
Abstract
The provision of thrombolysis in a timely fashion is the mainstay of treatment for acute myocardial infarction. With the publication of the National Service Framework (NSF) for Coronary Heart Disease increasing efforts have been put into the reduction of the ‘pain to needle time’. Of the various parts of the patient journey the time delays in hospital are the easiest to resolve. Published research shows that the time taken for the patient to call for help is intractable at present. Therefore, the obvious target for the reduction in the overall time from pain to treatment is the in hospital portion of the delay (the door to needle time). There are several methods that have been recommended for the reduction of the door to needle time. However, the increasing focus on the door to needle time is leading health care providers away from other issues such as the safety and accuracy of assessment by a non-cardiologist. Furthermore, the standards for audit of the door to needle time have not been set by the NSF and this has led to the presentation of selected data and the avoidance of discussing issues of accuracy and appropriateness.
Introduction
The drive for quality in the treatment of acute myocardial infarction (AMI) has recently focussed on the reduction of the door to needle time [1–3]. This focus has been on various methods of reducing the time from the presentation of the patient at the hospital (‘door’) to the initiation of treatment (‘needle’). Many methods have been proposed from the use of protocols [4], moving the site of treatment from the Coronary Care Unit to the Accident and Emergency Department [5] and the use of ‘thrombolysis nurses' [6,7]. What is noticeable from both the current drive for quality in the treatment of the patient experiencing an AMI and the published data is that door to needle times are considered the only measure of quality of care. This blinkered attitude is self limiting and appears to be leading clinicians away from other salient, and equally important, issues surrounding the administration of thrombolysis such as the appropriate use of thrombolysis. That is, whether thrombolysis is being inappropriately administered to patients not experiencing an AMI and whether patients experiencing an AMI are not receiving thrombolysis, either due to misdiagnosis or because of inappropriate exclusions. Furthermore is the drive for the faster administration of thrombolysis leading to an exacerbation of these problems?
Despite the fact that the standard mortality ratios for heart disease have been falling by approximately 4% per year since the 1970s coronary heart disease (CHD) is still the largest cause of death in Britain [8]. Government initiatives have been targeting heart disease in the UK for several years. The white paper ‘Saving Lives. Our Healthier Nation.’ [9] set forward targets for reducing the mortality from CHD by 40% by the year 2010. The present figures from the British Heart Foundation seem to suggest that the target will be met (and may even be surpassed) if the current trends continue. However, the overall figures for the nation do hide the fact that most of the reduction in CHD is occurring in the sub group of 35–44-year-old men, and not in what is commonly perceived as the highest risk sub-group of 45–64-year-old men.
The decline in mortality is falling much slower in those over 65 and in women of all ages. This slower decline is of interest as both these groups have been identified in prior studies as those less likely to receive thrombolysis or to have a longer symptom onset to treatment time [10,11]. Thus, there is the possibility that the introduction of thrombolysis is the main cause of reduced coronary mortality. However, this is at present, mere speculation and cannot be proven. Whilst at first glance the picture is encouraging the evidence supporting this is at best incomplete and often tenuous.
Door to needle times: the drive for quality
The National Service Framework (NSF) for Coronary Heart Disease [12] is an integral part of the government plans to modernise the NHS. The first indication of this drive came in the 10-year plan set out in the white paper ‘The New NHS. Modern. Dependable.’ [13]. This put forward the need to modernise the NHS and bring care up to a standard that could be recognised as best practice. Following this the Department of Health published ‘A First Class Service’ [14] setting out the framework by which the modernisation and standard setting would be carried out. In the area of cardiology the emphasis on effective, efficient delivery of care and health outcomes of care can easily be applied as performance markers for the use of thrombolysis and in particular the speed with which it is delivered.
In Section 1, the NSF states that it is setting out best practice, based on the best evidence. This is held up as the standard that all hospitals will be expected to achieve. In this way, the NSF is intended to remove the regional variations in care by bringing all hospitals to a similar standard of care for the patient with CHD. Whilst this is a laudable aim, we must ensure that it is indeed best evidence that informs the basis for change.
The NSF highlights door to needle times for thrombolysis as an area for improvement in many Trusts. The framework states that the hospital environment is the best place to administer thrombolysis unless local emergency transportation means that there would be unacceptably long delays in the provision of treatment. The NSF also states that the call to needle time should not be longer than 60 min, with a door to needle time of less than 30 min (with a further reduction to 20 min by 2003). This aim for a reduction in the time between the call for help and the door of the hospital is an area that is not proving amenable to large reductions [15], an issue compounded by difficulties in the accurate measuring and reporting of data. However, several initiatives have been carried out into pre-hospital thrombolysis, pooled data presented by Habib [16] suggests that the mortality benefit in the urban setting is small (all cause mortality benefit 1.78%). Therefore, the focus in reducing overall time to treatment has not been on the ‘call to needle time’ but rather the ‘door to needle time’ [15].
Government white papers in the last few years have focussed on the measurement of quality improvement by the use of targets. Health care trusts are expected to show that they are meeting the government targets, or at least making improvements in a clear drive to attain the required target. Much of the work published by government agencies in the last few years has focussed on this related to the concept of clinical governance. The Department of Health states that one of the main components of clinical governance is ‘Ensuring the clinical standards of NSFs and NICE recommendations are implemented.’ [17]. The NSF for CHD, when discussing AMI, focuses on the use of thrombolysis as the treatment of choice. It is therefore helpful to consider the reason that thrombolysis has become the standard treatment in the UK.
The treatment of acute myocardial infarction
Treatment options are based on the seminal work of DeWood et al. [18] which found that more than 85% of patients have an occlusive thrombus in the infarct related artery at 3 h. The aim of modern treatment is to gain patency in the infarct related artery (the open artery theory). This theory associates early and complete coronary perfusion with improved clinical outcome [19].
Conservative treatment is almost always reserved for those incidents where thrombolysis or PPTCA is either contra indicated or unavailable. The use of acute anticoagulation such as heparin in AMI is now only routinely used as an adjunctive therapy to thrombolysis with tissue plasminogen activator [20].
Thrombolysis has therefore been established as the most common treatment for AMI in the western world, and it is estimated that treatment with thrombolysis and aspirin can reduce 1-month mortality in patients with myocardial infarction by 50% [21]. The analysis of all trials of greater than 1000 patients by the Fibrinolytic Therapy Trialists Collaborative Group [22] gave a mortality reduction of 30 lives saved per 1000 patients treated and this number can be doubled when aspirin is used concurrently. Furthermore, the mortality benefits of thrombolysis may be carried on for at least 5 years after the initial event [23].
Although the absolute and relative benefits of thrombolysis are variable between different subsets of patients the treatment is of value for all patients, without contra indications. This is regardless of age, sex, site of infarction, whether this is the first AMI or a subsequent event, regardless of previous history of bypass surgery and across a wide range of blood pressures and heart rates [22].
Thrombolysis has universally offered a greater hope of full recovery from AMI than any other treatment, however, the mortality gain is, to some extent, off set by the incidence of stroke and major bleeds that can occur as a result of the administration of the treatment. The exact incidence of these complications is dependent on the type of thrombolytic agent used and the demographics of the patient group [24]. However, the mortality benefit of all types of thrombolysis in the first 6 h after the onset of symptoms far outweigh the relative risk of major complications in patients without contra indications to treatment [24].
Primary percutaneous transluminal angioplasty (PPTCA) is the opening of the infarct related vessel using balloon dilatation in the cardiac catheterisation laboratory during the acute phase of a myocardial infarction, within the first 6 h after the onset of symptoms. This procedure has been found to be a better treatment for acute MI due to its relative reduction in the incidence of major bleeds and stroke, and improved outcomes. The GUSTO IIB trial [25] found that disabling stroke occurred in 0.8% of patients receiving tPA vs. 0.2% in patients who underwent PPTCA.
With the gains in morbidity and mortality it must be asked why PPTCA is not the treatment of choice in the UK. The use of angioplasty in the treatment of AMI requires the presence of skilled staff 24 h a day. The financial burden of this can be seen as prohibitive to most hospitals in the UK where healthcare is funded by a system of taxation rather than medical insurance. Furthermore the trials into PPTCA have all been carried out in tertiary centres where there is a high volume of procedures being carried out, thus skill levels are maintained. One trial of PPTCA in a non-tertiary centre showed no benefit of PPTCA over thrombolysis [26]. Whereas Aversano et al. [27] has shown a benefit in the use of PPTCA in the community hospital setting (however, the confidence intervals were quite wide—OR 0.57 (95% confidence intervals 0.34–0.95)), however, the protocol for medical staff participating in this study stated that they must undertake 50 procedures a year in order to perform PPTCA. Furthermore, both technical and nursing staff underwent a period of training thus adding to the financial burden.
Thrombolysis is easy to administer (after comparatively little training) and requires no specialist equipment, other than the standard cardiac monitoring provision. Thus in a rationalised health care setting thrombolysis gives the greatest benefit per pound per patient.
Why the call for reduced door to needle times?
Studies in animal models have shown that the duration of coronary occlusion and the extent of collateral circulation are the main determinants of infarct size [28]. In the acute setting the extent of collateral circulation is not a variable that can be altered, however, the duration of coronary occlusion is.
Early thrombolysis trial data (administration <2 h after the onset of symptoms) show that there is a large benefit of administering thrombolysis as early as possible. The United Kingdom Heart Attack Study Collaborative Group [29] found that there was a 50% reduction in mortality in those patients who received thrombolysis within 2 h of symptom onset compared with those who received thrombolysis after this time period. The Fibrinolytic Therapy Trialists Collaborative Group [22] carried out a meta analysis of all trials of thrombolysis involving more than a 1000 patients. The analysis of these data showed that for every 1000 patients treated 65 lives would be saved if thrombolysis was administered within 1 h, 37 lives would be saved if the time interval was 1–2 h and 26 lives if the time interval was 2–3 h.
This combination, of the findings from animal models and the data from trials of early thrombolysis, points to a large benefit in the administration of thrombolysis as early as possible after the onset of symptoms, thus making the reduction of time to treatment in AMI probably the patients best chance of survival.
Driving down the door to needle time
Many papers have been published summarising successes in driving down the door to needle time. A selection of these data are given in Table 1. The method of reducing the door to needle time varies from project to project. However, what is common between all these papers is the emphasis on the door to needle time as the main measure of success.
Published door to needle times
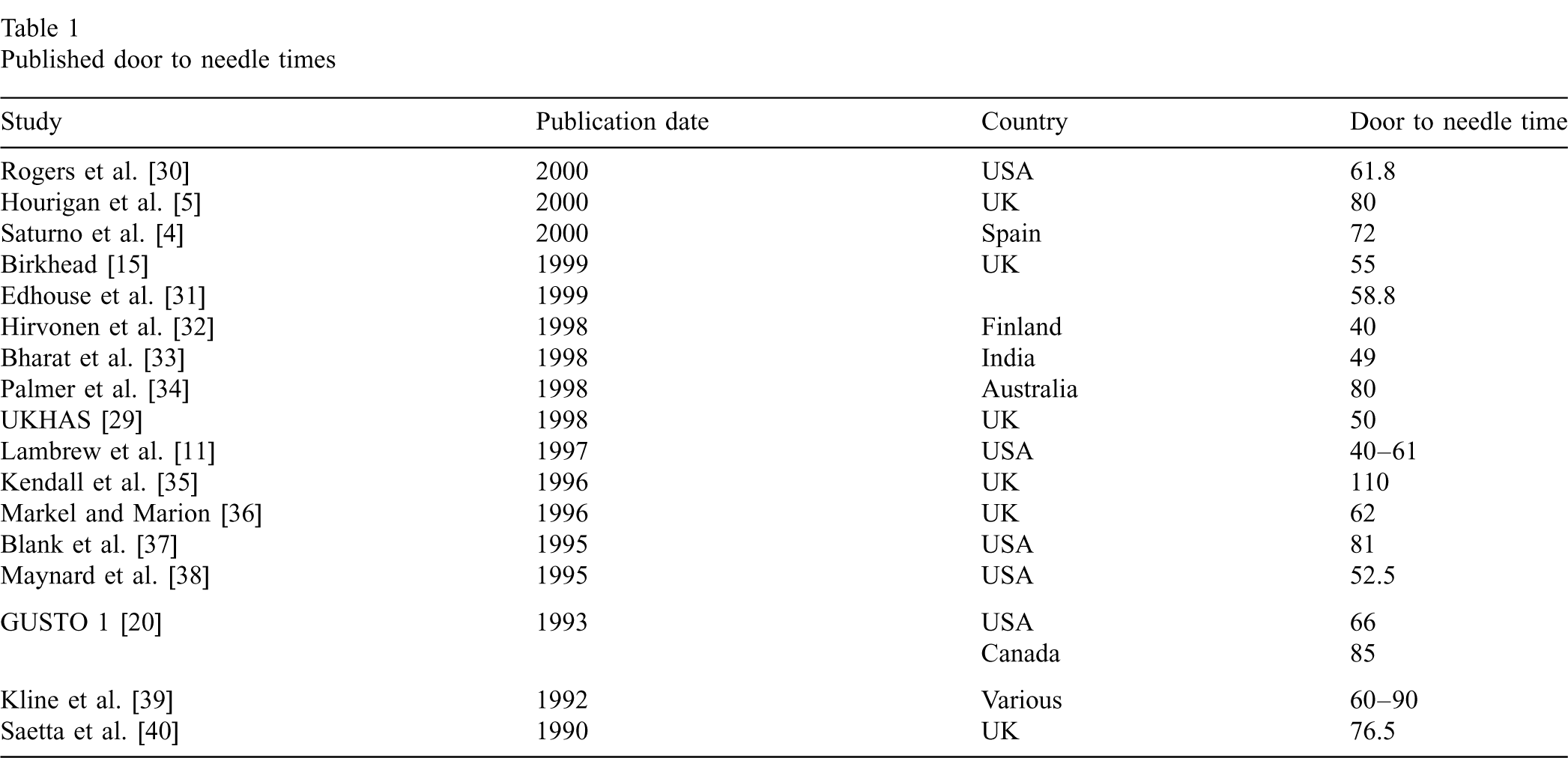
Published door to needle times
The emphasis on door to needle times is obscuring an important issue in thrombolysis use—the appropriate administration of thrombolysis. Most published audits of thrombolysis, and many research studies of door to needle times, do not give data as to the usage of thrombolysis in the appropriate patient. That is, the proportion of patients eligible for thrombolysis who do not receive it and the proportion of patients who receive thrombolysis but are not experiencing an AMI. In either instance the patient may suffer severe clinical consequences.
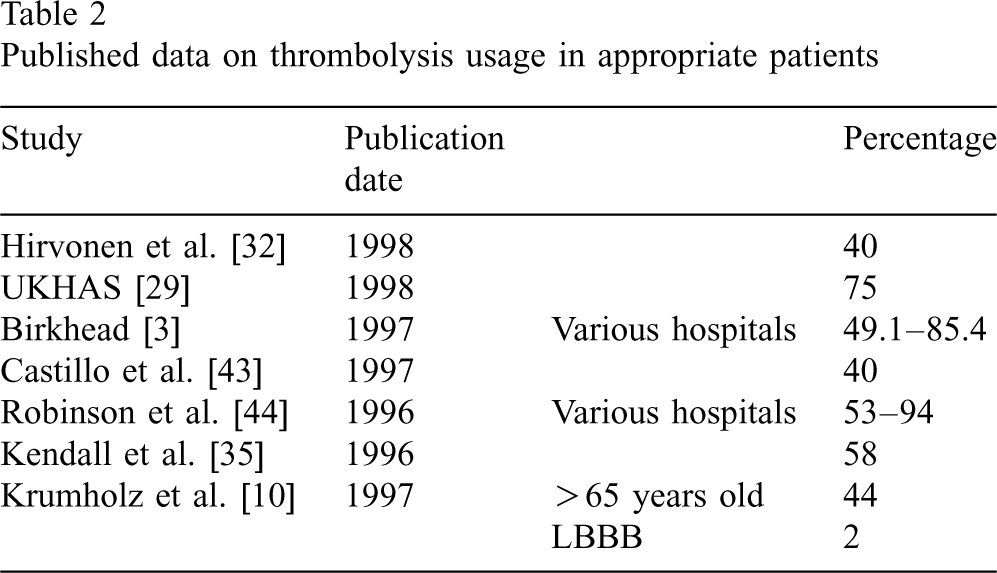
The question of the patient who is wrongly diagnosed is an issue that cannot be ignored in the quest for shorter door to needle times. As can be seen from the data from the published trials many patients who are eligible for thrombolysis are not receiving the appropriate treatment (Table 2). In some cases this will be due to the misdiagnosis of the patients' condition (Pope et al. [41], state that in the United States an estimated 11 000 cases of myocardial infarction are missed each year). Whereas others will be the result of treatment not being given due to hospital policy excluding certain types of patient. Lambrew et al. [42] found that just over 34% of hospitals surveyed had protocols that excluded thrombolysis in those over 75 years of age.
Published data on thrombolysis usage in appropriate patients
There is also the fact that many doctors are simply unaware of the recommendations on thrombolysis in certain sub groups of patients. In one study Krumholtz et al. [10] found that of patients over 65 years of age who were eligible for thrombolysis less than half (44%) were given the treatment. Advanced age was found to be an independent predictor of the non-use of thrombolysis (odds ratio 0.91). Of the patients (over 65 years of age) not given thrombolysis only 19% had a reason written in the notes, this is patently not a defensible position for a hospital, or individual practitioner, to find themselves in. Of this 19% ‘advanced age’ was given as a reason in 20%; one patient even had ‘female sex’ given as the reason for non-use of thrombolysis. These data establish a worrying trend of clinical ignorance (and/or naivety) in spite of the European Society of Cardiology and American College of Cardiology/American Heart Association guidelines stating that thrombolysis should be given to those over the age of 75 (without contra indications) as the mortality from myocardial infarction is greater than the risk of complications [2,45]. The authors also note that only 2% of eligible patients presenting with left bundle branch block (LBBB) were given thrombolysis, suggesting an inability to diagnose AMI on non-classical ECG presentations.
Reviewing the evidence there is a risk that, as the drive for faster thrombolysis times becomes a higher political priority, the inappropriate use of thrombolysis may become greater. Most studies do not publish the data showing how many patients were given thrombolysis inappropriately but it certainly does happen (although at present this assertion is only supported by small amounts of anecdotal evidence). Lloyd et al. [46] found that 73% of patients given thrombolysis in their hospital did not have a diagnostic ECG. However, they do not state how many of these patients were later found to have been experiencing an AMI.
Whilst it is increasingly important to aim for the maximum benefit from thrombolysis the drive for shorter door to needle times may actually be resulting in increased rates of inappropriate thrombolysis and/or missed diagnoses. Al-Mohammad et al. [47] found that a drive to reduce door to needle times in their hospital was associated with the inappropriate administration of thrombolysis in 24% of cases, however, this was a small study (n = 127), unfortunately the inappropriate administration rate before the initiative was not reported. Kelion et al. [48] found that the introduction of an aggressive policy to reduce door to needle times was associated with a 16% increase in the rate of inappropriately thrombolysed patients (from 11 to 27%). Hourigan et al. [5] found that the mortality rate for emergency department thrombolysed patients was 12% compared with 3.4% for CCU thrombolysed patients. They go on to say that this could be a type 1 error or part of a learning curve as the next trache of patients had a mortality rate of 6%. This could be explained by the accident and emergency staff becoming more conservative in the use of thrombolysis or transferring complicated patients to the CCU for management. In the absence of definitive data, however, this can only be surmise.
The rate of missed infarctions is also a subject that is not widely discussed in the literature. There is real concern from some authors that patients with a definitive diagnosis of AMI are being missed by accident and emergency staff or not given thrombolysis for inappropriate reasons. Chan et al. [49] found that in one accident and emergency department 27% of all patients with a discharge diagnosis of myocardial infarction were misdiagnosed on admission in accident and emergency. Of these 34.8% (~15 patients) had definite ECG changes that would indicate thrombolysis was necessary. Pope et al. [41] analysed data from 10 hospitals in the United States and found that of 10 689 patients presenting to the emergency department with chest, neck and jaw or arm pain 55% did not have a cardiac problem. However, 8% (894) of patients were experiencing an AMI, of these patients 5 self-discharged and 19 (2%) were discharged inappropriately without treatment. However, the context of care in this study is not easily translatable, in the United States there is no NSF and nor do they have the problems of chronically under staffed and over worked accident and emergency departments. If the rate of inappropriate discharge is 2% in the US then what is the rate in the UK, where government drives compound the issues. In total, of the 894 patients with myocardial infarction, 2 patients with diagnostic ST elevation on the ECG were discharged without proper treatment. This does not seem as high as the missed diagnosis rate in other studies but it must be remembered that this study was looking at the inappropriate discharge of patients and did not include those patients who were misdiagnosed but admitted to hospital.
In recent years there has been a growing recognition that the accident and emergency departments in England and Wales have become over crowded, under staffed and under resourced [50]. This may have a dramatic impact on the diagnosis and care of the patient suffering from an AMI. There is a danger that the rates of missed diagnosis, inappropriate treatment and mortality will increase as staff are put under increasing pressure to cope with a larger, sicker population.
In the light of this there seems to be a reasonable argument for the extension of required audit data. This should include data on missed diagnoses and inappropriate administration. The drive to reduce the door to needle time may be, at times, at the cost of accuracy in diagnosis. Lambrew et al. [11] state that emergency departments should be the place for the administration of thrombolysis but there should be third party monitoring of the process. For instance, the cardiology team would be ideally placed to monitor the adherence to a protocol and investigate any clinical incidents. There should also be a training programme put in place to ensure a reasonable standard of ECG interpretation. This call for the use of accident and emergency to be the site for the administration of thrombolysis is repeated in the NSF. The expectation is that 75% of accident and emergency departments will be the main point for the administration of thrombolysis in a hospital. Yet the NSF does not stipulate any controls on the data collected by individual trusts beyond the door to needle times. Within the modern NHS we must look to create a more definitive (and accurate) evidence base, rather than a thin veneer of evidence with no substance.
In conclusion, none of the papers seem to deal with the issue of what happens if the ECG is not obviously diagnostic or if the patient does not conform to the protocol. There should be a little thought put into a system to ensure that those patients who do not conform to the protocol are at least referred straight to a cardiologist or the admitting medical team if the cardiology team is not on call. Thus, though the patient will not have the fastest door to needle time the system will at least ensure that they are not left on the ‘slow track’. The use of protocols may be of use, aiming to ensure a baseline for patient care. However, protocols must not be regarded as a panacea, and indeed if poorly designed or audited they can become a blinker reducing the drive for quality, making everyone think that they have solved the problem.
Thus, in order to ensure that the service provision for patients with AMI is adequate there should not only be an audit of all door to needle times but also audit and regular case reviews to identify if thrombolysis is being used appropriately. However, this has not been specified as an audit requirement in the NSF and is therefore unlikely to be carried out in the majority of hospitals.
Is door to needle time the ‘holy grail’ for cardiology or is it fast becoming an obsession that is leading the professions away from issues of equal importance? If the door to needle time is important how should it be monitored? Should there be a stricter definition of the audit criteria or is improving the door to needle time for those patients with obvious ST elevation a satisfactory target for all?
There is no doubt that thrombolysis is a time sensitive treatment and that the reduction of the time delay from pain onset to the administration of thrombolysis is a matter of concern [12]. The reality (as shown in the discussion of data in this paper) shows that the current interpretation of audit requirements and door to needle standards in the NSF are poorly expressed. This has led to the presentation of data across the country for which there is no guarantee of quality or comparability. Authors are presenting data that only include patients who fit into a defined protocol and have no delays (many audits exclude patients with a delay of any cause). This is hardly comparable data and it should be argued that audits of protocols should not be presented as a hospitals' ‘door to needle’ time but as an audit of the protocol with additional data presented regarding the number of patients who fell out of the remit of the protocol. Therefore, there is a need, if the reduction of door to needle times is not to become an exercise in ‘spin’, to create guidelines for the audit and presentation of door to needle times.
The concentration on door to needle times is becoming the sole focus of many cardiology departments to the deficit of other areas of care. This blinkered attitude is directing attention away from another area of thrombolysis that is important, i.e. the appropriate use of thrombolysis. The concentrated focus on the audit of time has led many to ignore the question of how many patients are receiving thrombolysis inappropriately due to either poor assessment or the as a direct result of the drive for lower door to needle times, and the number of patients who are not receiving thrombolysis who should be. Audits of door to needle times should naturally incorporate the inappropriate use (and non-use) of thrombolysis. It would be especially interesting to evaluate the effect of the introduction of bedside measurement of cardiac specific enzymes (e.g. Troponin I, Troponin T) on rates of missed diagnosis and inappropriate thrombolysis.
The concentration of staff on the patient with the obvious AMI may be leaving staff with the attitude that the problem is solved. This may be leaving those patients who do not fit into the rigid criteria with a second-class system. Those without an obvious infarct or with possible complications are at risk of being left on the ‘slow track’. As developments are created to speed up the door to needle times using protocols, accident and emergency staff and nurses may inadvertently avoid the ‘complicated’ case. Every hospital must look to its provision for all patients with AMI not just the few who fit in narrowly defined protocols. At the same time the work on the door to needle times for those without complications must be applauded, as the service provision for patients in the past has been less than satisfactory in the light of the known time sensitivity of thrombolysis.
Footnotes
Acknowledgements
This paper was developed from original dissertation work done as part of the M.Sc. in Cardiorespiratory Nursing at Imperial College, London.