
Abstract
Background: Guidelines stress the importance of risk factor management in patients with coronary heart disease (CHD). Aims: To evaluate whether guidelines on patient education in risk factor management are followed in clinical practice and to assess the contribution of nursing to risk factor management as perceived by patients with established CHD. Methods: Within three Dutch hospitals consecutive patients were identified after a first coronary–artery bypass graft, a first percutaneous transluminal coronary angioplasty or hospital admission for acute myocardial infarction or ischaemia (n=357). Data were collected through patient interviews at least 6 months after hospital admission. Results: Among smokers, overweight patients, patients with hypertension, high cholesterol, and sedentary lifestyle, respectively 75, 36, 67, 61 and 49% reported that information on presence or management of these risk factors was provided. The proportion of patients informed by nurses ranged from 14% (lowering cholesterol) to 23% (increasing physical activity), while 55% (lowering cholesterol) to 71% (stop smoking) were informed by physicians. Conclusion: Many patients with established CHD and cardiovascular risk factors do not remember ever having received information about management of their risk factors. Clearly, there is a substantial potential to improve professionals’ compliance to guidelines on risk factor management, including those on patient education. The perceived contribution of nurses to risk factor management is small compared to that of physicians and other caregivers. If risk factor management is felt to be a main responsibility of nurses, current nursing activities in this area should be reconsidered within an improved organisational structure.
Introduction
Despite falling age-specific coronary heart disease (CHD) mortality rates in Western European countries the prevalence of patients with established CHD increases, mainly because of ageing populations and the improving prognosis of coronary patients due to more effective treatment [1]. Major objectives of risk factor management in patients with established CHD are to reduce the risk of further coronary and other atherosclerotic events, to increase life expectancy, and to improve quality of life [2]. There is a substantial amount of scientific evidence that these objectives can be achieved through lifestyle changes and use of appropriate prophylactic drug-treatment. On the basis of scientific evidence, the European Society of Cardiology (ESC), the European Atherosclerosis Society, the European Society of Hypertension, and other organisations provided recommendations on prevention of CHD [2]. The goals defined in these recommendations are to stop smoking, to achieve a body-mass index (BMI) less than 25 kg/m2, a blood pressure below 140/90 mmHg, a total cholesterol concentration less than 5.0 mmol/l, to become physically active, and to use appropriate drug-treatment.
To evaluate to what extent recommendations are followed in clinical practice, the ESC initiated the Euro Heart Survey (EHS) programme. During 1995–1996 and 1999–2000 two consecutive surveys, EUROASPIRE I and EUROASPIRE II, were conducted within the EHS programme to evaluate to what extent the recommendations on prevention of CHD are embedded in clinical practice [3,4]. Both surveys showed disappointing results with regard to the management of risk factors. Comparison of the results of EUROASPIRE I and II showed an improvement in drug-treatment, but adverse lifestyle trends among European CHD patients [5]. The prevalence of obesity (BMI⩾30 kg/m2) increased substantially from 25.3% in EUROASPIRE I to 32.8% in EUROASPIRE II, while the prevalence of smoking remained almost unchanged at 19.4 vs. 20.8%. Clearly, there is a substantial potential to reduce the risk of recurrent non-fatal cardiovascular disease and death.
An essential step to achieve the goals as formulated in the recommendations on coronary prevention is to inform patients about their cardiovascular risk factors and possibilities to reduce their risk on cardiovascular events. Increasing patients’ awareness through patient education has been shown to be a crucial factor in promoting a healthy lifestyle and adherence to prescribed medications [6,7]. Although patient education is recommended by guidelines on coronary prevention [2], little is known about whether these guidelines are followed in clinical practice and by whom. In the Netherlands, patients with established CHD are, after hospital discharge, mostly looked after by cardiologists, and general practitioners. Little is known, however, about the actual contribution of general practitioners and cardiologists to management of cardiovascular risk factors, and how often other professional caregivers are consulted. The contribution of nursing to risk factor management is also not clear, although it has been argued that nurses can or should play a role in CHD prevention [2,8,9]. As part of the EUROASPIRE II survey, we evaluated whether guidelines on management of cardiovascular risk factors are followed in clinical practice, and we assessed the current contribution of nurses, physicians, and other caregivers in the management of risk factors.
Methods
Study population
Three hospitals in the region of Rotterdam, the Netherlands, participated in the EUROASPIRE II survey [4]. Within each hospital, consecutive patients (⩽70 years of age at the time of index event or procedure) were identified with the following diagnoses: first elective or emergency coronary–artery bypass graft (CABG), first elective or emergency percutaneous transluminal coronary angioplasty (PTCA) without previous CABG, first or recurrent acute myocardial infarction without previous CABG or PTCA, and first or recurrent acute myocardial ischaemia without previous CABG, PTCA, or myocardial infarction. Between January 1997 and March 1999, a trained research nurse retrospectively identified patients with the use of hospitals’ admission registrations. In two of three participating hospitals, patients were asked by whom the information on management of cardiovascular risk factors was provided.
Data collection
Data on demographic characteristics, the presence or absence of cardiovascular risk factors and risk factor management were collected by a trained research nurse who interviewed and examined the patients at the outpatient clinic at least 6 months after hospital admission. Data collection was approved by the medical ethics committees of participating centres and all patients gave informed consent.
At the time of the interview, patients were asked whether they were smoking, and concentration of carbon monoxide in breath was recorded in ppm (Smokerlyser, Bedfont Scientific, UK, model EC 50). Height and weight were measured in light indoor clothes without shoes. Blood pressure was measured twice on the right upper arm in a sitting position by use of an automatic digital sphygmomanometer (Omron 711; Matsuzaka, Japan), and the mean of both measurements was used in the analyses. Venous blood was drawn for measurement of cholesterol concentrations in serum. Serum samples were stored at a minimum of −20 °C and transported frozen to the central laboratory at the Department of Medicine, University of Manchester, UK, where total cholesterol measurements were done on a Cobas Mira S auto-analyser (Roche Diagnostics, Switzerland) with Unimate 7 (Roche) cholesterol reagent. Physical activity was measured with one question: ‘Which of the following four best describes your level of activity outside work? (Please consider getting to and from work, sporting activity and other physical effort during your leisure time, like gardening or dancing): (1) No physical activity weekly; (2) Only light physical activity in most weeks; (3) Vigorous physical activity at least 20 min once or twice a week (vigorous activity causes shortness of breath, a rapid heart rate, and sweating); (4) Vigorous activity for at least 20 min three or more times per week’.
To assess whether patients were informed about their cardiovascular risk factors and possibilities to reduce their risk on cardiovascular events, and to determine who provided the information on management of their risk factors, patients were asked to answer the following questions: ‘Were you offered any personal advice about stopping smoking by a doctor or other health care worker?’; ‘Have you ever been told by a doctor or other health worker that you have high blood pressure/have to lose weight/have a high blood cholesterol?’; ‘Are you on a special diet prescribed by a doctor or other health worker to lower your blood pressure level/blood cholesterol level?’; ‘Are you taking (in the last 2 weeks) pills or other medicine prescribed by a doctor to lower your blood pressure/blood cholesterol level?’, and patients who were informed about their cardiovascular risk factors were asked: ‘Who provided you with the information: physician, nurse, and/or other professional caregiver?’.
Statistical analyses
Descriptive statistics were used to calculate, by diagnostic category, the prevalence of risk factors, the proportion of patients that received information about cardiovascular risk factors, and the proportion of patients that were informed by physician, nurse and/or other caregiver. All statistical analyses were performed using SPSS statistical software (version 10.1).
Results
We identified 536 consecutive patients; 503 (94%) survived for follow-up. After a median period of 20 months (IQR=15–26 months) 357 patients (71% of the survivors) were interviewed and examined concerning the presence of cardiovascular risk factors and information they received on management of their cardiovascular risk factors. Data on who this information provided (physician, nurse and/or other caregiver) was collected in two of the three participating hospitals (n=307).
Prevalence of cardiovascular risk factors
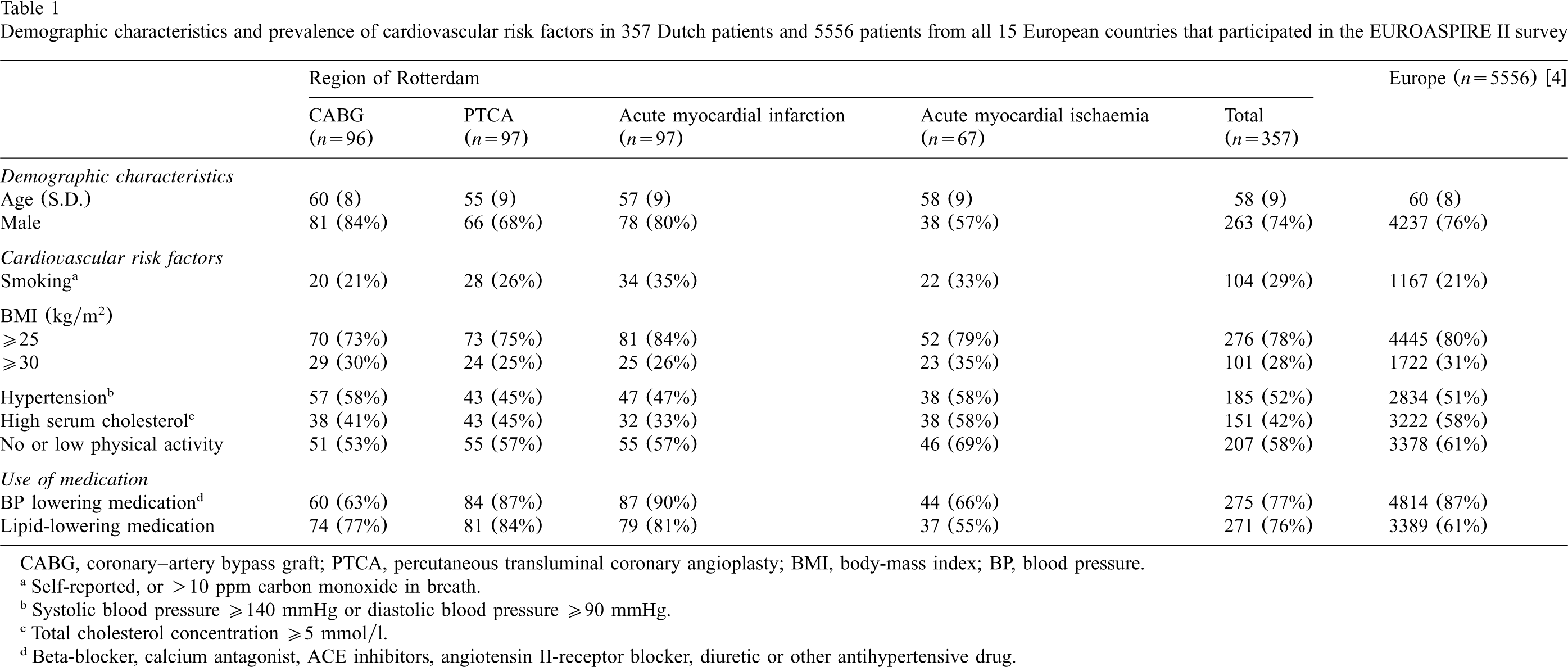
Of the 357 patients who were interviewed and examined regarding the presence of cardiovascular risk factors, mean age was 58 years (S.D. 9 years) and 74% were male (Table 1). In all, 29% were smokers, 78% were overweight (BMI⩾25 kg/m2), 52% had a raised blood pressure (systolic blood pressure ⩾140 mmHg or diastolic blood pressure ⩾90 mmHg), and high cholesterol concentration (⩾5.0 mmol/l) was observed in 42%. In addition, 58% had no or low physical activity. The prevalence of cardiovascular risk factors was highest among patients with acute myocardial ischaemia.
Demographic characteristics and prevalence of cardiovascular risk factors in 357 Dutch patients and 5556 patients from all 15 European countries that participated in the EUROASPIRE II survey
Demographic characteristics and prevalence of cardiovascular risk factors in 357 Dutch patients and 5556 patients from all 15 European countries that participated in the EUROASPIRE II survey
CABG, coronary–artery bypass graft; PTCA, percutaneous transluminal coronary angioplasty; BMI, body-mass index; BP, blood pressure.
Self-reported, or >10 ppm carbon monoxide in breath.
Systolic blood pressure ⩾140 mmHg or diastolic blood pressure ⩾90 mmHg.
Total cholesterol concentration ⩾5 mmol/l.
Beta-blocker, calcium antagonist, ACE inhibitors, angiotensin II-receptor blocker, diuretic or other antihypertensive drug.
Compared to average results on European level, the prevalence of smokers in the Netherlands was relatively high (29 vs. 21%), while the proportion of patients with high cholesterol levels was remarkably low (42 vs. 58%).
Blood pressure lowering medication (which was not necessarily taken as an antihypertensive treatment) was used by 275 patients (77%). Of these, 51% did not reach the blood pressure goal of less than 140/90 mmHg. Lipid-lowering medication was used by 271 patients (76%), but 33% of them did not reach the total cholesterol goal of less than 5.0 mmol/l. Use of both blood pressure and lipid lowering drugs was smallest (66 and 55%, respectively) in patients with acute myocardial ischaemia. The proportion of patients who did not reach the blood pressure goal of less than 140/90 mmHg or the lipid goal of less than 5.0 mmol/l, despite their use of blood pressure or lipid lowering drugs, was highest (64%) among PTCA patients and lowest (53%) among patients with acute myocardial ischaemia. Compared to results on European level, the use of blood pressure lowering drugs was lower (77 vs. 87%), while the use of lipid lowering drugs was higher (76 vs. 61%) in the Netherlands.
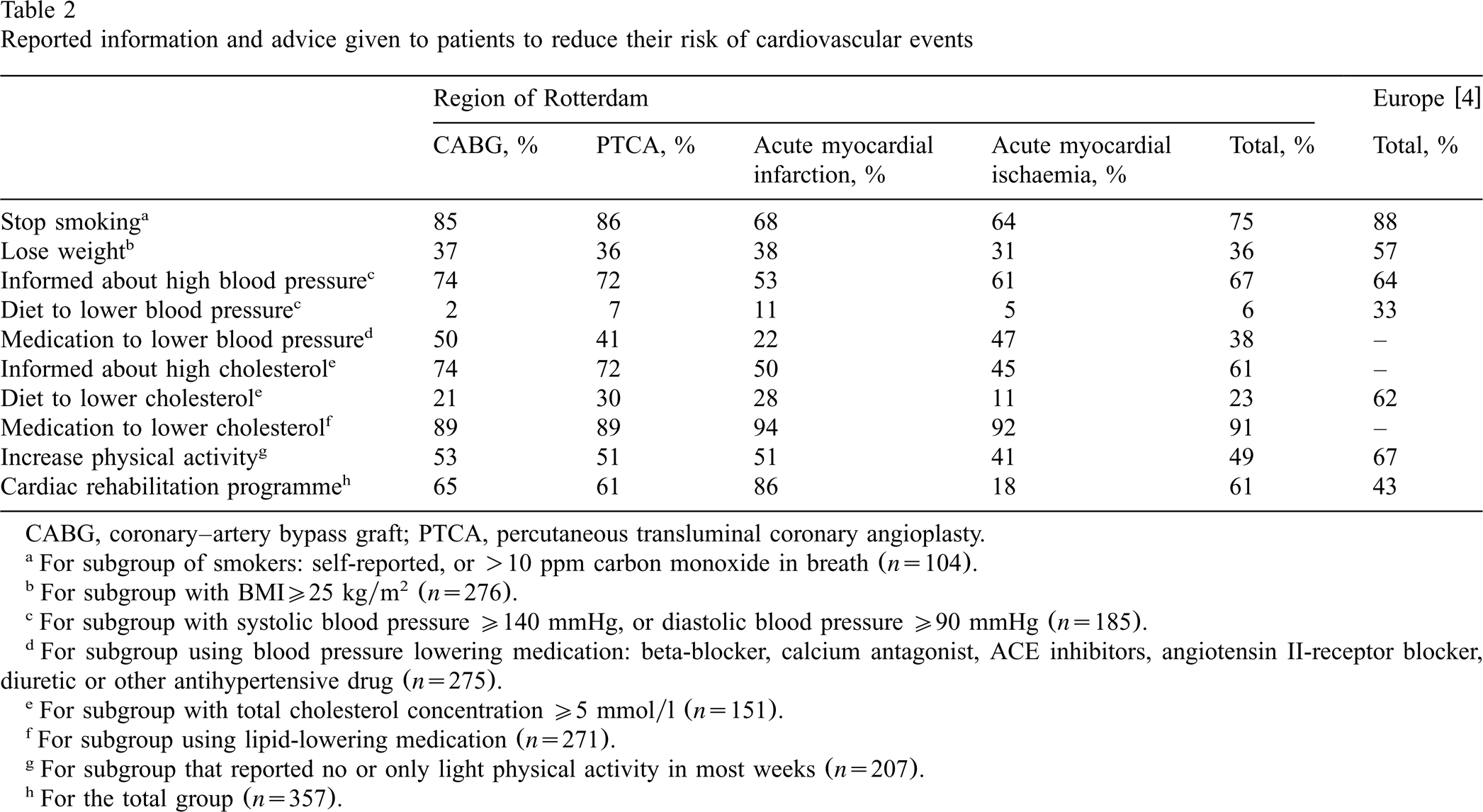
Of the 104 patients who were smokers, 75% reported that they had received advice to stop smoking (Table 2). Of those who were overweight (276 patients), 36% reported that a professional caregiver told them to lose weight. Of 185 patients with high blood pressure, 65% were informed about the presence of this risk factor, while 6% reported that they followed a diet to lower blood pressure as advised by a professional caregiver. Among those using blood pressure lowering medication (275 patients), 38% were aware of their use of such drugs. Of 151 patients with high cholesterol concentrations in blood, 61% were informed about the presence of this risk factor, while 23% reported that they followed a diet to lower cholesterol. Among those using lipid-lowering medication (271 patients), 91% were aware of their use of these drugs. Of 207 patients with no or only little physical activity, 49% reported that they had received advice to increase their level of physical activity, whereas 61% of all 357 patients were advised to attend a cardiac rehabilitation programme. The majority (88%) of those who received this advice did attend a cardiac rehabilitation programme.
Reported information and advice given to patients to reduce their risk of cardiovascular events
Reported information and advice given to patients to reduce their risk of cardiovascular events
CABG, coronary–artery bypass graft; PTCA, percutaneous transluminal coronary angioplasty.
For subgroup of smokers: self-reported, or >10 ppm carbon monoxide in breath (n=104).
For subgroup with BMI⩾25 kg/m2 (n=276).
For subgroup with systolic blood pressure ⩾140 mmHg, or diastolic blood pressure ⩾90 mmHg (n=185).
For subgroup using blood pressure lowering medication: beta-blocker, calcium antagonist, ACE inhibitors, angiotensin II-receptor blocker, diuretic or other antihypertensive drug (n=275).
For subgroup with total cholesterol concentration ⩾5 mmol/l (n=151).
For subgroup using lipid-lowering medication (n=271).
For subgroup that reported no or only light physical activity in most weeks (n=207).
For the total group (n=357).
The number of patients with one or more cardiovascular risk factor was 89 (93%) in CABG patients, 95 (98%) in PTCA patients, 97 (100%) in patients with acute myocardial infarction and 64 (96%) in patients with acute myocardial ischaemia. Respectively, 93, 84, 87 and 94% of them were not informed about at least one relevant secondary prevention item (Fig. 1). Moreover, respectively, 28, 23, 29 and 48% did not receive information about four or more relevant items. Compared to average percentages of the total Dutch group, PTCA and CABG patients were informed better on most items, with the exception of advice on diet to lower blood pressure or cholesterol (CABG patients) and awareness of use of lipid-lowering drugs (both CABG and PTCA patients). Patients with acute myocardial ischaemia, however, were informed worst about most items.
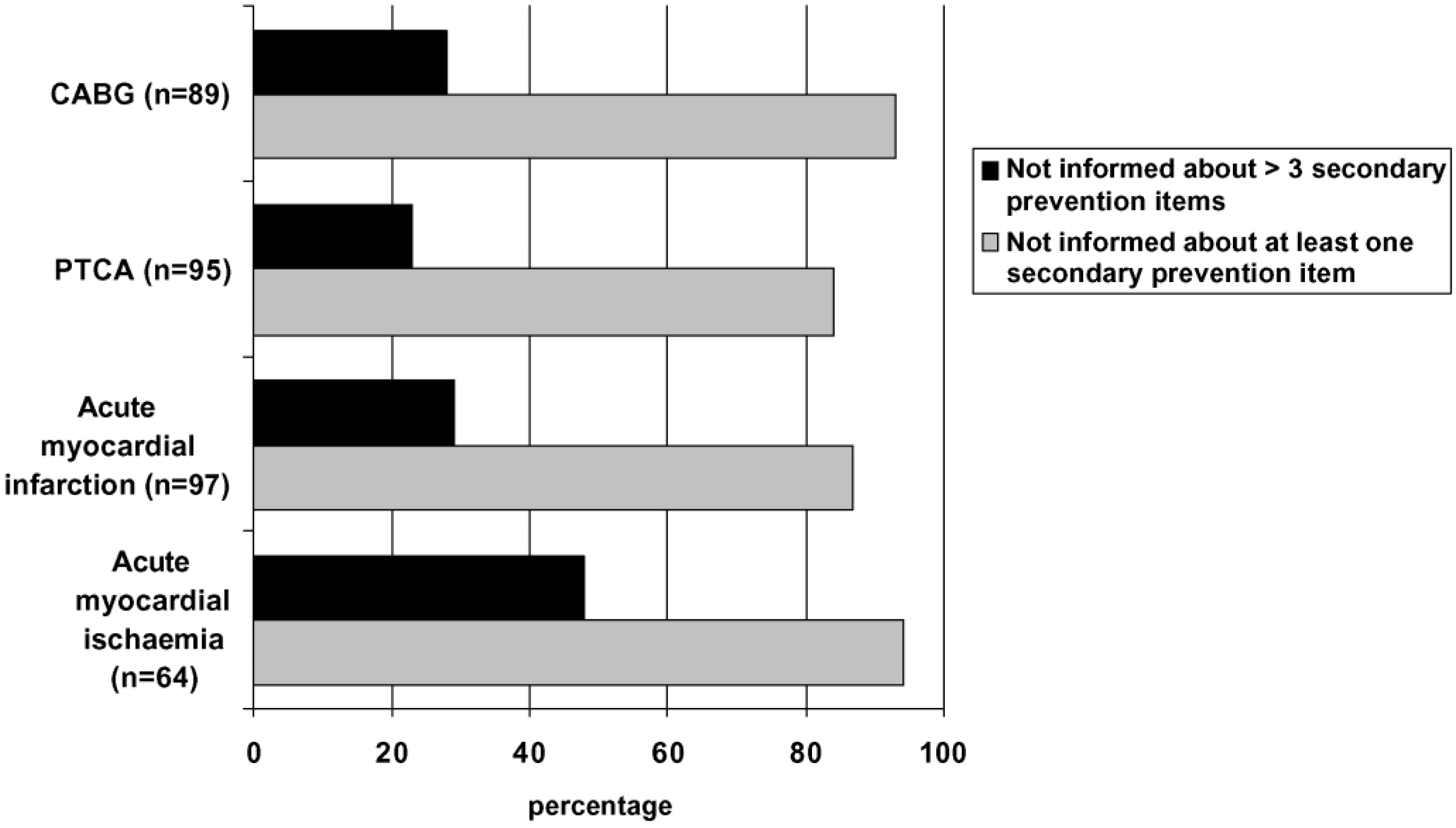
CABG, coronary–artery bypass graft; PTCA, percutaneous transluminal coronary angioplasty.
Compared to average results on European level, information and advice given to patients in the Netherlands was less for all items of secondary prevention, except for being informed about high blood pressure.
Of 66 smokers who were advised to stop smoking, 22% reported that they received this advice from nurses, while 71% were advised by physicians, and 24% by other caregivers (Fig. 2). The advice to lose weight was given to 83 overweight patients, of whom 21% received this advice from nurses, 59% from physicians, and 45% from other caregivers. Of 98 patients with a raised blood pressure and who were informed about their raised blood pressure or advised to follow a diet to lower blood pressure, most patients (59%) received this information or advice from physicians, while 23% received this advice from nurses. Information about the presence of a high cholesterol or advice to lower cholesterol by diet was provided to 80 patients with high cholesterol levels, of whom 13% received this advice from nurses, 55% from physicians, and 43% from other caregivers. Of 83 sedentary patients who received advice about increasing physical activity, 23% received this advice from nurses, 57% from physicians, and 31% from another caregiver. Compared to physicians and other caregivers, the contribution of nurses was lowest for all measured secondary prevention items, in particular regarding information about the presence of a high cholesterol level or advice on lowering cholesterol by diet. Of all 288 patients that received information regarding their risk factors, 36% was about one or more risk factors only informed by physicians while none were only informed by nurses or other caregivers.
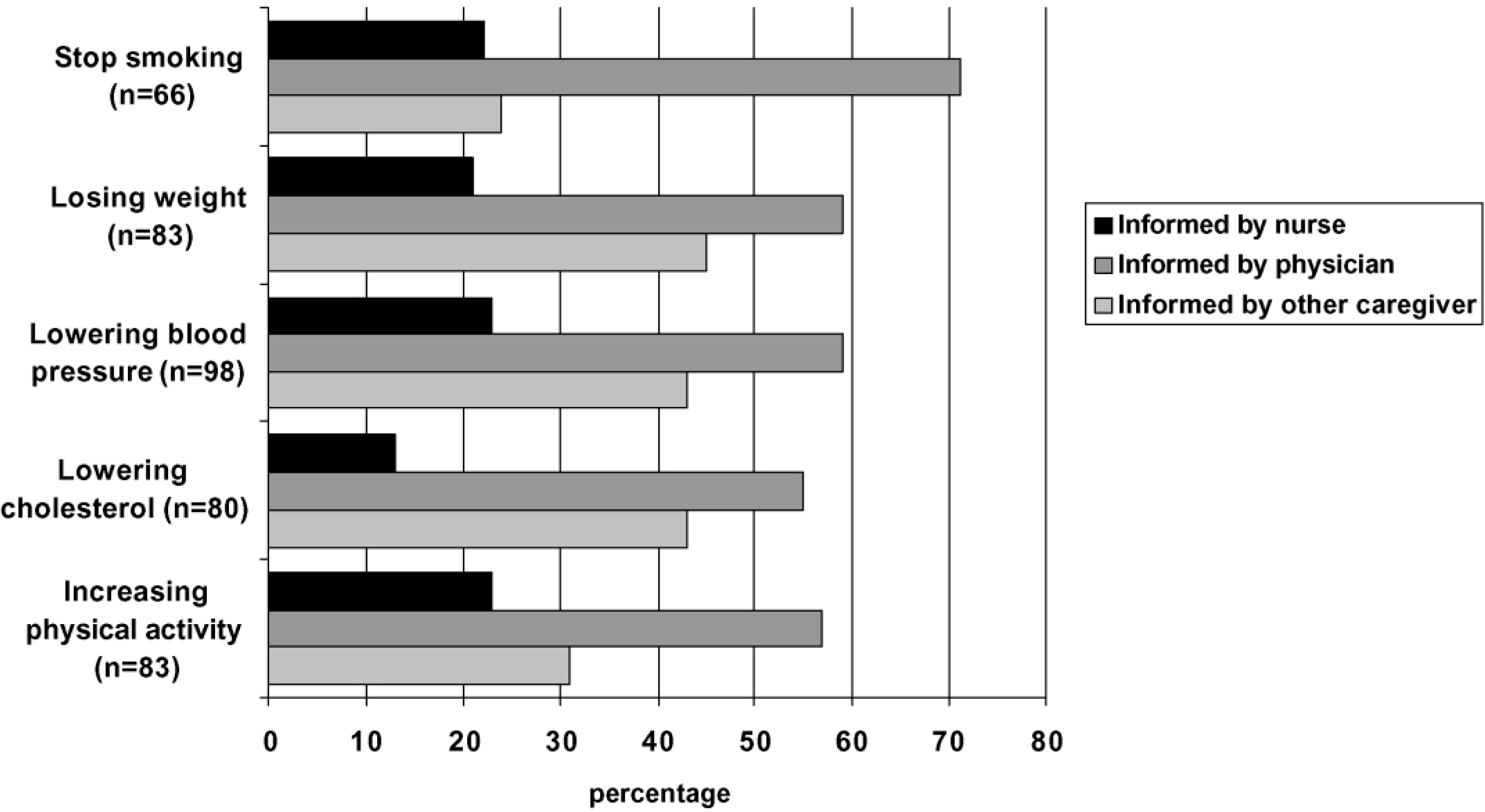
(1) For subgroup of smokers advised to stop smoking; (2) For subgroup of overweight patients advised to lose weight; (3) For subgroup of patients with high blood pressure informed about high blood pressure, or advised to lower blood pressure by diet; (4) For subgroup of patients with high total cholesterol concentration informed about high cholesterol, or advised to lower cholesterol by diet; (5) For subgroup of patients that reported no or only light physical activity, and who were advised to increase physical activity.
The number of patients with one or more cardiovascular risk factor was 88 of 95 CABG patients (93%), 86 of 88 PTCA patients (98%), 100% in 76 patients with acute myocardial infarction and 31 of 33 patients with acute myocardial ischaemia (94%). Respectively, 44, 18, 27 and 17% of them were informed by nurses about at least one relevant secondary prevention item (Fig. 3). The contribution of physicians was highest for all diagnostic categories (range 71–84%), while the contribution of nurses was lowest for all diagnostic categories (range 17–44%).
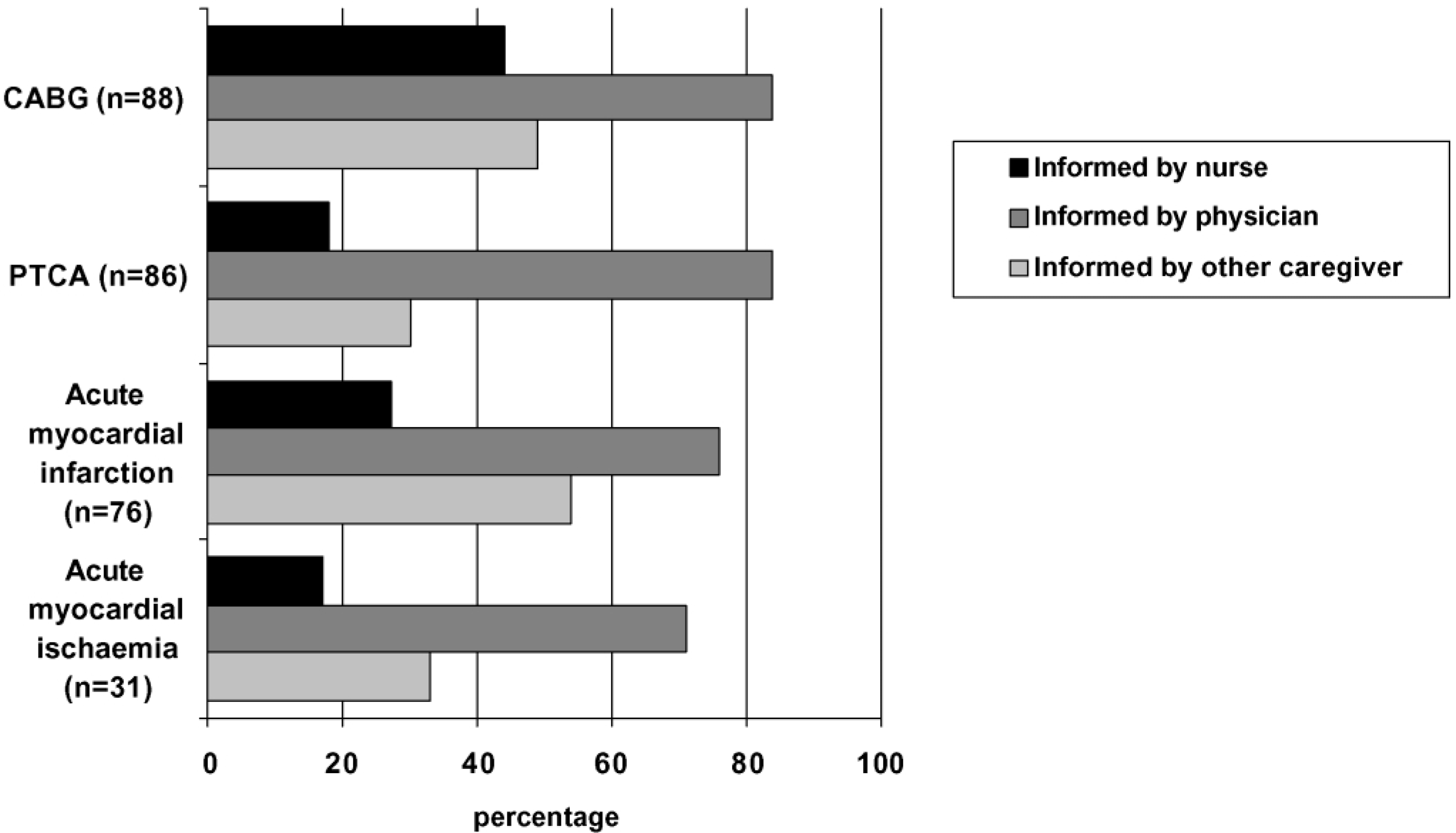
CABG, coronary–artery bypass graft; PTCA, percutaneous transluminal coronary angioplasty.
Overall, the results show a high prevalence of modifiable risk factors in patients with established CHD. In the Netherlands as well as on average in Europe, many patients at risk do not remember ever having received information about management of their risk factors. A real clinical potential therefore exists to further reduce cardiovascular morbidity and mortality. For all cardiovascular risk factors, the contribution of nurses in risk factor management as perceived by patients is small compared to the input of physicians and other caregivers. Since, guidelines and randomised controlled trials indicate that nurses can or should have an important role in risk factor management [2,9,11–13], current nursing activities in risk factor management should be reconsidered.
There is overwhelming evidence for beneficial effects of risk factor management and guidelines stress its importance in patients with established CHD [2]. However, many patients at risk, especially patients with acute myocardial ischaemia, did not remember ever having received information about the presence of their risk factors or possibilities to reduce their risk of cardiovascular events. Patients at risk may not have been identified and were consequently not informed, or none of the health caregivers informed these patients adequately. Possibly, these patients received information about risk factor management, but since they did not remember any of it, the timing or way in which information may have been provided was obviously not effective.
Although guidelines and randomised controlled trials indicate that nurses can or should have an important role in risk factor management [2,9,11–13], our results showed a relatively small contribution of nurses. The results are not that surprising if one considers the fact that a large number of patients, in the Netherlands as well as in other European countries, only have contact with nurses during their in-hospital stay. During hospital admission, of which the length has decreased tremendously during the past decades, many patients primarily focus on surviving and coping with the acute event. Awareness of risk factors, changing lifestyle, and knowledge of the purpose of prescribed drugs are perhaps items that can be more effectively addressed after hospital discharge. Like most European countries, patients with established CHD in the Netherlands are, after hospital discharge, mostly looked after by hospital cardiologists, or general practitioners, but not nurse specialists. Some patients may have contact with nurses in a cardiac rehabilitation programme, while probably even fewer patients are visited by community nurses. In view of the current organisation of clinical practice, nurses’ small contribution to risk factor management compared to the input from physicians and other caregivers is not an unexpected finding.
Considering the large number of CHD patients at risk that were not identified, not informed, not effectively medically treated, or not adequately supported in efforts to improve lifestyle, important changes in the organisation of current clinical practice may be necessary to enable successful risk factor management. A need for improvement of the identification of patients at risk and improvement of their awareness is clearly indicated by our findings. In the Netherlands as well as on average in Europe, less than 70% of patients with hypertension were informed about their elevated blood pressure and just over 60% of patients with high cholesterol were informed about this risk factor. Furthermore, many of those using blood pressure lowering drugs and some of those using lipid-lowering drugs did not reach the recommended blood pressure and lipid goal, indicating a need for improvement of patients’ follow-up. Moreover, many patients were not aware of the fact that they were taking blood pressure or lipid lowering drugs, which may have a negative influence on patients’ adherence to prescribed medication [6]. In addition, a large number of the interventions to support patients in efforts to improve lifestyle may be too comprehensive to simply incorporate in current practice. For example, our study results showed that 29% of the CHD patients were still smokers at the time of the interview. The majority (75%) of them had received the advice to stop smoking, but were apparently not successful in adopting or maintaining lifestyle change. Effective support of patients in adopting, and especially in maintaining lifestyle changes requires more than informing patients. Intensive counselling provided by specialist health professionals has proven to be more successful than a brief advice only, and is therefore strongly recommended [14,15]. To enable adequate identification of patients at risk, necessary follow up and effective support in lifestyle as recommended by guidelines, the organisational structure of current clinical practice needs to be reconsidered.
The literature offers various suggestions for comprehensive improvement of current clinical practice regarding risk factor management. Cardiac rehabilitation programmes that include the assessment and modification of risk factors, for example, proved to be successful [16–18]. Furthermore, randomised controlled trials have shown that visits to a nurse-led secondary prevention clinic every 2–6 months can be more effective, in terms of both medical and lifestyle components, than routine care from general practitioners [11,12]. Nurse-led clinics proved to be able to improve aspirin prescription, blood pressure and lipid control, dietary habits and physical activity. In addition, comparison of an audit and feedback system with audit plus a systematic recall of patients to general practitioners, and audit plus a systematic recall to a nurse-led clinic showed that the proportion of patients that were adequately assessed rose markedly during the trial in all three groups, but was more common in the nurse and general practitioners recall groups (85 and 76%, respectively) than the audit group (52%) [13]. Although these successful multidisciplinary and nurse-led interventions regarding risk factor management are organised in different ways, their common distinctiveness compared to less successful interventions [19,20] is systematic identification and follow up of patients at risk, intensive and long-term support in improving lifestyle, integrating hospital and community care, and clarity about the responsibilities of involved professional caregivers. It should be noted, however, that qualitative research about patients’ and nurses’ perceptions of nurse-led secondary preventive care revealed the need for specialist education for nurses as preparation for their role [21,22].
Currently, nurses’ role in risk factor management in the Netherlands seems to be relatively small, while risk factor management clearly needs improvement, in the Netherlands as well as in Europe. Since guidelines, randomised controlled trials as well as nurses themselves indicate that nurses can or should have an important role in risk factor management [2,9,10], nursing activities in risk factor management should be reconsidered and can only be beneficial within a largely improved organisational structure.