
Abstract
Background
A number of therapeutic strategies have contributed to improved survival rates in patients with acute myocardial infarction (AMI) who survive sufficiently long enough to receive hospital treatment [1].
The initial assessment of patients with chest pain, potentially due to AMI, includes a history and physical assessment, 12-lead electrocardiograph (ECG) and measurement of biochemical markers such as CK, CK-MB, troponins, and myoglobin. The primary therapeutic goals of management for patients with AMI are to promptly restore perfusion to the myocardium and to prevent or limit myocardial cell death. Continuous monitoring of myocardial perfusion status is, therefore, an essential component of ongoing management for patients with AMI. Critical care nurses can have an important role in recognising and monitoring ischaemia.
Traditionally, the 12-lead electrocardiograph (ECG) has been used diagnostically to detect myocardial ischaemia or infarction, manifested by changes in the ST-segment and/or T-wave. Q-wave development and R-wave loss may also be present. The 12-lead ECG is the single-most important source of data in the assessment of patients with potential AMI. However, ECG changes indicating AMI may not be immediately apparent at the point of hospital admission. Furthermore, in the early stages of myocardial ischaemia and infarction, the ST-segment and T-wave undergo dynamic changes, which may not be captured by single or intermittent serial ECGs [2]. Obtaining serial standard ECGs can be time-consuming and erratic, and important trends in ST-segment and T-wave changes may be missed.
The role of ST-segment monitoring
Rather than relying upon a series of ECG ‘snapshots’, ST-segment monitoring (and concurrent T-wave monitoring if it is available) provides a continuous method for monitoring changes in myocardial perfusion over time. Simultaneous angiographic studies have demonstrated that early reduction in ST-segments by ≥50% in the first 2 h post thrombolytic therapy is a good predictor of reperfusion [3–5]. Continuous ST-segment monitoring, therefore, is a non-invasive method for monitoring of infarct-related artery patency/re-occlusion and myocardial tissue perfusion [3].
ST-segment monitoring is available in most current models of cardiac monitoring equipment, although functionality varies with different systems. Systems may utilise full 12-lead ST-segment monitoring, or derived leads. Some ST-segment monitoring systems offer additional features such as continuous T-wave and QRS monitoring. Stand-alone ST-segment monitors are also available, and so continuous ST-segment monitoring is accessible to smaller hospitals such as those in rural areas that may not have facilities for angiography or more comprehensive cardiac monitoring systems [6].
The value of ST-segment monitoring in the initial evaluation of acute myocardial infarction
Thrombolytic therapy has been shown to improve in-hospital and long-term survival in patients with AMI [7,8] by restoring patency to the infarct-related artery. The goal of thrombolysis is to restore myocardial perfusion (TIMI 3 grade flow to the infarct-related artery with associated full tissue perfusion) within 60–90 min. TIMI 3 grade flow to the infarct-related artery post thrombolysis has been associated with improved survival, when compared with TIMI 2 and 0/1 grade flow, as well as decreased incidence of congestive cardiac failure, recurrent ischaemia and improved left ventricular ejection fraction [9]. Continuous ST-segment monitoring can be utilised to predict coronary artery patency: a reduction of ST-segments by ≥50% has been associated with patency of the infarct-related artery in several studies [3–5,10–13]. It should be noted, however, that myocardial tissue may be perfused by collaterals to varying degrees [13–16], which may result in the reduction of ischaemia and the reduction of ST-segment elevation in the presence of continued coronary artery occlusion.
Coronary angiography is the ‘gold standard’ for direct visualisation of epicardial coronary artery patency. However, the assessment of thrombolytic efficacy by coronary angiography soon after thrombolysis is costly, carries an inherent risk of bleeding and is not available at all institutions. Furthermore, coronary angiography is not an indicator of the stability of reperfusion: coronary angiography only provides a ‘snapshot’ view of the coronary artery, whereas thrombolysis is a dynamic process resulting in episodes of cyclic patency/occlusion of the infarct-related artery in up to 25–50% of patients [15–18], which will not be captured in entirety during angiography [19].
Importantly, coronary angiography does not necessarily reflect the adequacy of tissue perfusion. The nature of failed or slow tissue reperfusion is not constant, in that non-reperfusion may be due to continued coronary artery occlusion, but in some cases, it may be due to the ‘no re-flow’ phenomenon through a recanalised infarct-related artery. Epicardial coronary artery patency does not guarantee microvascular flow [20]. Perfusion at the myocardial tissue level can be assessed more directly by serial 12-lead electrocardiograph (ECG) or continuous 12-lead ST-segment monitoring: continued ST-segment elevation=continued myocardial ischaemia.
Identifying failed reperfusion
It has been reported that reperfusion fails to occur at any stage in approximately 25% of patients and in 50–70% of patients at 90 min after thrombolytic administration [21,22]. Furthermore, only 25–40% achieve normal perfusion; a number of patients have incomplete tissue perfusion despite a patent infarct-related artery [23]. Overt or silent re-occlusion of the infarct-related artery is also a problem, with approximately 10% of patients re-occluding in-hospital after thrombolytic therapy: this has been shown to double early in-hospital mortality rates [24].
It is not entirely clear why some patients fail to reperfuse with thrombolytic therapy. There are a number of proposed mechanisms for the failure of thrombolysis, including thrombolytic resistance or failure to reach a ‘lytic state’ [25], thrombus composition with exposed activated thrombin resulting in a prothrombotic state, mechanical factors such as arterial pressure proximal to the occluding thrombus, myocardial wall tension, thrombus burden [26], lesion complexity [27], residual stenosis and the presence of sub-intimal haemorrhage [28] contributing to impaired reperfusion.
It is, therefore, necessary to assess the efficacy of thrombolytic administration in individuals with AMI as they may benefit from incremental pharmacological or invasive perfusion strategies [29,30].
Conclusions
It is essential that critical care nurses recognise the dynamic nature of AMI and monitor for acute changes in the ischaemic status of such patients so that rapid and appropriate intervention is given. ST-segment monitoring is an accurate, non-invasive and continuous method of assessing myocardial tissue perfusion in patients who survive to reach hospital with an AMI (see Fig. 1). It is easy to use, readily available, does not involve the potential risks and costs associated with coronary angiography. This type of monitoring should be initiated at the earliest opportunity on all patients with a probable or definitive diagnosis of AMI who are likely to receive an intervention that is designed to restore myocardial perfusion to optimise treatment.
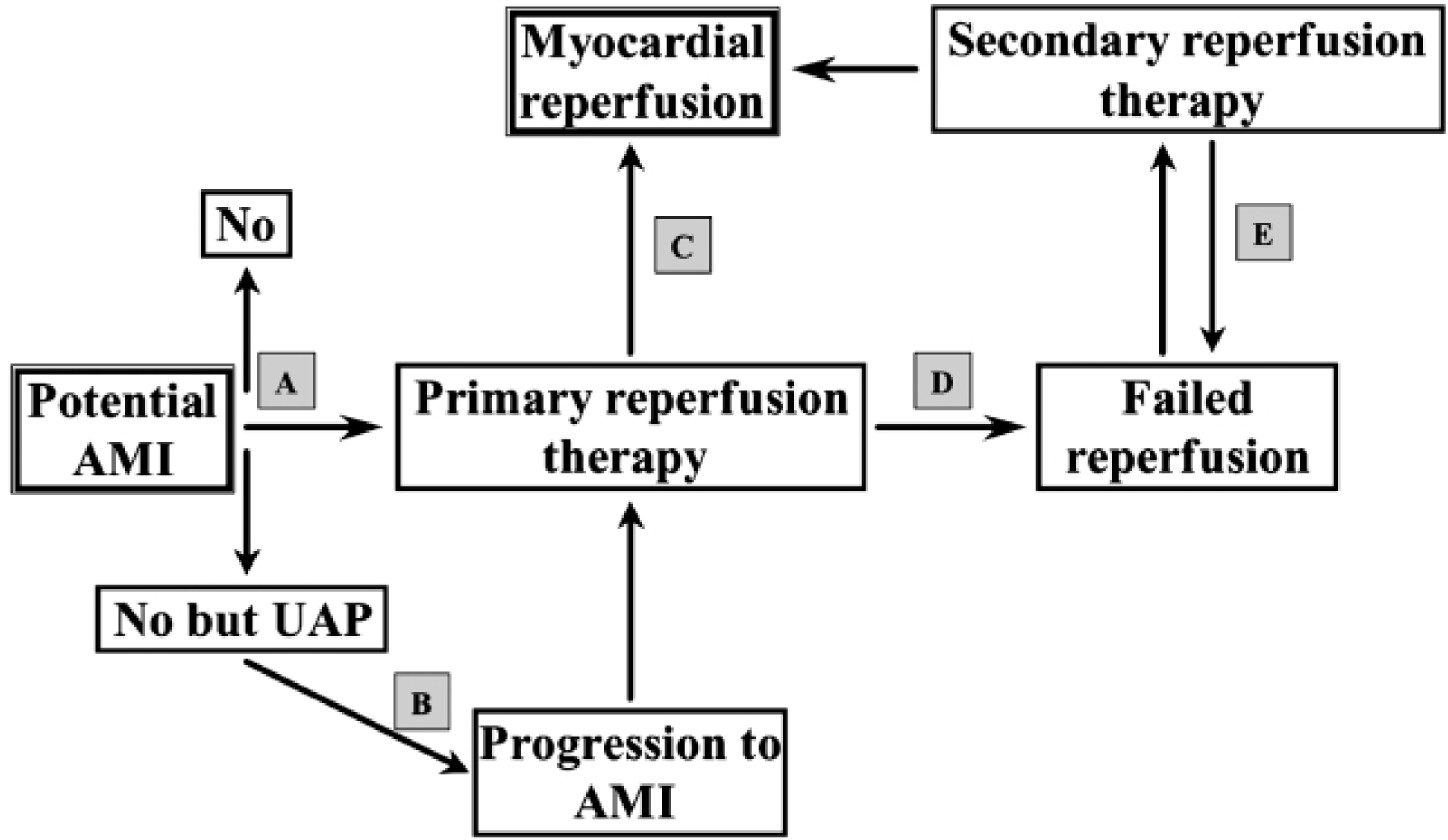
A. ST-segment monitoring facilitates determination of an accurate diagnosis (e.g. non-cardiac chest pain or an acute coronary syndrome). B. If a patient is being treated for unstable angina pectoris or non-Q-wave myocardial infarction their ischaemic status may worsen suddenly. Continuous ST-segment monitoring often detects such progression in the absence of other signs and symptoms (e.g. silent AMI with sudden elevation of ST segments). C. In addition to detecting worsening myocardial ischaemia, it also enables a rapid evaluation of the success of primary reperfusion therapy (e.g. resolution of ST elevation post thrombolytic therapy). D. Conversely, it may also indicate the absence of early ST-segment resolution with the need for ‘rescue’ intervention (e.g. sustained ST elevation in anterior-lateral ECG leads despite initial thrombolysis managed with a rescue angioplasty). E. As with C and D, ST-segment monitoring is useful in determining the success of treatment in those patients who initially failed to reperfuse (e.g. patients who experience recurrent ischaemia following a ‘rescue’ angioplasty and require further treatment). Value of ST-segment monitoring in providing optimal management in acute myocardial infarction.