
Abstract
Lactescent pleural effusions are commonly recognised in cats. Although the sequelae of excessive pleural fluid can quickly become life-threatening, the clinician must take care to treat not only the signs of pleural effusion but to also determine the underlying disorder if appropriate therapy is to be instituted. The pleura is lined by a single layer of flattened mesothelial cells, beneath which is a rich network of blood vessels and lymphatics. The parietal pleura (that covering the thoracic walls, mediastinum and diaphragm) receives its blood supply from the systemic circulation. The visceral pleura (that covering the lungs) is supplied by the low-pressure pulmonary circulation. In the absence of pleural effusion, the parietal and visceral pleura contact each other. There are four basic mechanisms by which pleural fluid may accumulate in abnormal quantities:
Increased capillary hydrostatic pressure, such as in congestive heart failure;
Decreased capillary oncotic pressure as a result of hypoalbuminaemia;
Increased capillary membrane permeability (inflammation);
Lymphatic obstruction.
Clinical signs and physical examination findings
Clinical signs of pleural effusion are dependent on the volume of effusion, the rapidity of its accumulation and the underlying disease process. Lethargy, depression, anorexia, weight loss and coughing are common historical complaints. Because clinical signs are often not noted until the effusion is substantial these animals need to be handled with extreme care. They may need to be given supplemental oxygen (via a mask or oxygen cage) prior to thorough examination. Physical examination findings vary depending on the underlying disease. Consistent findings with pleural effusion are muffled heart sounds and decreased repiratory sounds in the ventral thorax. Findings such as a cardiac murmur, pulse deficits, tachycardia, decreased compressibility of the anterior thorax, distended abdomen, chorioretinitis, trauma, and fever may be important clues as to the underlying disease process.
Diagnostic techniques
Thoracocentesis
Thoracocentesis may serve as either a diagnostic or therapeutic technique. Prior to radiography, thoracocentesis reduces the likelihood of stress-induced respiratory distress. Additionally, removing most of the effusion improves the radiographic visibility of the heart, lung fields and mediastinum. However, because fluid acts as an ‘acoustic window’ for ultrasonograpy this diagnostic modality (often used to detect anterior mediastinal masses) is best performed prior to removing large quantities of fluid. Thoracocentesis is usually performed in the 7th or 8th intercostal space just below the costochondral junction. Allowing the animal to remain in sternal recumbency during the procedure minimises stress, improves ventilation, and increases the removal of pleural fluid. A local block (lidocaine without epinephrine) may be performed, however, in most animals this is not necessary. The hair over the selected site is shaved and the skin prepared aseptically. A small guage (21- or 23-ga.) butterfly catheter attached to an extension tubing and 3-way stopcock works best. The needle is introduced in the middle of the intercostal space, thus avoiding the caudal rib margin and its associated nerve and vessels. Maintaining slight constant negative pressure on the syringe will aid identification of pleural fluid and avoid trauma to the lungs.
The initial samples collected aseptically should be used for laboratory evaluation. Fluid should be placed in a tube with anticoagulant (EDTA) for cell counts and measurement of specific gravity and total protein. Direct smears should also be made for cytologic evaluation. Biochemical parameters should be evaluated in fluid placed in a ‘clot’ tube.
Radiography
Pleural effusion is evident radiographically as interlobar fissure lines, rounding of lung margins at the costophrenic angles, separation of lung borders from the thoracic wall, scalloping of lung margins dorsal to the sternum, blurring or absence of the cardiac silhouette and widening of the mediastinum. At least 50 ml of effusion must be present to be demonstrated radiographically. Large volumes of pleural effusion may cause collapse of lung lobes, decreased visibility of the heart and mediastinum, dorsal elevation of the trachea, and caudal displacement of the diaphragm and liver. In cats the presence of enlarged caudal lobar pulmonary arteries may be a relative sensitive indicator of heartworm disease.
Ultrasonography
As previously stated ultrasonography is best performed prior to removing large volumes of pleural fluid. Anterior mediastinal masses and diaphragmatic hernias are easily detected using this imaging technique.
Aspiration cytology
Cytologic evaluation of pulmonary or intrathoracic masses (such as mediastinal lymphosarcoma or pulmonary adenocarcinoma) may establish the cause of pleural effusion. Radiographs can be used to determine the aspiration site. The skin should be prepared as for thoracocentesis. A 12 ml syringe and a small needle (23- or 25-ga.) should be used. The needle is introduced in the appropriate intercostal space to a depth chosen from the radiographs. The plunger is withdrawn quickly two or three times, all negative pressure is released and the needle removed from the thoracic cavity. The needle is disconnected from the syringe while air is aspirated into the syringe. The contents in the hub of the needle are then forced onto several microscopic slides.
Pleural fluid analysis
The pleural fluid should be evaluated for color, turbidity, odor, and the presence of particulate matter. Turbidity is a measure of the number of cells present; inflammatory effusions being more turbid and modified transudates having lower cell counts. A foul or putrid odor may be suggestive of a septic inflammatory effusion, particularly one associated with an anaerobic organism. Particulate matter such as sulfur granules may be noted with effusions caused by Nocardia. Chemical characteristics such as specific gravity and total protein are determined on fluid preserved with an anticoagulant. Cell counts, although often inaccurate, may be performed and serve as a guide for classifying effusions as transudates, modified transudates, or exudates.
Cytologic evaluation of direct smears is useful in identifying underlying causes. Sediment from a centrifuged sample may be resuspended to make direct smears. Questions to ask are:
is the effusion inflammatory or non-inflammatory,
is the effusion septic or non-septic, and
are neoplastic cells present?
Remember that exfoliated mesothelial cells are difficult to distinguish from neoplastic cells!
Pyothorax
Pyothorax is an accumulation of pus in the pleural space. The fluid is classified as an exudate and can range from amber to red or white in color. The protein content is usually greater than 3.5 gm/dl and the fluid appears turbid or opaque due to the high TNCC. Cytologically the nucleated cells consist primarily of degenerative neutrophils, but nondegenerative neutrophils can predominate, depending on the causative agent (see above under cytological parameters). Effusions associated with fungi and higher bacterial agents such as Actinomyces and Nocardia are often characterised cytologically by nondegenerative neutrophils and macrophages. Apparently these organisms only produce sufficiently large enough quantities of (or strong enough) toxins to cause degenerative changes in those cells found in close proximity to the organisms. The route by which the pleura becomes infected in animals with pyothorax is usually not evident. Possible routes of infection include hematogenous spread, migrating foreign objects such as plant awns, penetrating wounds (particularly bite wounds), extension from diskospondylitis, extension from pneumonia (eg, aspiration pneumonia), pulmonary neoplasia and abscessation, pulmonary or thoracic wall trauma, and postoperative infection. Although diseases that result in immunosuppression (eg, FeLV and FIV) should be excluded in animals with pyothorax, there is no evidence that development of this disease requires debilitation or an increased susceptibility to infection.
Although the cause of the effusion in animals with pyothorax is often not discernible, attempts should be made to find and correct, if possible, underlying diseases. Management of these animals needs to be aggressive. Following the diagnosis, a chest tube should be placed. If available, continuous suction devices are ideal; however, most animals can be managed with intermittent aspiration. Lavage should be performed two to four times daily. Isotonic fluid, such as saline or lactated Ringer's solution (warmed to room temperature) should be used at a dosage of 10 ml/kg body weight. The fluid is allowed to remain in the thoracic cavity for one hour and is then removed. The addition of antibiotics to the lavage fluid offers no advantage over the use of appropriate systemic antibiotics. If antibiotics are used topically, the systemic dose should be decreased in order to minimise toxicity. The use of proteolytic enzymes is controversial and is no longer recommended by most authors. However, the addition of heparin (1500 units/100 ml of lavage) appears to be beneficial. Lavage may be required for five to seven days. Systemic antibiotic therapy should be based on results of microbial culture and susceptibility testing and should be continued for a minimum of four to six weeks.
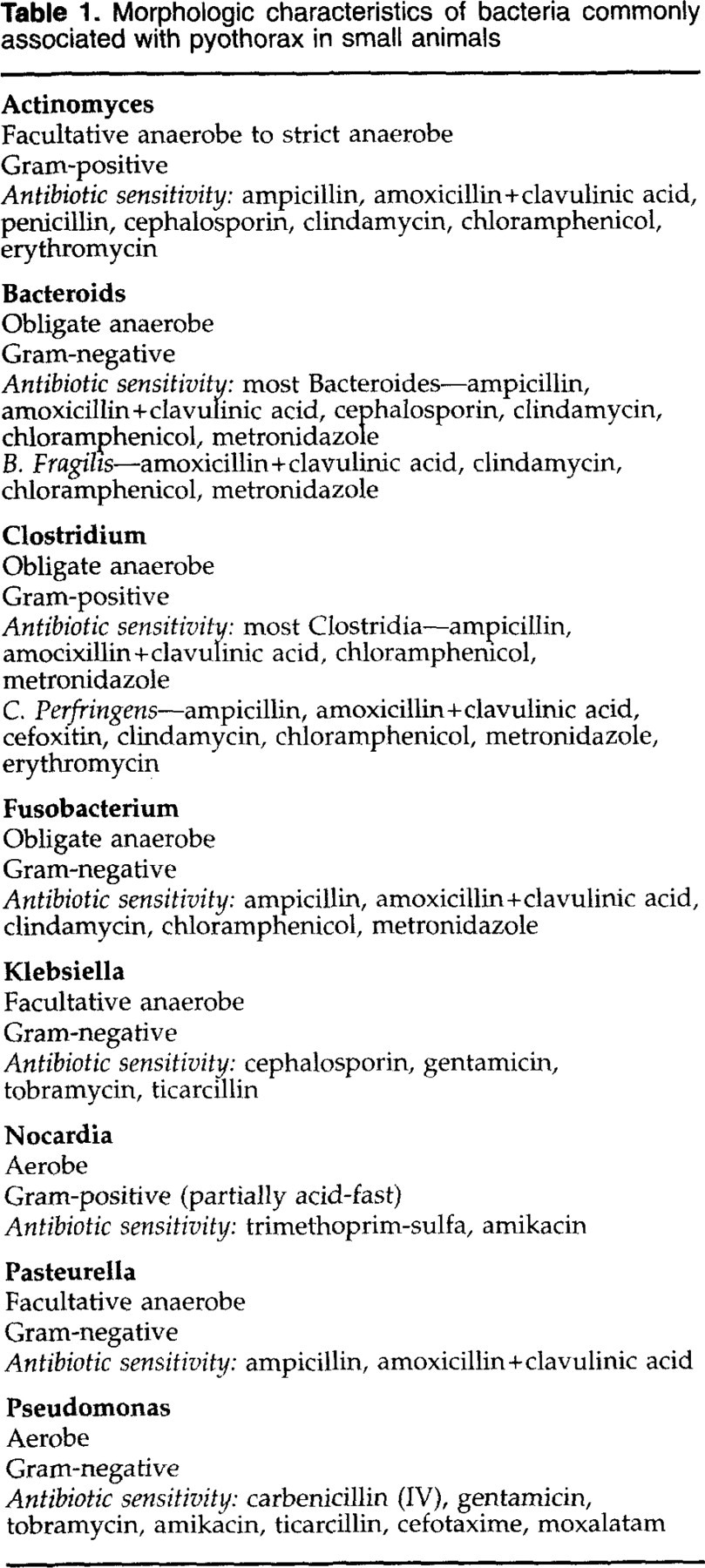
Morphologic characteristics of bacteria commonly associated with pyothorax in small animals
Surgical intervention is indicated if no improvement occurs in the first three to four days of therapy. The thorax may be approached via an intercostal thoracotomy if an abnormality can be localised to one hemithorax, or median sternotomy if localisation is not possible. Explore the thoracic cavity for abscesses, foreign bodies, or other abnormalities, and remove affected tissues. Prior to closure, lavage the thoracic cavity with warmed sterile saline solution. If the pyothorax is chronic or localised, or the patient remains dyspnoeic in the absence of significant volumes of pleural fluid, surgical intervention and decortication may be warranted. Long standing empyema may resorb leaving a pleural ‘peel’ which is a thick sheet of fibroblasts and inflammatory cells attached to the visceral pleura. This pleural peel may inhibit normal expansion of lung tissue. Decortication is recommended in human beings if lung entrapment is suspected. Decortication should be performed once the empyema is mature, but before it adheres to the pleura and becomes vascularised (three to four weeks is recommended).
Feline chylothorax
Chylothorax is a potentially fatal disorder that presents both a diagnostic and therapeutic challenge to the veterinarian. This disease, which is a pathological accumulation of chyle in the thoracic cavity, may be due to a number of underlying disease processes or may be ‘idiopathic’. Chyle is the term used to denote lymphatic fluid arising in the intestine and therefore containing a high quantity of fat. The intestinal lymphatics arborise in the cisterna chyli, a large dilated sac which lies adjacent to the aorta at L1–L4. The thoracic duct (TD) is the cranial continuation of the cisterna chyli. In the cat, the TD lies between the aorta and the azygous vein on the left side of the thorax and terminates in the venous system of the neck (left external jugular vein or jugulo-subclavian angle).
The age of cats affected with chylothorax may range from six months to 16 years. There does not seem to be a sex predisposition, however, Siamese cats may be predisposed to this condition. Until recently, chylothorax was thought to be due to TD rupture secondary to trauma. However, other documented causes of chylothorax in the cat include mediastinal neoplasia (lymphosarcoma, thymoma), cardiomyopathy, heartworm infection, and in many cats the underlying etiology is undetermined (idiopathic chylothorax). Because the treatment of this disease varies considerably depending on the underlying etiology it is imperative that the clinician identify concurrent disease processes prior to instituting definitive therapy.
History and clinical findings
The most common presenting clinical sign in cats with chylothorax is dyspnoea. The owners often report that the animal has had rapid heavy breathing, exercise intolerance, and lethargy for months and may have been treated for nonspecific respiratory problems without improvement prior to the diagnosis. The dyspnoea in cats with chylothorax, as in other types of pleural effusion, is usually marked by a forceful inspiration with what appears to be a delayed expiration, as though the cat is ‘holding its breath’. Interestingly, many of the owners report that the first abnormality they noted was coughing. Coughing, although not typically associated with pleural effusion of non-cardiac origin, appears to be a common finding in chylothorax. Most cats with chylothorax present with a normal temperature, unless extremely excited or severely depressed. Cats with elevated temperatures should be evaluated for the presence of pyothorax, rather than chylothorax. If the cat has had previous thoracocenteses, secondary bacterial infections of the chyle may be superimposed.
Diagnosis
If the cat is not overtly dyspnoeic thoracic radiographs should be taken to confirm the diagnosis of pleural fluid. During radiographic procedures, minimising manipulation and stress by performing dorsoventral (rather than ventrodorsal views), and ‘standing lateral’ views may be necessary to prevent further compromise of respiration. Supplementing oxygen by face mask during the procedure may also be beneficial. In the severely dyspnoeic cat it is best to remove some fluid by needle thoracocentesis before taking radiographs. Fluid recovered should be placed in an EDTA tube for cytological examination. Placing the fluid in an EDTA tube rather than a ‘clot-tube’ will allow cell counts to be performed. Triglyceride and cholesterol levels should be performed on both the pleural fluid and serum for comparison. Fluid should also be submitted for culture and sensitivity. The presence of pleural fluid will often prevent satisfactory visualisation of the structures of the thoracic cavity on radiography. Adequate visualisation of the entire thorax is necessary in order to rule out anterior mediastinal masses such as lymphosarcoma or thymoma. If ultrasonagraphic capabilities are present, they should be performed prior to removing large quantities of fluid because the fluid acts as an ‘acoustic window’ enhancing visualisation of thoracic structures.
Chylous fluid is a white or pinkish, opaque fluid in which a cream layer will form when left to stand. When centrifuged, chylous fluid will not clear (versus an exudate with a high cellular content, such as a pyothorax), and chylomicrons can usually be seen on smears. The predominant cell type in feline chylothorax is the lymphocyte, however, higher neutrophil counts than lymphocyte counts may be seen and should not preclude the diagnosis of chylothorax. The most objective way to identify chyle is to measure the triglyceride content of the pleural fluid and compare it to that of serum. Chylous fluid will have a higher triglyceride content than serum.
Medical management
The goal of medical management of animals with chylothorax is to provide the nutritional and metabolic needs of the patient until the effusion spontaneously resolves. Thoracocentesis and dietary management are the main components of medical therapy. Generally, meeting the animal's caloric needs by feeding a low-fat diet such as R/D or a homemade diet is adequate. Benzopyrones (ie, Rutin) may be beneficial in promoting resorption of pleural fluid in animals with chylothorax (Rutin B 50–1000 mg/kg; TID; PO).
Surgical management
Surgical intervention is warranted in cats that do not have underlying disease and in whom medical management has failed. Unfortunately, surgical therapy of this disease in the cat is often unrewarding. I have had poor results in cats with TD ligation. Therefore, I am currently recommending that both TD ligation and a shunting procedure (either mesh installation in the diaphragm or a pleuroperitoneal shunt) be done. With increased experience we may find that shunting is more successful than TD ligation.
The standard approach for TD ligation in the cat is a left intercostal thoracotomy. This approach is recommended when TD ligation and placement of a pleuroperitoneal shunt is being performed. However, when mesh is being placed in the diaphragm, a midline celiotomy and transdiaphragmatic approach to the TD allows both procedures to be performed through the same incision.
Diary
If you are holding a feline meeting and would like to publicise it further, please send details to: Claire Bessant, JFMS, Taeselbury, High Street, Tisbury Wiltshire SP3 6LD, UK. Fax: +44 (0)1747 871873. E-mail:
October 6 1999
Title: FAB Conference
Location: Newbury Race Course, UK
Contact: FAB, Taeselbury, High Street, Tisbury, Wiltshire SP3 6LD
Tel: +44 (0)1747 871872
Fax: +44 (0)1747 871873
e-mail:
October 7–10 1999
Title: 45th Annual Meeting of the German Small Animal Veterinarians (FKDVG)
Location: Giessen, Germany
Contact: DVG-Geschäftsstelle, Frankfurter Str. 89, D-35392 Giessen, Germany
Tel: +(49) 641 24466 or 641 702 4900
Fax: +(49) 641 25375
October 14–16 1999
Title: Annual Congress of the European Society of Veterinary Internal Medicine (ESVIM) and affiliated societies (ESCG, ESVC, ESVNU, ESVCN, ESVONC)
Location: Peruggia, Italy
Contact: Marian Blom, ESVIM Congress Secretary, PO Box 80, 154, 4508 TD Utrecht, The Netherlands
Tel: + 31 30 253 1589
Fax: +31 30 251 8126
e-mail:
October 16–19 1999
Title: Feline Meeting. Fall 1999
Location: Doubletree Hotel, Nashville, Tennessee, USA
Contact: AAFP, 2701 San Pedro NE, Suite 7, Albuquerque, NM 87110, USA
Tel: +1 505 8882424
Fax: +1 505 8882688
e-mail:
ESFM study day GERPAC/AVEPA Conference, Barcelona
October 21 1999
Reproduction in the queen: Stefano Romagnoli
Immunology and epidemiology: Craig Green
Haematology of the kitten and pregnant queen: Urs Gieger
Behavioural evolution of the kitten: P Pageat
Veterinarians in breeding establishments: Ch Dumon
Round table discussion on reproduction: chairman Tim Gruffydd-Jones, European Society of Feline Medicine
Information on the study day and whole congress is available from the Congress office: Inter-Congress, Maignon 50, 08024 Barcelona, Spain.
Tel: 34 93 21 34 447
Fax: 34 93 21 06 698
e-mail:
One day in the general programme (Friday October 22 1999) will also be devoted to feline medicine.
October 27 1999
Title: Feline Viral Diseases
Location: Taunton, Somerset, UK
Contact: Steve O Shea, The Veterinary Hospital, Colwill Road, Estover, Plymouth, Devon PL6 8RP
Tel: 44 (0) 1752 702646
Fax: 44 (0) 1752 773305
e-mail:
October 1999
Title: Feline Diabetes
Location: Verona, Italy
Contact: Stefano Romagnoli
Tel: 39 050 570.308/542.331
Fax: 39 050 542.892
e-mail:
November 11 1999
Title: Recent Advances in Feline Viral Diseases
Location: Daresbury Park, Warrington, North West UK
Details: Mrs Christine Ding, 63 London Road South, Poynton, Stockport, Cheshire SK12 1LA
Tel: 44 (0) 1625 859019
Fax: 44 (0) 1625 850544
December 5 1999
Title: Management of Urinary Tract Disease
Location: Cambridge, South East UK
Contact: Dr Caroline Manser, Centre for Small Animal Studies, Animal Health Trust, Lanwades Park, Kentford, Newmarket, Suffolk CB8 7UU
Tel: 44 (0) 1638 552700
Fax: 44 (0) 1638 555600
December 12 1999
Title: Small Animal Medicine Opthalmology
Location: Athens, Greece
Contact: University of Georgia, College of Veterinary Medicine
Tel: (706) 542 1451
Fax: (706) 542 8254
e-mail:
January 15–19 2000
Title: The North American Veterinary Conference
Location: Orlando, FL, USA
Contact: The North American Veterinary Conference Registration Headquarters
Tel: US & Canada 800 756 3446
Tel: International 617 749 1126
Fax: 617 749 0791
Home page: http://www.afn.org/∼henavc/
February 6–8 2000
Title: Ski 2000—feline meeting
Location: Olympoa Park Hotel and Conference CentrePark City, Utah, USA
Contact: AAFP, 2701 San Pedro NE, Suite 7, Albuquerque, NM 87110, USA
February 20–24 2000
Title: Western Veterinary Conference
Location: Las Vegas, NV, USA
Contact: Western Veterinary Conference, 2425 East Oquendo Road, Las Vegas, NV 89120, USA
Tel: (702) 739 6698
e-mail:
Home page: http://www.wvc.org/
March 11 2000
Title: Feline medicine
Location: University of Liverpool, Leahurst, UK
Contact: The Continuing Professional Development Unit, Faculty of Veterinary Science, Leahurst, Neston CH64 7TE.
Tel: 0151 794 6016
Fax: 0151 794 6005
e-mail:
April 6–9 2000
Title: Annual Congress of the British Small Animal Veterinary Association (BSAVA)
Location: Birmingham, UK
Contact: BSAVA, Kingsley House, Church Lane, Shurdington, Cheltenham, GL51 5TQ
Tel: +(44) 1242 86 994
Fax: +(44) 1242 86 3009
e-mail:
Home page: http://www.bsava.ac.uk
April 24–29 2000
Title: Congress of the World Small Animal Veterinary Association (WSAVA)
Location: Amsterdam, The Netherlands
Contact: Dr H Myer, The Netherlands Association for Companion Animal Medicine, PO Box 9386, NL 3506, GJ Utrecht, The Netherlands
Tel: +(31) 343 200 39
Fax: +(31) 343 200 39
April 25–29 2000
Title: 25th WSAVA–FECAVA World Congress, organised in conjunction with the Voorjaarsdagen of the Netherlands Association for Companion Animal Medicine
Location: Amsterdam, The Netherlands
Contact: Royal Netherlands Veterinary Association, PO Box 14031, 3508 SB, UTRECHT, The Netherlands
Attn: Majolijn Fijten/Linsey Sterkenburg
Tel: +31 30 2510111
Fax: +31 30 2511787
e-mail:
ESFM Membership

Nominations for the ESFM Executive Committee
ESFM President Marian Horzinek will stand down at the AGM in April 2000. Nominations for President should be recieved by September 1999 to be published in the December issue. Nominations should be sent to ESFM, Taeselbury, High Street, Tilsbury, Wiltshire SP3 6LD, UK.
ESFM BOARD OF REPRESENTATIVES
(Treasurer)
Tierklinik Leonding
Mayrhansenstrase 21A
A-4060 Leonding, AUSTRIA
186 rue de l'Eglise
1640-Rhode Sainte Genese, BELGIUM
Falstersvej 9
DK 2000 Frederiksberg
DENMARK
Tel: +388 84777
Fax: +388 85777
Kissaklinikka Felina
Tyomiehenkatu 4C
00180 Helsinki, FINLAND
Tel: 358 09 6852288
Fax: 358 09 6852299
85 ter Bd Soult
75012 Paris, FRANCE
Tel: 33 1 43436344
Fax: 33 1 43473791
e-mail:
Medizinische Tierklinik
Veterinasse 13
8000 Munchen 40, GERMANY
Tel: 49 89 21802697
Fax: 49 89 21806240, e-mail:
Universitat Leipzig
Inst fur Vet Pathologie
Margarete-Blank Str 4
04103 Leipzig, GERMANY
Tel: 49 341 9738271
Fax: 49 341 9738299
Biogdanfy u 7B/22
H-1117 Budapest, HUNGARY
University College Dublin
Faculty of Veterinary Medicine
Dept. of Small Animal Clinic Studies
Veterinary College
Ballsbridge, Dublin 4, IRELAND
Tel: 353 1 66 87988
Fax: 353 1 66 75401
e-mail:
Dipartimento di Clinica Veterinaria
Viale delle Piagge 2, 56124 Pisa, ITALY
Tel: 39 050 570.308/542331
Fax: 39 050 542892
e-mail:
Dipartimento di Patologia Animale
Universita di Torino
Via Nizza 52, 10126 Torino, ITALY
Tel: 390 11 6688769
Fax: 390 11 8174325
e-mail:
Associate Professor
Virology Unit, Veterinary Faculty
Utrecht University, de Uithof
Androclusgebouw
Yalelaan 1, 3584 CL Utrecht
THE NETHERLANDS
Tel: 31 302532487
Fax: 31302536723
e-mail:
Dept Clinical Sciences of Companion
Animals
Veterinary Faculty
Utrecht University, de Uithof
Yalelaan 8, 3584 CM Utrecht
THE NETHERLANDS
Tel: 31 30 2531681 or 1589
Fax: 31 30 2518126
e-mail:
Eidskog Dyreklinikk A/S
2230 Skotterud
NORWAY
Tel: 47 62 835666
Fax: 47 62 836665
e-mail:
Dept of Infectious Diseases
Faculty of Veterinary Medicine
Warsaw Agricultural University
Ul Grochowska 272
03849 Warsaw, POLAND
Tel/Fax: 48 228 104651
e-mail:
Department of Internal Diseases
Veterinary Faculty
Agricultural University of Warsaw
Grochowska 272
03849 Warsaw, POLAND
Tel/fax: 48 22 810 2142
e-mail:
All Russian State Research Institute for Control, Standardization & Certification
5 Zvenigorodskove Shosse
123022 Moscow, RUSSIA
Tel: 7 095 2593546
Fax: 7 095 2531491
State Diagnostics & Prevention Centre for Human and Animal Diseases
42 Timiryazevskaya Street
125422 Moscow, RUSSIA
Tel/Fax: 7 095 2075474
Centro Veterinario
Calle Los Naranjos s/n
Pueblo Lopez
29640 Fuengirola
Malaga, SPAIN
Tel: 34 5 462688
Höjens Gård
S-71692 Fjugesta, SWEDEN
Tel: 46 10 66553495 (mobile)
Veterinarnedizinisches Labor
der Universitat Zurich
Winterthurerstrasse 260
CH-8057 Zurich, SWITZERLAND
Tel: 4 11 16358312
Fax: 4 11 16358906
e-mail:
Tierarzt, Zürcherstrasse 3
Niederglatt 8172, SWITZERLAND
Tel: 4 11 8518070
Fax: 4 11 8548071
e-mail:
(Secretary ESFM)
FAB Lecturer in Feline Medicine
The Feline Centre
University of Bristol, Langford
BRISTOL BS40 5DU, UK
Tel: 44 117 9289280
Fax: 44 117 9289628
e-mail
(SECRETARY/JFMS EDITOR)
The London Cat Clinic
11 Belsize Terrace
London NW3 4AX
Tel: 44 171 704 0984
Fax: 44 171 4314413
e-mail:
ESFM EXECUTIVE COMMITTEE
Director, Insitute of Veterinary Research, Utrecht University, de Uithof, Practicumgebouw, Yalelaan 1, 3584, Utrecht, The Netherlands
Tel: 31 30 253 2485, Fax: 31 30 253 6723
E-mail:
CONTACTING ESFM
Please send letters/articles/comments for JFMS to Claire Bessant, ESFM/FAB, Taeselbury, High Street, Tisbury, Wiltshire, SP3 6LD, England. Tel: 44 1747 871872, Fax: 44 1747 871873 Membership details may also be obtained from this address.
Footnotes
JFMS is included as part of membership on the understanding that the Journal is for the member's use only and not passed on to libraries.