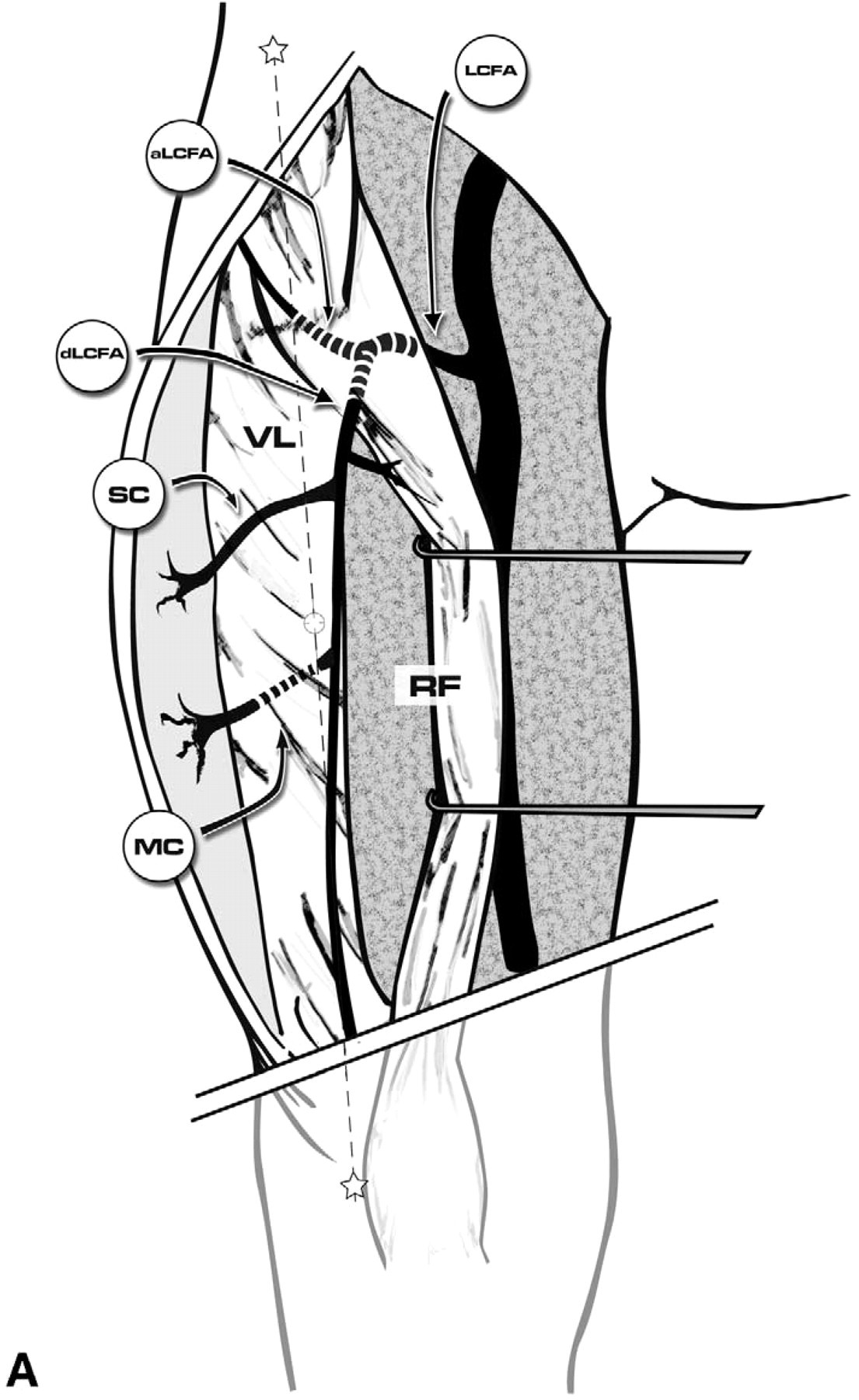
The anterolateral thigh flap is supplied by perforating vessels arising from the descending branch of the lateral circumflex femoral artery. The descending branch runs downward in the intramuscular space between the rectus femoris and the vastus lateralis, terminating in the vastus lateralis just above the knee. In the midportion of the lateral thigh, the descending branch provides a number of perforators to the skin of the lateral thigh. These perforators can either run between the rectus femoris and vastus lateralis muscle and traverse the fascia lata as septocutaneous perforators to supply the skin of the lateral thigh or they can traverse the vastus lateralis muscle and the deep fascia as musculocutaneous perforators to supply the skin (Fig 1A). The length of the pedicle is 8 to 16 cm and usually has 2 venae commitantes. 6
Harvesting Techniques
The free tissue transfers in this series were harvested by 3 surgeons (R.G., P.N., J.L.). The harvest technique is similar to that described by Wei et al 6 in 2002. The skin perforators of the lateral thigh are mapped with Doppler, using the midpoint of a line drawn between the anterior superior iliac spine and the lateral aspect of the patella as a landmark. The first skin incision is placed on the medial aspect of the flap design. If a suprafascial technique is to be used for a thin flap, the dissection is carried laterally until the major perforators to the skin are identified. If a fascio-cutaneous harvest is planned, the incision is carried through the deep fascia with the flap site mobilized laterally until the perforating vessels are visualized traversing the deep fascia. Once the perforators are identified, the skin incisions are completed and the pedicle dissected in a retrograde fashion either to the descending branch for septocutaneous flaps or through the vastus lateralis in patients with myocutaneous perforators (Fig 1B). In myocutaneous perforators, we have usually left a small cuff of muscle around the pedicle to protect the small perforating branches. Great care should be used to maintain hemostasis in this portion of the elevation because the vessels frequently will go into spasm and the muscle may bleed excessively after revascularization. As the dissection proceeds proximally, great care is taken to avoid injury to the motor nerves to the vastus lateralis and rectus femoris. The lateral femoral cutaneous nerve of the thigh may be included in patients requiring innervated reconstructions. If a thinned subcutaneous flap is required, this is done with judicious thinning of the deep layer of fat, avoiding the vascular pedicle. 3
RESULTS
Patient Characteristics
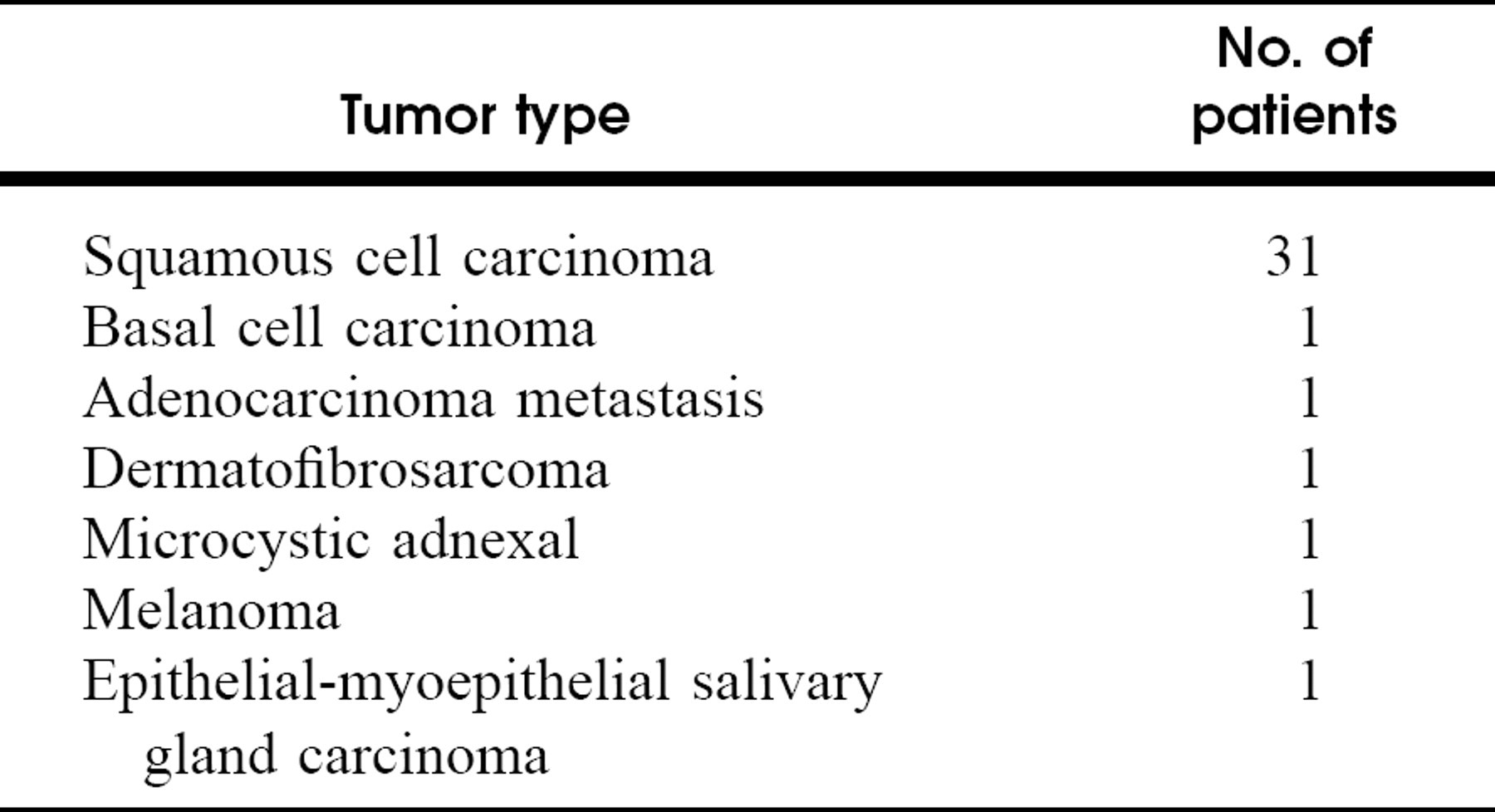
Thirty-seven patients (28 men and 9 women; median age, 62 years; age range, 32 to 89 years) underwent reconstruction with an anterolateral thigh free tissue transfer. Three patients were of Asian ethnicity, and the remainder were white. All of the patients were treated for malignant tumors. The pathology of the various neoplasms in this series is given in Table 1.
Free Flap Harvesting
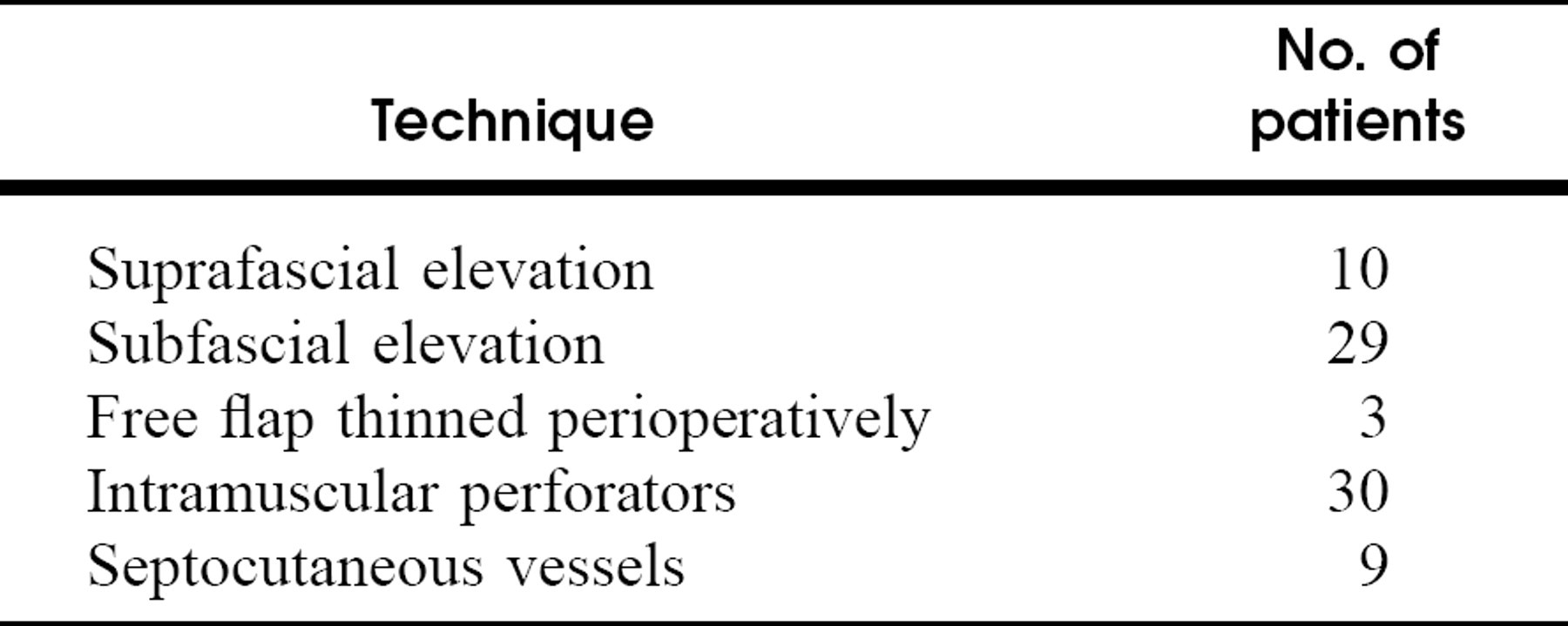
Details on free flap harvesting techniques and the vessels used for these flaps are given in Table 2.
Pathology of the tumors
Harvesting techniques in 39 anterolateral free flaps
Free Flap Reconstruction
There were 39 reconstructions with a free anterolateral thigh flap in the series of 37 patients. Details on these reconstructions are summarized in Table 3. Two patients required a second resection and free flap reconstruction: 1 for a neck wound dehiscence and partial necrosis of the neck skin flap and 1 for recurrent disease. The median size of free flaps used in this series was 132.5 cm 2 (range, 24 to 252 cm 2 ). The donor site was closed primarily in 37 cases and with a split thickness skin graft in 2 cases. The median operative time, including the resection of the tumor, neck dissection and reconstruction with anterolateral thigh free flap, was 10.5 hours (range, 7 to 12 hours).
Outcome
The overall success rate was 97.4% (38 of 39). One anterolateral thigh flap died 2 days postoperatively. The patient had been operated on for recurrent (rT4 N0) squamous cell carcinoma of the maxillary sinus. In this case the thin portion of the pedicle that had traversed the vastus lateralis was compressed against zygomatic process, resulting in total flap loss. Four patients had venous outflow problems. Two had venous occlusions at the anastomotic site and were salvaged with reanastomosis. Two patients had venous compression from overlying structures: one, a mandibular reconstruction, and the other, an edematous sternocleidomastoid muscle. Both were salvaged by repositioning of the pedicle. There were no late complications and no donor site complications in the present series of patients. One postoperative neck hematoma and 1 postoperative neck abscess required operative exploration. There were 2 other postoperative neck explorations due to minor hematomas, with no obvious flap-related problems. One patient had a mandibular nonunion of the osteotomy, which was managed operatively. One patient experienced acute respiratory distress 21 days postoperatively and underwent a repeat tracheostomy.
Flap characteristics of 39 anterolateral free flaps
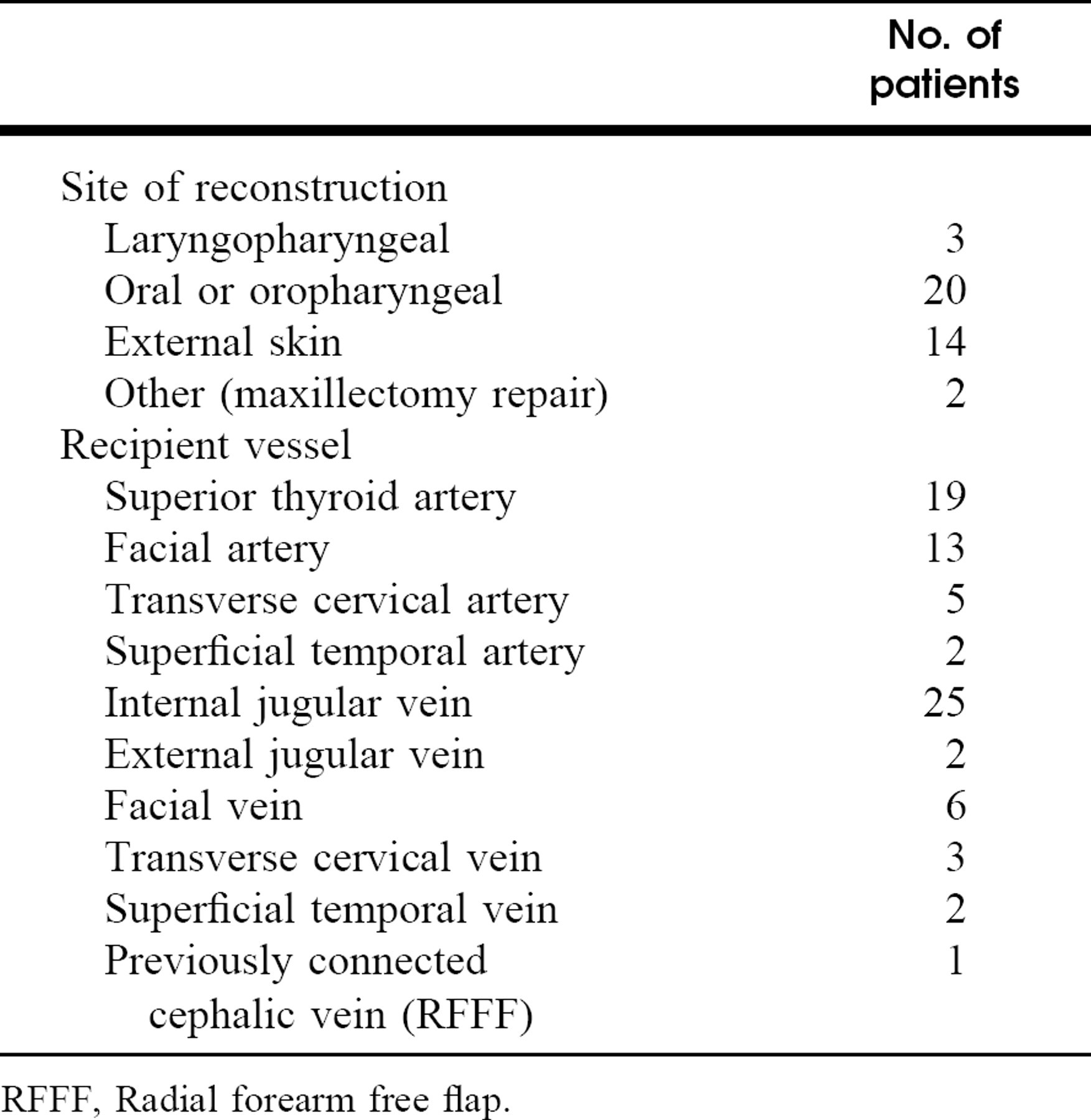
RFFF, Radial forearm free flap.
CASE REPORTS
Case 1
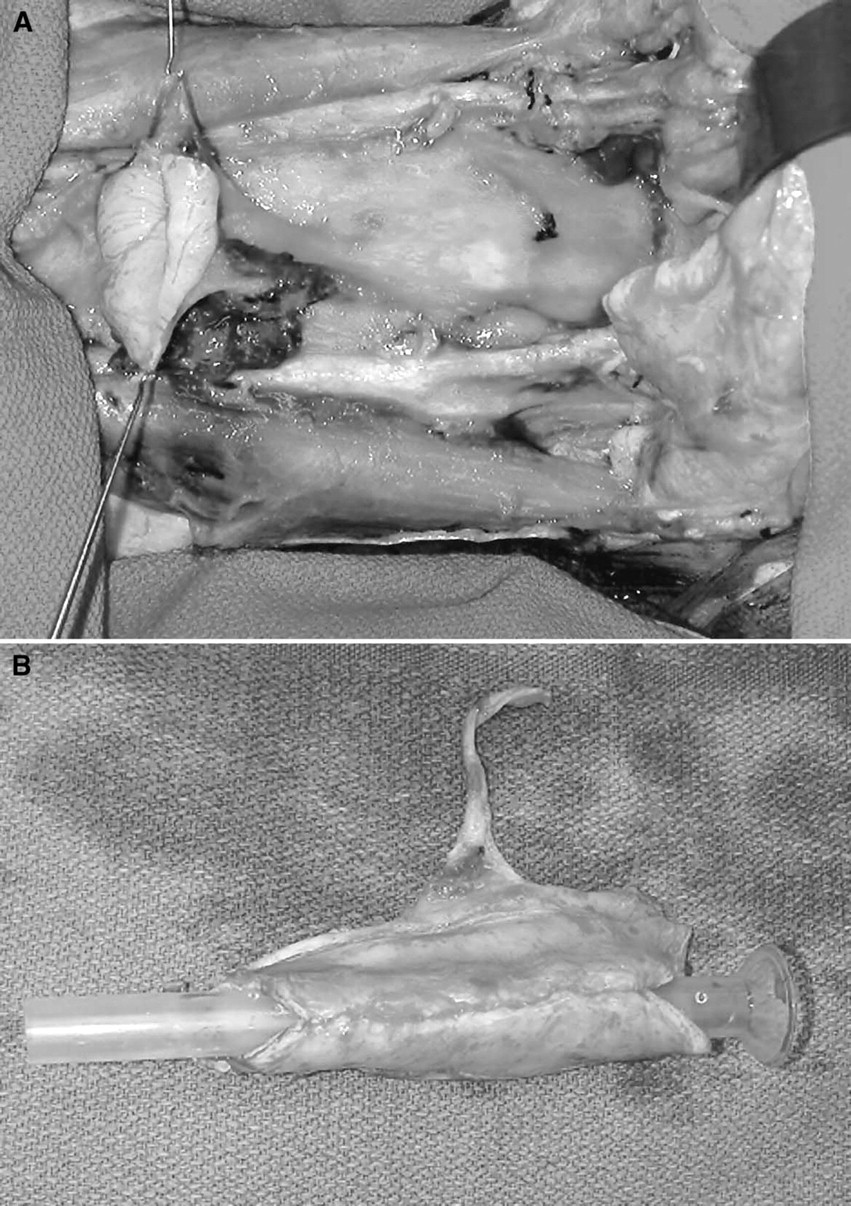
A 42-year-old man presented with a recurrent spindle cell variant of squamous cell carcinoma of his laryngectomy stoma. He had previously undergone radiation therapy and total laryngectomy. The size of the surgical defect was estimated pre-operatively to be approximately 140 cm 2 . At surgery, radical resection of the affected tracheostomal region and left hemithyroidectomy were performed (Fig 2A). This included resection of a segment of the trachea and dissection of the anterior superior mediastinum. An anterolateral thigh flap was used to cover the defect (Fig 2B). He remains alive and disease free over 16 months postoperatively, with a good functional and aesthetic result.

Patient 2
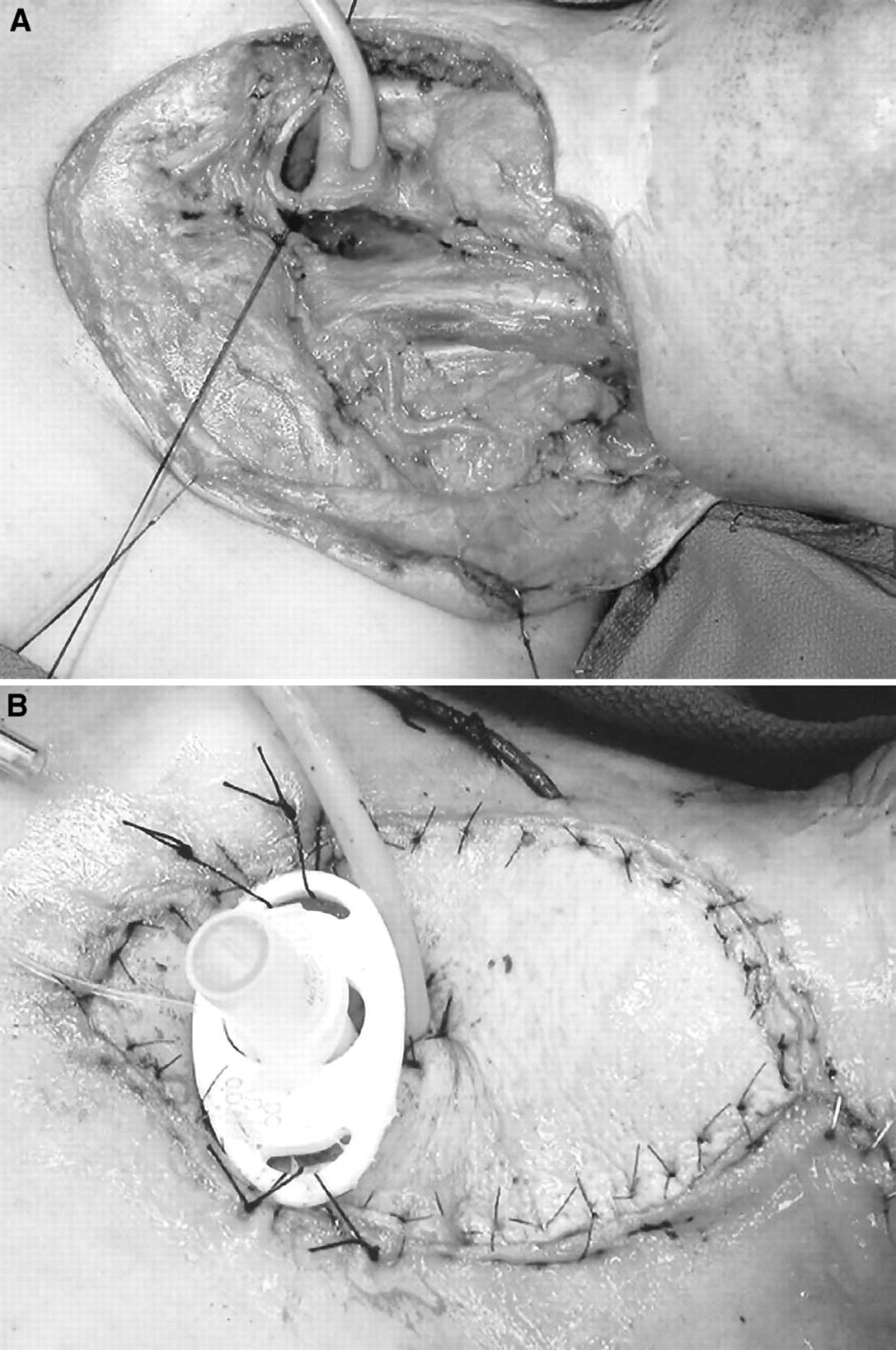
A 54-year-old man presented with T4 N0 squamous cell carcinoma of the hypopharynx. The tumor involved transglottic structures and circumferentially the hypopharynx extending superiorly to the tonsil. It had invaded posterior cricoid cartilage and right arytenoid cartilage. At surgery, a total laryngopharyngectomy, total thyroidectomy, and bilateral functional neck dissection (levels I, II, III, and IV) were performed (Fig 3A). A tubed anterolateral thigh flap and a salivary bypass tube were used to repair the defect (Fig 3B and C). Before closure, a TE puncture was performed to create a fistula for a voice prosthesis. The patient remains disease free 16 months postoperatively with an excellent fistula voice.
DISCUSSION
We described a single institution's experience with the free anterolateral thigh flap in 37 patients undergoing 39 reconstructions of various defects of the head and neck. The majority of our patients were white, with an overall flap success rate of 97% and an acceptable major surgical complication rate. The distribution of flap anatomy (ie, septocutaneous versus musculocutaneous perforators) in our series was predominantly musculocutaneous, as described by other authors.
Two harvest techniques, as described by Wei et al, 6 have been used by our reconstructive group. In 10 patients requiring thin flaps, we used a suprafascial harvest technique with 3 patients undergoing flap thinning. In 29 patients, we used the more common subfascial technique. Our series suggested that flaps may be judicially thinned without complications. 8 It has been our experience that the suprafascial technique of defining perforators and following them through the fascia and vastus lateralis muscle is more tedious and technically more difficult. We would therefore recommend that for the surgeon developing an experience with this flap, the subfascial approach be considered before a suprafascial harvest is attempted.
The donor site complications associated with this flap appear to be minimal, with the majority of sites closed primarily without the need of a skin graft. This finding is consistent with the report of Kimata et al, 9 who demonstrated that donor site morbidity was dependent on the extent of injury to the vastus lateralis and the need for a skin graft to achieve donor site closure. As a routine, we recommend that the innervation to the vastus lateralis be protected whenever possible in the harvest of this flap.
Our series supports the observations of others regarding the utility of this flap for reconstruction of a variety of surgical defects of the head and neck. Mucosal defects in the head and neck region in whites have been reconstructed with various fasciocutaneous free transfers, with the radial forearm flap and lateral arm flap used most frequently. The anterolateral thigh flap offers certain advantages over both of these flaps in appropriately selected patients with thin lateral thighs. It has a large cutaneous area available for transfer and can include the lateral cutaneous nerve of the thigh to provide sensation. Because of the distance of the donor site from the head and neck, the flap can be elevated simultaneously with tumor ablation. The donor site can usually be closed primarily with a much more acceptable donor site scar than the forearm flap.
This flap can easily be tubed for reconstruction of the total laryngopharyngectomy defect defects in thin patients and has the advantage in this setting of a thick layer of deep fascia, which can be used to reinforce the pharyngeal repair. The flap also has great usefulness for a variety of soft tissue and cutaneous defects and is suitable for dead space filling and contouring in the head and neck region. 10
Contraindications for the use of this flap would be patients with previous surgery in the upper thigh, including major vascular bypass procedures. Patients with excessive subcutaneous fat due to obesity or body habitus are not good candidates for this flap, as the flap will usually be too bulky for a head and neck recipient site and the dissection will be technically quite difficult. In general, if the thigh appears to be excessively thick for an individual recipient site, we select a different donor site with appropriate subcutaneous thickness.
Major complications were infrequent in this series, with the loss of one flap due to external compression of the muscular perforator portion of the vascular pedicle. In addition, there were 4 patients who required reexploration for reduced venous outflow. Two of these patients had venous occlusions at the anastomotic site, and both were salvaged with repeat anastomosis. The remaining 2 patients had from local compression of the muscular perforator portion of the pedicle, and after the release of overlying soft tissue, both were salvaged. This experience with venous occlusion/compression illustrates the fact that unlike other fasciocutaneous or cutaneous free flaps, this flap is more at risk of venous obstruction from local compression of the pedicle. This is likely because the portion of the vascular pedicle, which is dissected through the muscle, is extremely small and therefore sensitive to compression. To avoid this problem, the surgeon using this flap must take great care to avoid local compression of the vascular pedicle.
CONCLUSION
This is the first report on the use of the free anterolateral thigh flap in a North American population. We have found this free transfer to be a reliable and safe method for the reconstruction of various head and neck defects after tumor resection. This flap is relatively easy to harvest once the anatomic variations of this flap are clearly understood. We anticipate that this reconstruction will likely replace the forearm flap as the reconstruction of choice for oral cavity reconstruction in appropriately selected patients with thin lateral thighs. In addition, the use of this flap in a wide variety of reconstructive problems ensures its role in the armamentarium of the head and neck reconstructive surgeon.